











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
INTRODUCTION
Various biological, psychosocial, cultural, economic and political factors converge in child development that shape changes and impact the growth of children. One of these factors that negatively impacts the emotional, mental and physical health of individuals is poverty, characterized by deprivations of basic capabilities that are not only expressed in the lack of income, but also in deficits of other dimensions that affect well-being such as malnutrition, illiteracy, barriers to access to early childhood care and health services, informal work and lack of access to drinking water, among others (Botello, 2017; Cantú & Gallardo, 2020; Bettenhausen et al., 2021; Goswami & Ghosal, 2022; Hoke & McCabe, 2022).
Children living in poor households and marginalized areas with less educated mothers are at higher risk of developmental delays (United Nations Children’s Fund [UNICEF], 2020). It is urgent to take measures to mitigate this situation since the numbers show that in 2021, 32,1 % of households in Latin America were in poverty and 13,8 % in extreme poverty (Economic Commission for Latin America and the Caribbean [ECLAC], 2022). Likewise, it is estimated that the growth of 3,6 million boys and girls from 3 to 4 years of age is not adequate for their age, 15,5 % have developmental delays and 6,2 % of children under 5 years of age present overweight (Pan American Health Organization [PAHO], 2019; UNICEF, 2020).
Poverty in Colombia has been measured through the multidimensional poverty index prepared initially by Alkire & Foster (2009) and secondly, adjusted by the National Administrative Department of Statistics to the Colombian context. From this, it is observed that the situation of multidimensional poverty in people living in populated and rural centers is 3 times higher than the municipal capitals with 37,1 %. Latin American rural areas are characterized by being areas dependent on agriculture and natural resources, with a high prevalence of poverty, isolation, and marginality, as well as state abandonment and difficulties in vital development (Rico-Ramírez et al., 2019; Gatica-Arias, 2020; Boudewijn & Jenkins, 2023). This situation reflects the contextual differences that affect the increase in single-parent homes, specifically, made up of mothers and children, and one-person homes (López, 2017), which are family structures that will shape the dynamics of childcare.
Childcare involves components that are relevant to this study, such as behavioral attitudes and care practices (Love et al., 2020; National Academies of Sciences, Engineering, and Medicine et al., 2016; Amar et al., 2016).
Regarding attitudes, they are defined from the theory of planned behavior, proposed by Fishbein & Ajzen (2010) as the degree to which a person makes a favorable or unfavorable evaluation or assessment of behavior. Likewise, attitudes integrate visions, perspectives, and ways of thinking about aspects of child´s upbringing or development, the roles and responsibilities of parents (National Academies of Sciences, Engineering, and Medicine et al., 2016).
This is related to childcare practices according to authors such as Hamilton, van Dongen & Hagger (2020) and Amini et al. (2021), who contemplate the relationship of attitudes, subjective norms, and planned behavior in the prevention practices adopted by caregivers. Thus, care practices are defined as actions carried out by primary caregivers to provide food, health care, physical and cognitive stimulation, and emotional support that guarantee the well-being of the child and the satisfaction of their physical and emotional needs (Pino et al., 2017; Lenta et al., 2020; Dos Santos et al., 2023). These practices provide levels of psychosocial functioning, self-regulation, social competencies, cognitive stimulation, and autonomy, but may be affected by adverse experiences such as child abuse or neglect, parental substance abuse, and maternal depression that hinder child development, and in some cases, they generate problematic and antisocial behaviors (Velarde & Ramírez, 2017; Bater & Jordan, 2017; Sciaraffa et al., 2018; Sanders & Turner, 2018; Andreadakis et al., 2019). These practices include activities such as smiling, hugging, talking, participating in games, which influence the creation of behavioral and eating patterns during early childhood, and allow the establishment of neural connections that strengthen the child’s brain (Lagercrantz, 2016; Nicklaus, 2017; Hofstee et al., 2022; World health Organization, 2018).
It should be noted that there is a moderating effect of environmental and contextual factors such as socioeconomic status, neighborhood, and poverty on childcare practices and attitudes, evidencing specific associations in previous studies (Stahl et al., 2018; Taraban & Shaw, 2018; Hendry et al., 2022). In addition, it has been found that familial coexistence is lower in households that live in rural areas, they are illiterate or partially literate, being more traditional and without considerable exposure to external influences, unlike provincial urban areas (Lesthaeghe, 2020). Moreover, Farkas et al. (2017), Heidari et al. (2018) have found differences between families that live in rural areas and those that live in urban areas in terms of access to health services and educational programs that provide them with information and resources, being greater in urban areas than in rural ones. Likewise, other differences found in caregivers of children from Indonesia, China, the United States and other countries respond to aspects such as emotional support, breastfeeding practices, positive parenting, and cognitive stimulation, which tend to be more favorable in urban parents and the rates of Adverse Childhood Experiences (ACEs) are lower in urban areas (Yue et al., 2019; Lu et al., 2020; Paramashanti et al., 2022).
Leavy (2019) conducted an ethnographic analysis of childcare practices in the rural context which provides valuable insights into the care provided to children in such settings. The study sheds light on the complex interplay between poverty and childcare, demonstrating that poverty in rural areas can lead to a variety of unique challenges with far-reaching consequences for children’s development. Furthermore, it has been found that caregivers with lower levels of education and with scarce economic resources have less favorable attitudes towards childcare (Stahl et al., 2018; Ma et al., 2023), and are less sensitive when correctly interpreting the signals from the child and respond effectively to them (Engbretson et al., 2023). Likewise, other sociodemographic data that influence parental attitudes are the mother´s age, the number of children, and the differences between urban and rural areas (Mesman et al., 2016; Heidari et al., 2018; Bornstein et al., 2020; Paramashanti et al., 2022; Fang et al., 2022).
Mansilla et al (2018) highlight a critical aspect of caregiving in rural areas affected by poverty: the profound impact of health problems on children’s development, and the challenges caregivers face in addressing these issues. In these resource-constrained settings, caregivers must cope not only with the economic hardships of poverty, but also with the additional burden of limited access to essential health services and resources. The lack of accessible and timely health services in rural areas can significantly hinder the identification and management of child health problems (Anoua et al., 2021; Nazareth et al., 2021). Due to geographical remoteness and inadequate health infrastructure, caregivers may face significant barriers to seeking medical care for their children. Routine health checks, early detection of health problems, and access to essential medicines may be compromised, resulting in delayed or inadequate treatment.
In this sense, understanding the sociocultural factors that characterize urban and rural environments such as exposure to situations of poverty and the lack of infrastructure and state presence, mainly in rural municipalities, leads to a greater violation of the rights of the child, which allows identifying how the context is related to the care provided to children. Thus, this study aims to analyze the relationship between poverty multidimensional poverty index and attitudes towards childcare practices in rural and urban areas of Colombia.
METHOD
Participants
In this study participated 1189 caregivers of children between 4 and 64 months from rural (83,01 %) and urban (16,98 %) areas of the Department of Atlántico. The caregivers were mainly young adults (M=28 DE=8,75). The sample consisted mainly of mothers (85,86 %), people without university education (88,97 %) and who were mainly engaged in housework (70,53 %). The income level of the majority was low (86,90 %) (see Table 1).
Table 1 Sociodemographic characteristics of caregivers.
| Relative frequency | |
| Education | |
| University Studies | 11% |
| Bachelor or less studies | 88,9% |
| Occupation | |
| Housework | 70,5% |
| Study | 6,2% |
| Work | 23,2% |
| Context | |
| Urban | 16,9% |
| Rural | 8,30% |
| Ethnic minorities | |
| Yes | 22,4% |
| No | 77,5% |
| Familiar Structure | |
| Extended | 53,7% |
| Single parent | 8,6% |
| Nuclear | 37,5% |
| Reconstituted | 0,08% |
Measures
Sociodemographic factors
A questionnaire was designed to characterize the participants in which were asked sociodemographic data such as the age of the child, the age of the caregiver, the educational level (‘Elementary’, ‘Bachelor’, ‘Technicaltechnological’, ‘Undergraduate’, ‘Postgraduate’), (‘Study’, Housework’, ‘Work’), the socioeconomic level (‘Low’, ‘Medium’, ‘High’) and the housing context (‘Rural’, ‘Urban’).
Multidimensional Poverty Index (MPI):
It was determined through the Alkire & Foster (2009, 2011) methodology, taking as a reference the model used by the DANE (2023) whose unit of measurement is the family. Poverty was measured in relation to 5 dimensions: educational conditions of the home, conditions of childhood and youth, health, work, and access to home public services and housing conditions. Each of these dimensions is evaluated based on different indicators. From the evaluation of the poverty conditions, it is identified if the household is deprived of any dimensions, and it is appreciated how extensive is said deprivation.
Table 2 Dimensions and indicators of poverty
| Dimension | Indicators |
|---|---|
| Educational conditions of the home | Illiteracy |
| Low educational achievement | |
| Conditions of Childhood and Youth | Absence school |
| Lag | |
| Barriers to access early childhood care services | |
| Child Labor | |
| Work | Long-term unemployment |
| Informal employment | |
| Health | No health insurance |
| Barriers to access health services | |
| Access to residential public services and housing conditions | Access to improves water source |
| Excreta disposal | |
| Floors | |
| Exterior walls | |
| Critical overcrowding |
Note: All dimensions have the same weight in the total poverty index.
Attitudes towards childcare
The questionnaire of attitudes towards childcare was used, which is made up of 35 items that measured the assessments of caregivers towards childcare practices on a Likert-type scale with five answer options (1 = ‘Completely disagree’, 5 = ‘Completely agree’). It contains the following dimensions of childcare: care for cognitive abilities (α = 0,90; ‘Sing to him, because it helps him learn easier’), nutrition (α = 0,82; ‹Find a way for him to eat appropriate foods for his age’), sleep (α = 0,79; ‘Let them sleep the time they need’), health (α = 0,93; ‘Take them for growth and development check-ups’), emotions (α = 0,71; ‘ Interact with them, talk to them, look at them (as) and caress them (as)’), the ethical dimension (α = 0,82; ‘They learn to respect others’) and transcendence (α = 0,91; ‘How they are raised will determine how successful they are’). For the reader´s benefit, the ethical-moral dimension refers to those values and principles that are taught during the first years of life for the formation of identity and learning to relate with respect towards others, allowing an encounter with diversity, and transcendence is related to the development of potentialities and capacities to become better, in which common well-being is sought and spaces for self-reflection and critical rationality are generated that lead to self-realization (Amar et al., 2016). It should be noted that for this study was adapted and reduced the number of items designed in the subscales of the Amar et al. instrument (2016) used to measure childcare behaviors of caregivers. This is due to the fact that this study is related to an intervention project focused on attitudes towards childcare, making it necessary to adjust the items so that they assess attitudes and not specific childcare behaviors. This new version was reviewed by expert judges and the reliability of each subscale was evaluated (see supplementary material).
Procedure
Data collection was carried out between March and September 2022, based on the physical application of the survey on childcare practices within the framework of an intervention project on childcare. The interviewers were contacted with the help of the public health administrative offices of the different municipalities. The inclusion criteria of the participants were being of legal age, being a resident of one of the municipalities where the data was collected in the Department of Atlántico, and being in charge of caring for at least one child between 0 and 5 years of age. Participants were provided with an informed consent addressing the implications of participating in the study. This study was reviewed and endorsed by the Ethics Committee of the Universidad del Norte (Ref N°198/2019).
Analysis of data
Once the data collection was completed, the missing values of the questionnaires were imputed using the Predictive Mean Matching (quantitative variables) and Logistic Regression (categorical variables) implemented in the ‘mice’ package in R (R Core Team, 2022). Next, the reliability of the psychometric questionnaires of the study was evaluated from the calculation of Cronbach’s Alpha using the functions of the ‘psych’ package (Revelle, 2022) and the confidence intervals of the Alpha were estimated using bootstrapping techniques with one thousand random sub-samples. The 0,25 and 97,5 percentiles were used to determine the confidence interval. The calculation of the scores in the care practices was carried out with the weighted average of the answers of each caregiver. In this study, linear regression analysis was performed to achieve the objective. Statistical analyzes were performed using the total poverty index.
RESULTS
In general, the descriptive results of the participants generated high scores in the dimensions of attitudes towards childcare: cognitive care (M=4,41, DE=0,58), care in food (M=3,96, DE= 0,65), sleep care (M=4,41, DE=0,66), health care (M=4,59, DE=0,58), ethical care (M=4,51, DE=0,55), emotional care (M=4,41, DE=0,60), and transcendence (M=4,61, DE=0,59), which would indicate comprehensive care and the use of strategies that guarantee the satisfaction of children’s needs in these dimensions.
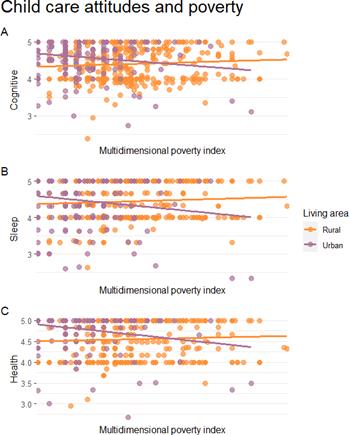
For its part, the regression analysis showed that caregivers in the urban context, compared to those in the rural context, have more positive attitudes about caring for cognitive abilities, nutrition, physical health, ps <0,001, ethical-moral development, p = 0,010 and emotional, p = 0,015, and transcendence, p = 0,020. However, no statistical evidence was found to support the relationship between attitudes towards infant sleep care with the caregiver’s context, p = 0,052.
No significant relationships were found when the multidimensional poverty index was compared to each of the attitude’s subscales regarding childcare, ps > 0,05. On the other hand, when the interaction between the multidimensional poverty index and the context was assessed, the findings showed only minor effects. It was discovered that caregivers from urban areas with high multidimensional poverty indices had fewer positive attitudes toward childcare than caregivers from rural areas with the same situation. These impacts were specifically significant for attitudes regarding cognitive care, p = 0,023, sleep, p = 0,018, and health, p = 0,028, respectively.
Table 3 Regression betas
| POVERTY | URBAN | POVERTY X URBAN | |
|---|---|---|---|
| Cognitive | 0,002 (0,001) | 0,296*** (0,085) | -0,007* (0,003) |
| Nutrition | 0,000 (0,002) | 0,398*** (0,095) | -0,006 (0,004) |
| Sleep | 0,001 (0,002) | 0,192 (0,099) | -0,009* (0,004) |
| Health | 0,000 (0,001) | 0,320*** (0,086) | -0,007* (0,003) |
| Ethical | 0,000 (0,001) | 0,216* (0,084) | -0,003 (0,003) |
| Emotion | 0,003 (0,001) | 0,215* (0,088) | -0,006 (0,003) |
| Transcendence | 0,002 (0,001) | 0,203* (0,087) | -0,006 (0,003) |
p* < 0,05, p** < 0,01, p*** < 0,001. Standard error in parentheses.
DISCUSSIONS
This study investigated the relationship between poverty and attitudes that caregivers have towards childcare practices in rural and urban areas in northern Colombia. The results showed that rural areas present more favorable attitudes towards the care of cognitive abilities, nutrition, physical health, ethical-moral and emotional development, and transcendence compared to urban areas of lower socioeconomic strata. This is consistent with research conducted in cross-cultural samples that found that attitudes of caregivers in urban areas are related to greater well-being in childcare (Yue et al., 2019; Lu et al., 2020; Paramashanti et al., 2022).
Based on the above, it can be argued that caregivers’ attitudes towards childcare practices are influenced by the prevailing conditions. Previous studies on economic conditions, parental stress and interculturality (Farkas et al., 2017; Stahl et al., 2018; Heidari et al., 2018; and Ma et al., 2023) in urban contexts have shown that there are greater educational guarantees, which provide parents with better access to knowledge about childcare and a deeper understanding of child development. Conversely, mothers living in rural areas of Colombia tend to experience greater territorial isolation, making it difficult for them to access institutional support networks for childcare.
Regarding sleep care, it was found that there were no significant differences according to the context, which differs from what was reported in samples from Portugal (Silva et al., 2013) in which no differences were observed according to population density in sleep habits in children from 1 to 6 years old who live in urban and rural areas. Various investigations on sleep habits in early childhood (Gupta et al., 2016; Alfonso et al., 2022; Zhao et al., 2022) have found differences in sleep problems and quality of preschool children living in rural and urban contexts, in which technological, biological, social and spatiotemporal factors converge, having high and low scores that do not depend solely on the area in which one lives. As a result, sleep care refers to a multifactorial study in which it is necessary to consider other conditions, characteristics, and factors that are common to these groups and independent of whether they reside in an urban or rural context.
No significant relationships were found when comparing the multidimensional poverty index with any of the childcare attitude subscales. This contrasts with findings from other studies (Stahl et al., 2018; Miller et al., 2019; Ma et al., 2023) that show how socio-economic factors influence caregiving practices. For example, lower family income is associated with less favorable caregiving practices and increased exposure of children to stressful factors that hinder their development. However, in this study the multidimensional poverty index measures basic living conditions, suggesting that caregiving practices may not be explained by these conditions alone. In addition, it is important to note that this study assessed attitudes toward caregiving, which may not always correspond to the actual behavior of the caregiver.
Therefore, it is understood that urban areas are not homogeneous among themselves, because some inhabitants of these do not enjoy the same benefits, conditions, and opportunities as those who live in slums or marginal areas. Thus, both marginal urban areas and rural areas present significant disadvantages in terms of reproductive health, living conditions, isolation, territorial exclusion, and a higher proportion of young mothers and households with several children (Mesman et al., 2016; Heidari et al., 2018; Bornstein et al., 2019; Paramashanti et al., 2022; Fang et al., 2022).
On the one hand, these findings contrast with some studies (Whiteside-Mansell et al., 2019; Lu et al., 2020; Wang et al., 2022) that suggest that rural families are at higher risk of experiencing adverse situations related to violence, abuse, parental separation and parenting challenges, and that these challenges negatively affect children’s development (Leavy, 2019). In addition, these studies suggest that rural families may experience less parental supervision and attention to their children, which may have a negative impact on attitudes towards childcare. Conversely, some research is consistent with the findings of this study (Niemistö et al., 2019; Bijnens et al., 2020) by identifying characteristics of urban environments that may have adverse effects on care practices, particularly cognitive care. For example, urban settings may emphasise academic stimulation, but restrict children’s play spaces to the home due to safety concerns. In contrast, rural areas may offer children access to larger play areas and opportunities to socialize with other children, promoting greater social development and motor stimulation.
In this way, the attitudes of caregivers in urban areas with higher poverty rates are affected by contextual stressors such as violence, crime, lack of social support, and poverty, in which imaginary lines of exclusion and marginalization are built. As has been observed in families that live in slums and belong to ethnic groups such as Afro descendants, they are exposed to complex urban dynamics such as discrimination and extreme poverty, which makes children more prone to adverse experiences such as sexual, physical, and emotional abuse and physical neglect (food insecurity) (Miller et al., 2019). Thus, the relationship between poverty and the attitudes of caregivers towards care practices differ depending on where they live, whether in urban or rural areas.
This study enabled an approach to the attitudes about childcare from a wide sample of caregivers from rural and urban areas. However, some limitations stand out. The measures in this study were generated from self-reports, which are susceptible to high social desirability. Likewise, attitudes towards care were recorded in a Likert-type format, so different care guidelines that could be relevant to the sample were surely omitted.
It is necessary that future studies implement other data collection techniques, such as direct observation, interview techniques, and triangulation to reduce such biases. Finally, future studies should explore whether the number of children, the mother’s age, and family structure influence care practices, since these variables could have a negative impact on care practices, since adolescent mothers and households with several children present care practices that could hinder children´s development due to the lack of personal resources for upbringing, as well as the overcrowding to which they would be exposed.
CONCLUSIONS
This study, conducted in both rural and urban areas of northern Colombia, sheds light on the relationship between poverty and caregivers’ attitudes towards childcare practices. The results suggest that compared to urban areas with lower socioeconomic status, rural areas have more favorable attitudes towards various aspects of childcare. These findings are consistent with previous cross-cultural research that suggests that the attitudes of caregivers in urban areas are associated with greater well-being in childcare.
The main findings also suggest that living conditions have a significant impact on caregivers’ attitudes towards childcare practices. In urban areas, there are more educational resources and institutional support. These are likely to contribute to caregivers’ better understanding of child development and childcare. In contrast, rural caregivers may face challenges due to limited access to institutional networks and resources, leading to more isolated childcare practices. Interestingly, the study found no significant differences between urban and rural areas regarding sleeping arrangements. This finding contrasts with previous studies from other countries, suggesting that sleep care may be influenced by multiple factors beyond the rural-urban context.
In addition, the findings challenge some common assumptions about rural and urban contexts. While some studies suggest that families living in rural areas face more significant risks related to violence and parental challenges, this study shows that rural environments may offer more opportunities for socializing and motor stimulation, which benefits children’s development.
To summarize, the study shows that the relationship between poverty and carers’ attitudes to childcare practices varies according to the geographical context, whether urban or rural. Urban caregivers with higher rates of poverty may face contextual stressors that have a negative impact on their attitudes, whereas rural caregivers have more positive attitudes despite the challenges they may face.
LIMITATIONS Y RECOMMENDATIONS
As with any study, there are limitations. These include the use of self-report measures and the omission of certain childcare guidelines. Future research should explore other data-gathering techniques to reduce bias and examine the potential influence of factors such as number of children, maternal age, and family structure on childcare practices.
IDEAS CLAVE (HIGHLIGHTS)
Rural areas have more favorable attitudes toward caring for cognitive abilities, nutrition, physical health, ethical-moral and emotional development, and transcendence compared to urban areas of lower socioeconomic strata.
Caregivers in urban areas with high multidimensional poverty index (MPI) have less favorable attitudes toward cognitive, sleep, and health care than rural areas with high MPI.

