











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
In late 2019, a new condition caused by SARS-CoV-2 was reported in Wuhan, China, causing a global pandemic problem1,2. Autopsies of patients who died from COVID-19 identified that the virus invades mainly the lungs, but also affects the cardiovascular system, the liver, the kidneys, and the coagulation system3. Reported data on morbidity and mortality from COVID-19 in hospitalized patients indicate that 80-85% present asymptomatically or with mild or moderate symptoms, 10% with severe infections, and half of the 5% of critical cases resulted in death4,5.
These data indicate that the severity or mortality rate is low; however, the World Health Organization (WHO) surveillance reports identify that the age distribution of COVID-19 cases is between 25-64 years of age, presenting a higher risk with 64% infection, followed by the third group between 65-84 years of age with a risk of 19.4% of cases6. During the pandemic, various international organizations, such as the American College of Sports Medicine (ACSM), the American Heart Association (AHA) and the WHO, recommended regular exercise at moderate intensity to maintain physical and psychological health7,8.In addition, physical exercise is an important immune system booster2, and although the risk factors associated with severe disease by COVID-19 are still being studied, there is increasing and consistent evidence of the relationship between physical inactivity and an increased risk of severe outcomes, i.e. hospitalization, intensive care unit admission, and/or death, similarly, patients who participated in aerobic and resistance training had a low risk of infection9. However, the training load dose and its response to the effort performed, as well as the most appropriate exercise modality, are not detailed10,11.
These elements are key considering the potential effect on patient health, which could put at risk a population deconditioned by physical inactivity and nutrition by excess, lack of supervision, and reliance on self-regulation to exercise that could increase the risk of cardiovascular events, alteration of the musculoskeletal system, and a potential immunosuppressive effect when intensity and recovery are not controlled12,13.
Therefore, when prescribing physical exercise, the following components should be carefully controlled: frequency, intensity, duration of each prescribed session and, above all, the modality of the exercise to be performed; i.e., endurance or resistance or both (concurrent)14,15. The endurance training mainly emphasizes a prolonged time at a lower intensity of execution, while resistance training, emphasizes high intensities and limited time with respect to resistance exercise and concurrent training involving the aforementioned modalities16.
These aspects are key when selecting the dose of physical exercise and its physiological contributions according to the individual needs of each person17. Therefore, this review aims to investigate existing evidence in the last five years (January 2016 through December 2021), on the immunological response of different physical exercise modalities in the population aged 25 to 84 years, identified with the highest number of confirmed cases of COVID-19, declared in the WHO report n°198 of the World Health Organization6.
Materials and methods
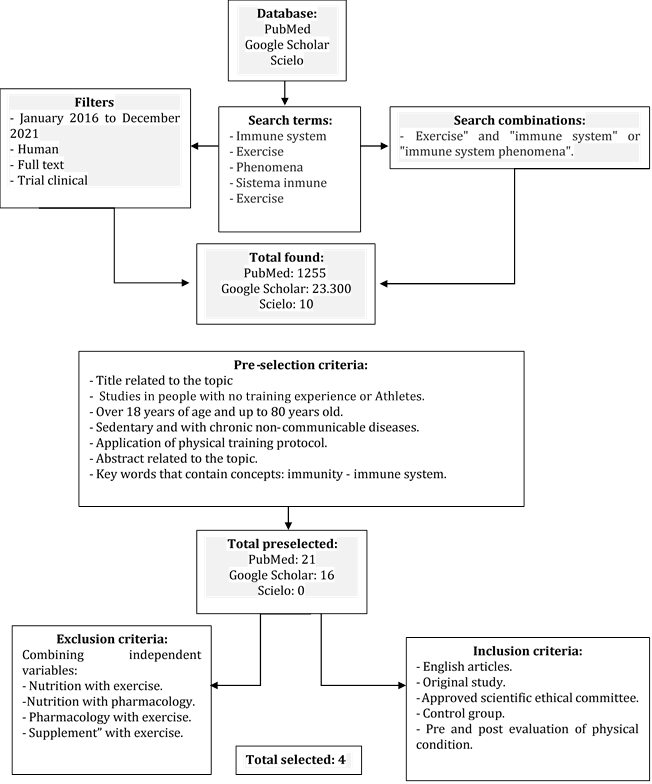
The following is a flow chart showing the methodology used to carry out bibliographic research and the steps taken to achieve it.
Results
Once the search was performed, following the steps explained above, a total of 4 articles were retrieved, all of the original scientific articles. Based on the characteristics of the selected study protocols, we were able to identify the general characteristics of the participants and the selected studies (Table 1), and the description of the exercise programs, variables, measures, and main results of the selected studies (Table 2).
Table 1 General characteristics of the selected studies
| First author/years | Main features | Age (Range in years) | Participants (n) | |
|---|---|---|---|---|
| EG | CG | |||
| Abd El-Kader & Al-Shreef18 | Healthy sedentary people | (61-67) | RS: 37 | --- |
| ≥15 minutes of physical activity no more than 2 times a week. | RS: 37 | |||
| Excluding smokers, consumption of any anti-inflammatory and antidepressant medication. | * Randomized gender distribution | --- | ||
| Bartlett et al.,19 | Sedentary with rheumatoid arthritis | (64 ± 7) | Men =1 | --- |
| No change in medication in the previous 3 months. | Women = 11 | --- | ||
| prednisone ≤5 mg / day. | ||||
| Subjects with diabetes mellitus or any cardiovascular disease are excluded. | ||||
| Broadbent & Coutts20 | Sedentary people with chronic fatigue syndrome | (18-65) | ET; (Itermittent) = 8 | 18 |
| No diagnosed cardiorespiratory problems | ||||
| No metabolic conditions. | ||||
| No recurrent problems | ET; Gradual = 8 | |||
| Hagstrom et al.,21 | Recovered from Breast Cancer (stage I-IIIA) | (51.9 ± 8.8) | ET; Cycling and regular care = 8 | 19 |
| ST: 20 | ||||
EG: experimental group
CG: control group
ET: endurance training
RT: Resistance training
Table 2 Description of the physical exercise programs analyzed and main results
| First author/years | Modality Training | Intensity | Duration | Frequency | Session duration | Instruments | Results |
|---|---|---|---|---|---|---|---|
| Ab d El-Kader & Al-Shreef(18) | Endurance | 1st stage: 60-70% HRmax | 3 months | 3 sessions/week | 40 min | Treadmill | ↓↓ TNF-α, IL-6, CD3, CD4, CD8, CD4/CD8 |
| 2nd stage 70-80% HRmax | 3 months | 3 sessions/week | 40 min | ↑↑ IL-10 | |||
| Resistance | 3 sets of 8-12 repetitions at 60% or 80% of 1RM | 6 months | Individual execution time | Pulley machines | ↓ TNF-α, IL-6, CD3, CD4, CD8, CD4/CD8 | ||
| ↑ IL-10 | |||||||
| Bartlett et al. (19) | Endurance (HIIT) | Intervals 80-90% VO2 reserve with active recovery 50-60% VO2reserve. | 10 weeks | 3 sessions/week | 30 min | Treadmill | ↓CD14/CD16, CD14/CD16 TLR2, TLR4 and HLA-DR of intermediate monocytes |
| Walking speeds range from 1-4.6 mph. | ↑ phagocytosis of monocytes from Escherichia coli | ||||||
| ↑ migration of peripheral blood neutrophils isolated from AR towards chemokine CXCL-8 | |||||||
| Broadbent & Coutts(20) | Endurance (Gradual) | Equivalent workload (w) at 50% of VO2peak or RPE 3 (1-10) | 12 weeks | 3 sessions/week | 25-30 min | Cycloergometer | ↑ counts CD3+ y CD4+, CD3-CD16+ CD56 |
| ↑↑NK expressing LAMP‐ 1 /LAMP‐ 2 | |||||||
| Endurance (Intermittent) | 1 minute at 60% of VO2 peak or RPE 4-5 alternating with 1 minute at 30% of VO2 peak or RPE 1-2 | 3 sessions/week | 25-30 min | Cycloergometer | ↑ counts CD3+, CD8+, CD4+, CD3+ CD4+ CD8 +, CD3-CD16+ CD56 +, CD19+ and CD45+ | ||
| ↑↑NK expressing LAMP‐ 1 /LAMP‐ 2 | |||||||
| Usual Care | mobilization by bicycle to the usual care center. | 3 sessions/week | Not specified | Bicycle | ↑↑ CD8+ | ||
| ↑ NK expressing LAMP‐ 1 /LAMP‐ 2 | |||||||
| Hagstrom et al,(21) | Resistance | 3 series of 8-10 repetitions al 80% 1RM | 16 weeks | 3 sessions/week | Not specified | Free weights | ↓ TNF-α in cells NK y NKT |
HRmax: Maximum heart rate.
HR: Heart rate.
1RM: 1-Maximum repetition.
RPE: range of perceived exercise.
HIIT: High-Intensity Interval Training.
TLR2: Toll-like receptor 2.
TLR4: Toll-like receptor 4.
HLA-DR: HLA Human Leukocyte Antigen System.
IL-6: Interleukin 6.
IL-10: Interleukin 10.
TNF-α: Tumor necrosis factor. NK: Natural killer cells.
Discussion
This review aimed to investigate the existing evidence in the last five years (January 2016 through December 2021), regarding the immunological response of different physical exercise modalities in the population aged 25 to 84 years, identified with the highest number of confirmed cases of COVID-19, declared in the WHO report n°198 of the World Health Organization2.
To propose appropriate physical exercise protocols for the benefit of the population between 25 and 84 years of age, identified as having the highest number of confirmed cases of COVID-19. In general terms, from the articles analyzed in relation to endurance exercise, the volume (duration) of exercise ranged from 20-40 minutes per session with intensities quantified by maximum heart rate (HRmax), Heart Rate Reserve (HRR), maximal oxygen consumption (VO2max) and Perceive Exertion scale (RPE). On the other hand, resistance exercises had a maximum duration of 60 minutes per session, whose intensity was determined based on the percentage of maximum repetition (60-80%1RM).
Specifically, focusing on the main studies, it is of interest to analyze the study by Abd El-Kader et al.18, who studied subjects older than 60 years, sedentary without comorbidities, randomly assigned to two groups exposed to both exercise modalities. One group performed moderate-intensity continuous endurance exercise on a treadmill, and the other group performed resistance exercise with pulley machines, both for the same period and number of weekly sessions. The results showed that endurance exercise was identified to contribute significantly to modulating the immune system and inflammatory markers in elderly subjects. However, resistance exercise can also be an effective method, as an alternative to a shorter endurance effort18.
Similarly, Bartlett et al.19 applied a high intensity treadmill training (HIIT) protocol to a sample of 60+ years of age. The authors found that non-classical monocytes (CD14/CD16) were significantly reduced, as were intermediate monocytes (CD14/CD16). The cell surface expression of toll-like receptors (TLR2, TLR4) and the human leukocyte antigen system (HLA-DR) of intermediate monocytes was significantly reduced. The phagocytosis of Escherichia coli monocytes was significantly increased and the migration of peripheral blood neutrophils isolated from rheumatoid arthritis to the chemokine CXCL8 was enhanced. The described HIIT protocol improved neutrophil migration precision and bactericidal functions in sedentary individuals of both sexes with rheumatoid arthritis. However, no changes were observed in inflammatory markers such as interleukin 1 β or IL-1β, interleukin 6 or IL-6, interleukin 8 or IL8 also known as CXCL-8, interleukin 10 or IL-10, C-reactive protein or CRP and tumor necrosis factor or TNF-α19.
Another study published by Broadbent and Coutts20 analyzed the effect of a gradual and intermittent endurance cycling protocol on lymphocyte cells (CD3+, CD4+, CD25+ and CD134+) counts during 12 weeks. The patients suffered from chronic fatigue syndrome (CFS) and ranged in age from 18 to 65 years. The authors concluded that weeks of training in both aerobic training modalities significantly improved CD4+ lymphocyte activation and aerobic capacity. However, they also suggested that intermittent exercise could improve patients with chronic fatigue syndrome20.
In addition, Hangstrom et al.21, conducted a resistance exercise intervention in breast cancer survivors (stage I-IIIA) whose ages ranged from 50-60 years, a resistance exercise protocol with free weight lifting was performed for 16 weeks, at a frequency of 3 times per week, at an intensity of 80% of 1RM. These changes were also correlated with an increase in lower body strength, in addition to a reduction in TNF-a, NK and NKT. No modifications were observed for changes in serum markers of inflammation. However, he found correlations between lower extremity strength gain and increased TNF-a, NK, and NKT21.
However, given the scarcity of controlled studies on physical exercise and COVID-19, future research should focus on the study of the specific effects on the immune response in patients infected with this new viral disease and determine the benefits of physical exercise in its different modalities. Therefore, it is suggested to pay attention to the correct dosage of the different modalities of physical exercise with the help of an exercise professional.
Conclusion
Based on the different protocols analyzed in the present review, resistance exercise and endurance exercise demonstrate benefits in the immune response in sedentary healthy subjects and/or those with underlying diseases. However, greater specificity and studies in patients who have presented COVID-19 are required.

