










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAquichan
Print version ISSN 1657-5997
Aquichan vol.15 no.3 Bogotá July/Sep. 2015
https://doi.org/10.5294/aqui.2015.15.3.4
How Nurses are Using the International Classification of Functioning, Disability and Health:
An Integrative Review
Cómo las enfermeras están utilizando la Clasificación Internacional del Funcionamiento, la Discapacidad y la Salud:
una revisión integrativa
Como as enfermeiras estão utilizando a Classificação Internacional do Funcionamento, da Deficiência e da Saúde:
uma revisão integradora
Diéssica Roggia Piexak1
Marta Regina Cezar-Vaz2
Clarice Alves Bonow3
Silvana Sidney Costa Santos4
1 PhD in Nursing. Federal University of Rio Grande, Brasil.
diessicap@yahoo.com.br
2 PhD in Nursing Philosophy. Federal University of Rio Grande, Brasil.
cezarvaz@vetorial.net
3 PhD in Nursing. Federal University of Pampa, Brasil.
enfcla@yahoo.com.br
4 Nursing. Federal University of Rio Grande, Brasil.
silvanasidney@terra.com.br
Received: 30 April 2014 / Submitted for peer review: 10 May 2014 / Accepted by peers: 21 May 2015 / Approved: 24 May 2015
Para citar este artículo / To reference this article / Para citar este artigo
Piexak DR, Cezar-Vaz MR, Bonow CA, Santos SSC. How Nurses are Using the International Classification of Functioning, Disability and Health: An Integrative Review. Aquichan. 2015; 15(3): 351-367. DOI: 10.5294/aqui.2015.15.3.4
ABSTRACT
Aim: The purpose of this study is to report the results of an integrative review of use of the International Classification of Functioning, Disability and Health (ICF) by nurses. This review is justified by the need for further investigation into use of the ICF in nursing, by nurses, so as to contribute to dialogue for the development of global, interdisciplinary and classification system comprehension. Methods: This integrative review included studies from 2001 to May 2015 in peer-reviewed journals. Two reviewers independently screened titles and abstracts for inclusion and completed data extraction. The papers were sourced from a number of electronic databases: MEDLINE/NML/ PubMed, Web of Science, LILACS, CINAHL and SCIELO. Results: Twenty-six articles were included. Three themes on use of the ICF were identified: clinical nursing practice; teaching nursing students and nurses; and nursing research. Conclusion: This review helps nurses to visualise how and in what care environments the ICF is being used. It demonstrates the ICF has been used specifically in the rehabilitation nursing field, but offers some evidence of its use in occupational health as well.
KEYWORDS
International Classification of Functioning, Disability and Health; nursing research; review; delivery of health care; nursing (source: DeCS, BIREME).
RESUMEN
Objetivo: el propósito de este estudio es reportar los resultados de una revisión integrativa de la utilización por parte de las enfermeras de la Clasificación Internacional del Funcionamiento, la Discapacidad y la Salud (ICF, por su sigla en inglés). Esta revisión se justifica por la necesidad de una mayor investigación sobre el uso de la ICF en enfermería, a cargo de las enfermeras, a fin de contribuir al diálogo para el desarrollo de la comprensión global e interdisciplinaria del sistema de clasificación. Métodos: revisión integrativa que incluyó estudios del 2001 a mayo del 2015 publicados en revistas revisadas por colegas. De forma independiente, dos revisores inspeccionaron los títulos y los resúmenes para su inclusión y completaron la extracción de datos. Los trabajos se obtuvieron a partir de una serie de bases electrónicas de datos: MEDLINE/NML/PubMed, Web of Science, LILACS, CINAHL y SCIELO. Resultados: veintiséis artículos fueron incluidos en el estudio. Se identificaron tres temas en cuanto al uso del ICF: la práctica clínica de enfermería; la enseñanza a los estudiantes de enfermería y a las enfermeras; y la investigación en enfermería. Conclusión: esta revisión ayuda a las enfermeras a visualizar cómo y en qué entornos de atención se está aplicando la ICF. Demuestra cómo la ICF se ha utilizado específicamente en el campo de la enfermería de rehabilitación, pero también ofrece alguna evidencia de su uso en salud ocupacional.
PALABRAS CLAVE
Clasificación Internacional del Funcionamiento, la Discapacidad y la Salud; investigación en enfermería; revisión; prestación de asistencia en salud; enfermería (fuente: DeCS, BIREME).
RESUMO
Objetivo: o propósito deste estudo é relatar os resultados de uma revisão integradora da utilização, por parte das enfermeiras, da Classificação Internacional do Funcionamento, da Deficiência e da Saúde (ICF, por sua sigla em inglês). Esta revisão se justifica devido à necessidade de uma maior investigação sobre o uso da ICF em enfermagem, sob a responsabilidade das enfermeiras, a fim de contribuir com o diálogo para o desenvolvimento da compreensão global e interdisciplinar do sistema de classificação. Métodos: revisão integradora que incluiu estudos de 2001 a maio de 2015, publicados em revistas revisadas por colegas. De forma independente, dois revisores analisaram os títulos e os resumos para sua inclusão e completaram a coleta de dados. Os trabalhos foram obtidos a partir de uma série de bases eletrônicas de dados: MEDLINE, NML, PubMed, Web of Science, LILACS, CINAHL e SciELO. Resultados: 26 artigos foram incluídos neste estudo. Identificaram-se três temas a respeito do uso do ICF: a prática clínica de enfermagem; o ensino aos estudantes de enfermagem e às enfermeiras; a pesquisa em enfermagem. Conclusão: esta revisão ajuda as enfermeiras a visualizarem como e em que ambientes de atenção está sendo aplicada a ICF. Demonstra como a ICF tem sido utilizada especificamente no campo da enfermagem de reabilitação, além de oferecer alguma evidência de seu uso em saúde ocupacional.
PALAVRAS-CHAVE
Classificação Internacional do Funcionamento, da Deficiência e da Saúde, pesquisa em enfermagem, revisão, prestação de assistência em saúde, enfermagem (fonte: DeCS, BIREME).
Introduction
The International Classification of Functioning, Disability and Health (ICF) provides a unified language and constitutes a framework for describing health and health-related states. The ICF offers definitions of functioning and disability, based on the understanding that the term encompasses all aspects of the body's functions, activities and restrictions to participation (1).
The current ICF model was approved by the World Health Assembly in May 2001, after several test versions. This model is based on the articulation of social and biomedical models, using a bio-psycho-social approach to visualise the integration of various dimensions of health (biological, individual and social) (1, 2). The concepts of the ICF introduce a new paradigm of work impairment and disability, which are determined by health conditions/illness, context (physical and social environment), different cultural perceptions and attitudes towards disabilities, and the availability of services and legislation (3).
Functionality is prioritised as a health component within the ICF, considering the environment both as a facilitator and as a barrier to performing activities and for participation. Thus, disability is the result of a series of situations and conditions that include the environment, health and personal conditions (1).
From this perspective, it is understood that healthcare professionals/nurses, along with other members of society, share responsibility in the planning and development of technology that constitutes facilitators for activities and the participation of people in different life situations. Understanding, therefore, that the performance of these people can be enhanced by environmental changes, such as physical, social and/or attitudinal, it offers different perspectives of an expanded view of health: biological, individual and social.
In the rankings of the World Health Organization (WHO), health states (including diseases and disorders) are classified according to the International Classification of Disease. The tenth revision (ICD-10) provides a structured aetiological basis. Functioning and disability associated with health conditions are classified in the ICF. Thus, ICD-10 and the ICF are complementary and provide a significant and broader view of human health, which may contribute to decision making (1).
According to WHO (1), the ICF is being used as a statistical, investigative, clinical, social and pedagogical tool. The ICF is used in clinical practice for several specialties, assisting in both assessment and decision making. Its socio-political application is evident in some countries within the framework of legislative changes or policy and social regulation. It also is used in the educational system as a conceptual framework for teaching/learning or for curricular units (4).
The number of published papers related to the ICF is increasing, but they are only evident in the areas of rehabilitation, paediatrics, care of the elderly, chronic disease, stroke, spinal cord injury and mental illness. These papers are written mainly by speech therapists, occupational therapists, physicians and physiotherapists (5).
This review is justified by the need for further investigation into use of the ICF in nursing, by nurses, to contribute to dialogue for the development of global, interdisciplinary and classification system comprehension. Clearly, the ICF is an important tool for nurses working in a number of different areas. It is, therefore, necessary to discover how it is used and how its use contributes to the work of nurses. Three study questions were defined: How is the ICF used by nurses? In what environments is the ICF being used? And, how does the ICF contribute to the work of nurses?
Aim
The purpose of the study is to report the results of an integrative review of use of the International Classification of Functioning, Disability and Health (ICF) by nurses.
Design
It is an integrative review that offers the opportunity for a comprehensive understanding of certain phenomena by analysing specific theoretical or empirical literature. An integrative review has the potential expand nursing science, informative research and practice and policy initiatives, through a synthesis of evidence (6).
Evidence can be classified hierarchically, according to the methodological approach used in studies. In this integrative review, the following classification of level of evidence was adopted: level 1 - evidence from a systematic review or meta-analysis of randomised controlled trials or evidence derived from clinical guidelines based on systematic reviews of randomized controlled trials; level 2 - evidence from at least one well delineated randomised controlled trial; level 3 - evidence from well-designed clinical trials without randomization; level 4 - evidence from cohort and case-control well delineated trials; level 5 - evidence from a systematic review of descriptive and qualitative studies; level 6 - evidence from a descriptive or qualitative study and; level 7 - evidence from the opinions of authorities and /or reports by expert committees (7). Knowledge of this evidence classification in publications related to the ICF system is crucial to be able to critically assess the results derived from these surveys, assisting in decision-making about the incorporation of evidence into clinical practice (8).
The search strategy included literature from 2001 to May 2015 found in MEDLINE/NML/PubMed, Web of Science, LILACS, CINAHL and SCIELO. The search terms were the "International Classification of Functioning, Disability and Health" and "Nursing". The inclusion criteria were: 1) full papers available electronically in MEDLINE/NML/PubMed, Web of Science, LILACS, CINAHL and SCIELO, which met the aim of the research, 2) papers published since May 2001 with the approval of the current model of the ICF by the World Health Assembly (1), 3) papers with at least one nurse among the authors, 4) summary presentation for initial examination, and 5) articles in Portuguese, English or Spanish. The items excluded were: abstracts published in proceedings, book chapters, theses, dissertations and editorials.
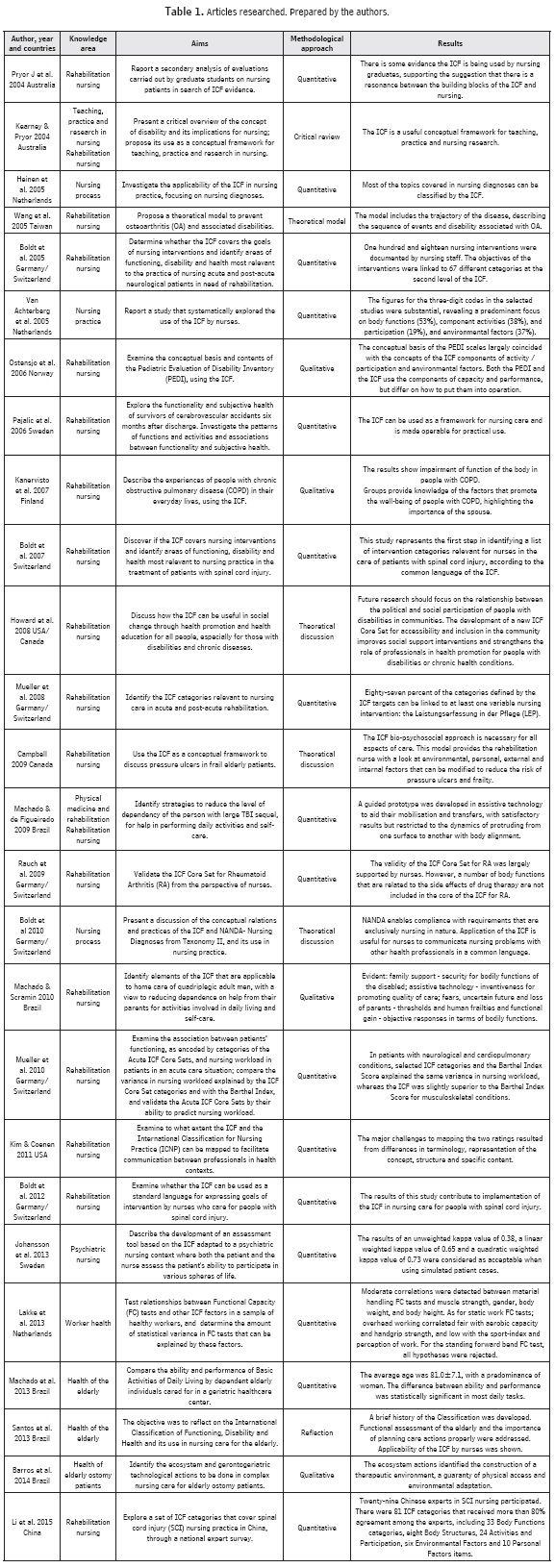
The abstracts were read and analysed in order to refine the sample and select the articles according to the inclusion / exclusion criteria. Articles repeated in more than one database were only considered once. Table 1 lists the articles and their respective databases.
The search strategy yielded a total of 130 references, many of which were duplicates. From the full analysis, a total of 26 articles were obtained: 17 from MEDLINE/NLM/PubMed, four from Web of Science, two from LILACS, two from SCIELO and one from CINAHL.
The studies were initially divided into groups, according to the methodological approach (quantitative, qualitative, theoretical discussions, critical and a theoretical model). They were evaluated independently by the lead author and a research assistant, using a quality appraisal checklist developed by Bowling (9) and modified by Desborough, et al.(10). Discussion resolved any discrepancies to reach a 100% consensus. As appropriate for an in-tegrative review, this appraisal included clarity in aims, methods, statistics, discussion and implications.
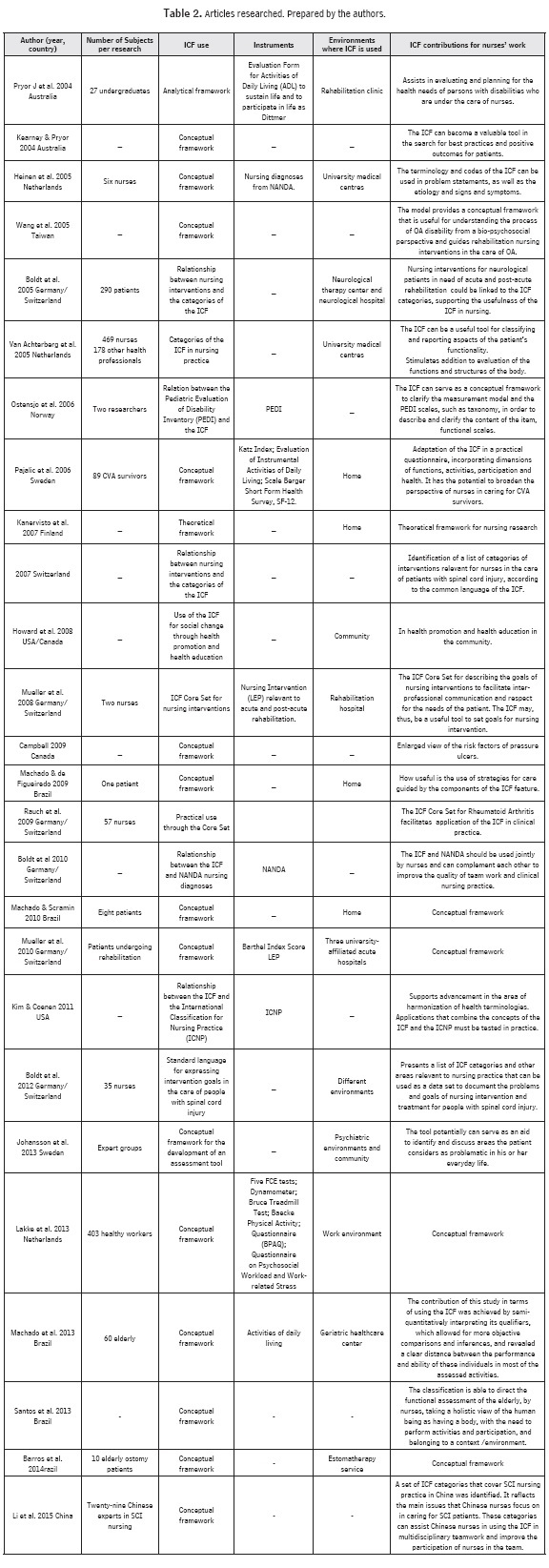
The methods suggested by Whittemore & Knafl (6) were followed for the data abstraction and synthesis. Two tables were developed to synthesise the data. Table 1 lists: author, year, country, knowledge area, aims, methodological approach, results and database. Table 2 lists: author, year, country, subject numbers, ICF use, ICF related instruments, environments in which the ICF was used and ICF contributions to the work of nurses. The format of the tables made the comparative analysis of the extracted information and patterns apparent, enabling identification of the themes.
Results
The studies originated in Germany/Switzerland (n = 6), Brazil (n = 5), the Netherlands (n=3), Australia (n = 2), Sweden (n = 2), Canada (n = 1), the USA (n = 1), the USA/Canada (n = 1), Finland (n = 1), Norway (n = 1), Switzerland (n = 1) and Taiwan (n = 1). The articles are dated between 2004 and 2015, with the largest number of publications in 2005 and 2013.
The principal authors of the publications are: Boldt C, with seven publications and Stucki G, with five. Most of the papers appeared in the following journals: Journal of Advanced Nursing (n = 5), with an impact factor of 1.477, and Disability and Rehabilitation (n=4), with an impact factor of 1.498 (11). Sixteen were quantitative, four were qualitative, three were theoretical discussions, one was critical, one was a theoretical model and one was reflective. Regarding the strength of the evidence, twenty articles (76.92%) were evidence level 6 and six articles (23.07%) were evidence level 7. Seventeen articles presented research subjects and seven of these were conducted with patients, six with nurses, two with expert groups, one with undergraduate students, and one with healthy workers. The subject numbers in the studies ranged from one to 469.
Defining Themes
Three themes were identified from the literature review: ICF use in clinical nursing practice, ICF use in teaching nursing students and nurses, and ICF use in nursing research.
ICF Use in Clinical Nursing Practice
Evidence showed there are attempts to apply the ICF in clinical nursing practice in fourteen selected articles (12-26). In most articles (n = 9), ICF application in clinical practice is defined in the Rehabilitation Nursing area (13, 15-21, 26), directed primarily to nursing interventions (n=4) with patients in acute and post-acute situations requiring rehabilitation (13, 17) and patients with spinal cord injury (16, 21, 26).
The study by Boldt (13), which sought to determine if the ICF covers the goals of nursing interventions and to identify areas of functioning, disability and health most relevant to nursing practice, found that one hundred and eighteen different nursing interventions were documented. For each intervention, nine ICF categories were identified. Nursing intervention goals were linked to 67 different ICF categories at the second level. Of the 67 categories, 30 belong to the component Body Functions, 19 to the component Body Structures, 13 to the component Activities and Participation, and five to the component Environmental Factors. All registered nursing interventions could be related to at least one ICF category.
Mueller et al. (17), who identified the ICF categories relevant to nursing care in acute situation and post-acute rehabilitation, showed eighty-seven percent of the categories defined by the ICF may be related to goals of at least one variable of nursing intervention. The nursing interventions that were linked to the highest number of different ICF-categories were "therapeutic intervention", "patient-nurse communication/ information giving" and "mobilizing".
These results suggest the ICF is relevant to Rehabilitation Nursing attempts to relate nursing interventions to the codes of the ICF through the development of Core Sets, which can provide viable inter-professional communication, maintaining the patient's needs as a priority. Thus, the ICF can be a useful tool to define nursing intervention goals (17).
In seeking evidence of whether the ICF covers nursing interventions and identifies the areas of functioning, disability and health most relevant to nursing practice in the treatment of patients with spinal cord injury, the study showed this initiative represented the first step towards identifying a list of categories relevant to nurses caring for patients with spinal cord injury intervention, according to the language of the ICF (16). This fact has stimulated research in this respect.
This is demonstrated in a study that shows implementation of the ICF helps in the care for people with spinal cord injury, identifying 823 responses that have been linked to 143 ICF categories (21).
The ICF use creates a data set that allows nurses to compare their contributions to patient care with those of other health professionals and on an international basis. However, the authors suggest future research should be conducted to confirm the usefulness of this set of data in clinical practice and to contribute to the process of ICF updating (21).
Such evidence of the ICF in clinical nursing practice, which confirms the identification of its use, has been developed mainly in the field of Rehabilitation Nursing. It is notable among these studies, particularly the study by Machado & de Figueiredo (18), that an assistive technology was planned and developed through the ICF framework to reduce the level of dependency and to assist in the performance of daily activities and self-care for patients with large brain traumatic injury.
Two studies conducted at the University Medical Center showed the applicability of the ICF in nursing, with a focus on processes/nursing diagnoses according to the North American Nursing Diagnosis Association (NANDA) Taxonomy II Nursing Diagnoses, their conceptual relations and their use in clinical practice (12, 14). It was found that the vast majority of topics addressed in nursing diagnoses can be classified by the ICF and that more identified codes were related to the Body Functions and Activities components (12).
To systematically explore ICF use for clinical nurses, it was found that the figures for the three-digit codes in the selected studies were substantial, showing a predominant focus on Body Functions (53%), Activity components (38%), Participation (19%) and Environmental Factors (37%) (14), demonstrating the ICF can be a useful working tool for nurses to classify and report patient functionality aspects.
It should be noted that studies concerning nursing interventions and procedures/nursing diagnoses in relation to the ICF more easily identify the Functions and Structures of the Body components than Activities and Participation and Environmental factors. This is more prevalent because the nursing care environment in these studies; namely, the hospital environment is inclined towards identifying these components. However, it is understood that nurses' visualization of all ICF components for expanded recognition of the patient's needs in rehabilitation is required.
Lakke et al. (22) showed the application of the ICF in clinical practice, unlike other selected studies. The ICF was used in connection with tests of Functional Capacity (FC) in healthy workers, thereby revealing other possible uses. The study showed that material handling FC tests were related to physical factors, but not to the psychosocial factors recorded in this study. The construction of static work FC tests remained largely unexplained. One limitation of the study was that cross sectional design is not suitable for the prediction of future work performance or future work disability.
ICF Use in Teaching Nursing Students and Nurses
From the literature reviewed, it was found the ICF contributes as a conceptual model for teaching nursing students and nurses. It also presents a comprehensive rhetoric, with numerous possibilities to contribute to nurses' work, but without a well-defined clinical practice application.
The ICF conceptual model encourages undergraduate nursing students to think comprehensively, by considering people as bio-psychosocial beings who are part of groups, such as the family and community. They have roles within these groups that influence and are influenced by these environments. In addition, the ICF model enables re-conceptualisation of the term disability, understanding it as a social, political and cultural human experience (5).
The study searched for ICF evidence in assessing patients in rehabilitation, which was carried out by graduate students in nursing. It found there is evidence of the building blocks of the ICF in the assessments. The assessments were designed using the form of daily activities to sustain life and/or participate in life. The documentation of information was found to be higher in relation to the Body Function and Personal Factors components, rather than Activities and Participation, supporting the suggestion that there is resonance between the building blocks of the ICF and nursing (27). This demonstrates a possible ICF contribution in assessing and planning of the health needs of people with disabilities who are under the care of nurses (27).
Another aspect that became evident was that the bio-psychosocial approach to the ICF is required for all aspects of care. This approach provides the rehabilitation nurse with a look at the environmental, personal, external and internal factors, which can be modified to reduce, for example, the risk of pressure ulcers and frailty in the elderly (28).
In presenting a discussion of ICF conceptual relations and practices, NANDA and their use in nursing practice, Boldt et al. (29) showed NANDA enables compliance with requirements that are exclusively related to nursing, and application of the ICF is useful for nurses to communicate nursing problems with other health professionals in a common language. For nurses, sharing knowledge with other health care workers can contribute to a broader understanding of patients' situation.
ICF Use in Nursing Research
The ICF contributes as a theoretical framework for nursing research (30-32). It could play a part in the following: expanding the attitude towards the risk factors of pressure ulcers in frail elderly patients (28); understanding the process of disability caused by osteoarthritis (33); broadening nurses' perspectives when caring for stroke survivors (15); and defining the goals of nursing intervention (17), as well as investigating the conceptual relationships and practices of the International Taxonomy of Nursing Diagnoses (29). It also contributes to the International Classification for Nursing Practice (35) and to discussions of how the ICF can be useful in furthering social change through health promotion and health education for all persons with disabilities (35).
However, five of these pieces of research (28, 29, 32, 33, 35) demonstrate results through methods with evidence level 7, which means evidence from the opinion of authorities (7). This is a weak factor for the immediate inclusion of this evidence into clinical practice. However, these findings provide insights for future research by incorporating methods that provide stronger levels of evidence. In quality analysis performed with a specific instrument (9, 10), six of the nine studies presented above reported discussions about the limitations of the study and the method used, which takes advantage of the verification of weaknesses and potential issues for further research.
Studies (17, 19) highlighted the ICF contribution to nursing research through the development of Core Sets for nursing inteventions (17) and rheumatoid arthritis (19), which may facilitate clinical practice implementation in the specific area of Rehabilitation Nursing.
The ICF can serve as an instrument to clarify the measurement model of the scales of the Paediatric Evaluation of Disability Inventory (PEDI) and as taxonomy to describe and clarify the content of the functional scales item (36). It also contributes to the construction of an evaluation tool adapted to the context of psychiatric nursing (37) and to testing the relationship between FC tests in healthy workers (22).
Discussion
The results of this integrative review show publications about the ICF were most likely to be produced by joint research teams from Germany and Switzerland (n = 6). Most of these researchers were part of WHO's ICF Collaborating Centre for Research in Germany, which has been one of the driving forces in Europe for implementation and dissemination of the ICF since 2004 and supports its pension scheme in the standings, despite initial difficulties in translating its concepts and construction (38).
The years 2005 and 2013 had the highest number of publications (n=4). Another study, which carried out a literature review on use of the ICF in 2007 and analysed 243 publications in different fields, also found the largest number of publications was in 2005 (n = 64) (39).
Most of the studies used a quantitative methodological approach. When it came to strength of evidence, twenty articles presented evidence derived from a single descriptive or qualitative study (evidence level 6) and six articles presented authoritative opinions, (evidence level 7) (7). Another relevant aspect is the number of subjects in the selected articles, which ranged from one to 469, demonstrating it is possible to conduct ICF-related research with a variable number of subjects.
The results of this study identified ICF use in clinical nursing practice, in teaching nursing students and nurses, and in nursing research, with emphasis on use of the ICF in the Rehabilitation Nursing area in 18 publications.
It is stressed that the area of rehabilitation is one of the fastest growing areas in publications related to the ICF (39), providing a common language between the disciplines of generic rehabilitation health code information. It also promotes a common basis for understanding the functional states associated with health conditions and comparing data across countries (5, 40). The results of this study have shown a growth in ICF literature on rehabilitation nursing.
Despite the fact that WHO (1) emphasizes the ICF can be used for various areas of knowledge, these results indicate such a perspective is rarely explored in clinical nursing practice, with most of the articles (n = 9) showing the specificity of clinical use in the rehabilitation area. This suggests further research should be done to explore other possibilities for ICF use, such as the study by Lakke et al. (22) who sought correlations between the ICF components with tests of FC in healthy workers. This differentiated it from many studies.
The number of ICF nursing publications is still low compared to other areas of knowledge and it is necessary for nurses to carry out more research, as the ICF now has a worldwide classification of reference for all disciplines (39). In Taiwan, for example, since 2012, the Law on Protection of the Rights and Interests of Citizens with Disabilities has required health care providers to assess the level of disability according to the ICF; this requires knowledge of the ICF on the part of nurses (41).
Use of the ICF offers opportunities for health professionals to provide standardisation between different disciplines and healthcare environments (42), assisting in the exchange of information between health professionals (43).
Most of the selected publications did not describe the physical, social and attitudinal specifications where the ICF was used and this did not, therefore, allow for a deeper analysis. Publications only stated the studies were developed in the following environments: rehabilitation clinics, neurological therapy centres and neurological hospitals, in the home, in psychiatric environments, in the community, in the work environment and at three university medical centres. According to the ICF, environmental factors have an impact on all components of functioning and disability and are organised sequentially, connecting the person's immediate environment to the general environment. Thus, environmental factors constitute the physical, social and attitudinal environment in which people live and conduct their lives (1), confirming the importance of knowledge about the environments where the ICF is used.
The area of rehabilitation nursing was the subject of the majority of the ICF papers. Therefore, it is evident we need more investment in studies that address disease prevention and health promotion through the ICF. As indicated by WHO, the ICF provides a conceptual framework for information applicable to health care personnel, including prevention, health promotion, improving participation by removing or mitigating social barriers, and encouraging the allocation of social support and facilitators (1).
In addition, further research is needed to address the contents of the ICF in relation to nursing, especially its use in patient care and the ability of nurses to write up records and specify nursing tasks. This requires expanding the ICF to include detailed knowledge of nursing in healthcare (43).
Conclusions
This review helps nurses to visualise how the ICF is being used, in what care environments and the contribution it is making. It demonstrates the ICF has been used specifically in the field of rehabilitation nursing, but offers some evidence of its use in occupational health.
The ICF also can be a useful tool for nurses' work in a number of other areas. These include education, as a conceptual model in practice, by generating a set of data that allows nurses to compare their contributions to patient care with those of other health professionals in different environments at an international level and also in research to describe the research questions and facilitate interpretation.
The advantages of use of the ICF by nurses include: advancement in utilization of a multi-professional instrument that facilitates inter-professional and world communication and can be used to compare research results in different countries; developing and making use of Core Sets in clinical practice, according to the patient's needs; helping to plan individual or collective nursing actions, considering environmental characteristics with the broadening of health/illness conceptions; and complementing conceptual models of nursing, by highlighting quantitative scores, which will serve as parameters for choices on heath/nursing interventions, as well as for assessing such interventions.
From this perspective, we suggest complementary use of the ICF with the already existing conceptual models of nursing, such as Callista Roy's Adaptation Model (44), Betty Neuman's Model (45), and Dorothea Orem's Self-Care Framework (46). These conceptual models view the person as a holistic system (44, 45) and identify nine needs: oxygenation, nutrition, elimination, activity and rest, skin integrity, senses, fluids and electrolytes, neurological function and endocrine function (44). In addition, Neuman's model considers the person as an open system in constant interaction with the environment (45), and Orem's Self-Care Theory aims to allow the person to be self-reliant (46). All these aspects are connected and described in the ICF.
Most of the selected publications did not describe the physical, social and attitudinal specifications of where the ICF was used, such as the number of patients seen per day, the number of nursing staff, size of the space, if the furniture was adapted to promote self-care and if the family and/or caregivers were present. This would provide a fuller analysis, as the ICF prioritises environmental factors, treating them as barriers and/or facilitators.
We are of the belief that more research needs to be carried out on use of the ICF, in different care settings and in different knowledge areas, to confirm the usefulness of this data in clinical practice. Such research also would help to update the ICF, ensuring the WHO classification is explicitly adapted to the needs of nurses. Moreover, there is still a need to encourage the use and dissemination of ICF studies in developing countries.
References
1. WHO. World Health Organization. International Classification of Functioning, Disability and Health: ICF. World Health Organization, Geneva, 2001. [ Links ]
2. Sampaio RF, Luz MT. Funcionalidade e incapacidade humana: explorando o escopo da Classificação Internacional da Organização Mundial da Saúde. Cad. Saúde Pública. 2009;25(3):475-83. [ Links ]
3. Farias N, Buchalla CM. A Classificação Internacional de Funcionalidade, Incapacidade e Saúde da Organização Mundial da Saúde: Conceitos, Usos e Perspectivas. Rev. Bras. Epidemiol. 2005;8(2):187-93. [ Links ]
4. Fontes AP, Fernandes AA, Botelho MA. Funcionalidade e incapacidade: aspectos conceptuais, estruturais e de aplicação da Classificação Internacional de Funcionalidade, Incapacidade e Saúde (CIF). Rev. Port. Sau. Pub. 2010;28(2):171-78. [ Links ]
5. Kearney PM, Pryor J. The International Classification of Functioning, Disability and Health (ICF) and Nursing. J Adv Nurs. 2004;46:162-70. [ Links ]
6. Whittemore R, Knafl K. The Integrative Review: Updated Methodology. J Adv Nurs. 2005;52(5):546-53. [ Links ]
7. Melnyk BM, Fineout-Overholt E. Making the case for evidence-based practice. In: Melnyk BM, Fineout-Overholt E. Evidence-based Practice in Nursing & Healthcare. A Guide to Best Practice. Philadelphia: Lippincot Williams & Wilkins; 2005. p.3-24. [ Links ]
8. Galvão CM. Níveis de evidência. Acta paul. enferm. 2006;19(2):5. [ Links ]
9. Bowling A. Research Methods in Health: Investigating Health and Health Services. Philadelphia: Open University Press; 2002. [ Links ]
10. Desborough J, Forrest L, Parker R. Nurse-led primary healthcare walk-in centres: An integrative literature review. J Adv Nurs. 2012;68:248-63. [ Links ]
11. Web of Knowledge. JCR Science Edition [Internet]. 2011 [cited 2014 Apr 07]. Available from: http://admin-apps.webofknowledge.com/JCR/JCR [ Links ]
12. Boldt C, Brach M, Grill E, Berthou A, Meister K, Scheuringer M, et al. The ICF categories identified in nursing interventions administered to neurological patients with post-acute rehabilitation needs. Disabil. Rehabil. 2005;27:431-6. [ Links ]
13. Van Achterberg T, Holleman G, Heijnen-Kaales Y, Van der Brug Y, Roodbol G, Stallinga HA, et al. Using a multidisciplinary classification in nursing: The International Classification of Functioning Disability and Health. J Adv Nurs. 2005;49:432-41. [ Links ]
14. Pajalic Z, Karlsson S, Westergren A. Functioning and subjective health among stroke survivors after discharge from hospital. J Adv Nurs. 2006;54(4):457-66. [ Links ]
15. Boldt C, Velstra I, Cieza A, Scheuringer M, Stucki G. Spinal cord injury: Identifying nursing intervention categories based on the World Health Organization's International Classification of Functioning, Disability, and Health. SCI Nurs. 2007;24(2):4. [ Links ]
16. Mueller M, Boldt C, Grill E, Strobl R, Stucki G. Identification of ICF categories relevant for nursing in the situation of acute and early post-acute rehabilitation. BMC Nurs. 2008;7:3. [ Links ]
17. Machado WCA, Figueiredo NMA. Base fixa teto/mãos: Cuidados para autonomia funcional de pessoas com sequela de lesão neurológica espástica. Esc Anna Nery. 2009;13(1):66-73. [ Links ]
18. Rauch A, Kirchberger I, Boldt C, Cieza A, Stucki G. Does the Comprehensive International Classification of Functioning, Disability and Health (ICF) Core Set for Rheumatoid Arthritis Capture Nursing Practice? A Delphi Survey. Int. J. NursStud. 2009;46:1320-34. [ Links ]
19. Muller M, Lohmann S, Strobl R, Boldt C, Grill E. Patients' functioning as predictor of nursing workload in acute hospital units providing rehabilitation care: A multi-centre cohort study. BMC Health Serv. Res. 2010;10:295. [ Links ]
20. Boldt C, Velstra IM, Brach M, Linseisen E, Cieza A. Nurses' intervention goal categories for persons with spinal cord injury based on the International Classification of Functioning, Disability and Health: An international Delphi Survey. J Adv Nurs. 2012;20. [ Links ]
21. Lakke SE, Soer R, Geertzen JHB, et al. Construct validity of functional capacity tests in healthy workers. BMC Musculos-kelet. Disord. 2013;14:180. [ Links ]
22. Pryor J, Forbes R, Hall-Pullin L. Is there evidence of the International Classification of Functioning, Disability and Health in undergraduate nursing students' patient assessments? Int J Nurs Pract. 2004;10:134-41. [ Links ]
23. Heinen MM, Van Achterberg T, Roodbol G, Frederiks CMA. Applying ICF in nursing practice: Classifying elements of nursing diagnoses. Int. Nurs. Rev. 2005;52:304-12. [ Links ]
24. Machado FN, Machado AN, Soares SM. Comparison between ability and performance: A study on the functionality of dependent elderly individuals. Rev Lat Am Enfermagem. 2013;21(6):1321-9. [ Links ]
25. Barros EJ, Santos SS, Gomes GC, Erdmann AL, Pelzer MT, Gautério DP. Ecosystemic and gerontotechnological actions in complex nursing care to the elderly with ostomy. Rev Bras Enferm. 2014;67(1):91-6. [ Links ]
26. Li K, Yan T, You L, Li R, Ross AM. International classification of functioning, disability and health categories for spinal cord injury nursing in China. Disabil Rehabil. 2015;37(1):25-32. [ Links ]
27. Campbell KE. A new model to identify shared risk factors for pressure ulcers and frailty in older adults. Rehabil Nurs. 2009;34(6):242-7. [ Links ]
28. Boldt C, Grill E, Bartholomeyczik S, et al. Combined application of the International Classification of Functioning, Disability and Health and the NANDA-International Taxonomy II. J Adv Nurs. 2010;66(8):1885-98. [ Links ]
29. Kanervisto M, Kaistila T, Paavilainen E. Severe chronic obstructive pulmonary disease in a family's everyday life in Finland: Perceptions of people with chronic obstructive pulmonary disease and their spouses. Nurs Health Sci. 2007;9(1):40-7. [ Links ]
30. Machado WCA, Scramin AP. (In) Dependência funcional na dependente relação de homens tetraplégicos com seus (in) substituíveis pais/cuidadores. Rev Esc Enferm USP. 2010;44(1):53-60. [ Links ]
31. Wang T, Chern H, Chiou Y. A theoretical model for preventing osteoarthritis - related disability. Inform Health Soc Ca. 2005;30(2):62-7. [ Links ]
32. Santos SSC, Lopes MJ, Vidal DAS, Gautério DP. International classification of functioning, disability and health: Use in nursing care for the elderly. Rev. Bras. Enferm. 2013;66(5):789-93. [ Links ]
33. Kim TY, Coenen A. Towards harmonising WHO international classifications: A nursing perspective. Inform Health Soc Ca. 2011;36(1):35-49. [ Links ]
34. Howard D, Nieuwenhuijsen ER, Saleeby P. Health promotion and education: Application of the ICF in the US and Canada using an ecological perspective. Disabil Rehabil. 2008;30(12-13):942-54. [ Links ]
35. Ostensjo S, Bjorboekmo W, Carlberg EB, Vollestad NK. Assessment of everyday functioning in young children with disabilities: An ICF-based analysis of concepts and content of the Pediatric Evaluation of Disability Inventory (PEDI). Disabil Rehabil. 2006;28(8):489-504. [ Links ]
36. Johansson C, Ástróm S, Kauffeldt A, Carlstróm E. Daily Life Dialogue Assessment in Psychiatric Care - Face Validity and Inter-Rater Reliability of a Tool Based on the International Classification of Functioning, Disability and Health. APN. 2013;27(6),306-11. [ Links ]
37. Schuntermann MF. The implementation of the International Classification of Functioning, Disability and Health in Germany: Experiences and problems. Int J Rehabil Res. 2005; 28, 93-102. [ Links ]
38. Jelsma J. Use of the International Classification of Functioning, Disability and Health: A literature survey. J Rehabil Med. 2009;41:1-12. [ Links ]
39. Eadie TL. The ICIDH-2: Theoretical and clinical implications for speech-language pathology. Int. J. Speech Lang. Pathol. Audiol. 2001;25:181-200. [ Links ]
40. Shen PY, Chen CM. The WHO's International Classification of Functioning, Disability, and Health (ICF): Essential Knowledge for Nurses. Hu Li Za Zhi. 2012;59(6):92-7. [ Links ]
41. Mrayyan MT. The influence of standardized languages on nurses' autonomy. J Nurs Manage. 2005;13:238-41. [ Links ]
42. Steiner WA, Ryser L, Huber E, Uebelhart D, Aeschlimann A, Stucki G. Use of the ICF model as a clinical problem-solving tool in physical therapy and rehabilitation medicine. Phys Ther. 2002;82(11):1098-107. [ Links ]
43. Florin J, Ehrenberg A, Ehnfors M, Bjórvell C. A comparison between the VIPS model and the ICF for expressing nursing content in the health care record. Int J Med Inform. 2013;82(2):108-17. [ Links ]
44. Roy C, Andrews HA. The Roy Adaptation Model: The Definitive Statement. Norwalk: Appleton & Lange; 1999. [ Links ]
45. Neuman B, Fawcett J. The Neuman Systems Model. 5th ed. Prentice Hall; 2010. [ Links ]
46. Orem DE. Nursing: Concepts of Practice. New York: McGraw-Hill; 1985.19 p. [ Links ]
Inicio
