











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
Cancer, a collection of over 100 diseases that have in common disordered cell growth and the ability to invade tissues and organs, is a chronic-degenerative disease, is currently considered a public health problem in both developed and undeveloped countries that affects several dimensions of human life 1. In fact, chronic non-communicable diseases are responsible for most of the world’s deaths, and cancer is believed to be the major cause, becoming the main barrier to life expectancy evolution worldwide in the 21st century. Currently, the burden of diseases associated with cancer indicates that it is the first or second cause of premature deaths (before the age of 70) in 52.9 % of the world’s countries, and 58.1 % in Latin America 2. In Brazil, cancer represents the second leading cause of death, and an estimated 600,000 new cases are expected for the 2018-2019 biennium. Some of the most prominent cancer types are located in the abdominal area, such as the colon and rectum, stomach, liver and biliary tract 3.
Cancer is a stigmatized disease, presenting repercussions in society in general, and since it is a complex disease, from diagnosis to treatment, the patient suffering from this ailment presents symptoms that permeate the physical, material and even the emotional spheres 4. Thus, symptoms presented by oncological patients comprise multiple dimensions, such as physical and psychological, and require a careful evaluation that comprises these various aspects 5. It should be noted that one symptom can influence the occurrence and the meaning of others. Patients with uncontrolled symptoms present significant losses in quality of life. Symptoms that are identified late and left untreated are directly related to changes in patient functional capacity, worsening of quality of life and repercussions in the reduction of the overall survival of these subjects. One of the clinical, diagnostic and social approaches in this context is the use of adapted scales and questionnaires. Adapted scales are an effective way of measuring certain phenomena 6.
The Memorial Symptom Assessment Scale (MSAS) was developed in 1994 with the aim of providing multidimensional information on a diverse group of physical and psychological symptoms common to oncology patients. It allows the evaluation of 32 physical and psychological symptoms and their frequency, severity and distress, through a scale of Likert-type points. In addition, this instrument provides a more comprehensive method of symptom assessment and may be useful when information on symptoms is desirable, such as clinical trials or epidemiological studies 7. Recently, it has been adapted for Brazil 8,9.
In particular, abdominal cancer encompasses a diverse group of tumors that are classified according to location, with higher colon and stomach incidences 3. Due to the diversity of affected organs and their specificities, patients with abdominal cancer may present multiple symptoms, which are likely to cause changes in physical and psychosocial structures. It is important to emphasize that patient symptoms vary according to the severity, frequency and duration of the disease 4. In this context, the aim of the study was to evaluate the symptoms presented by patients with abdominal cancer and their associated factors.
Methodology
Study design
This is a cross-sectional study that used a set of data on symptom prevalence and treatment in patients presenting abdominal tumors treated at the National Cancer Institute (INCA, for its initials in Portuguese), located in Southeastern Brazil. It welcomes patients from all over the country.
Sample
The convenience sample of this study included 100 adult subjects hospitalized between March and December 2016, equivalent to 82 % of the total patients in that period. Inclusion criteria comprised patients aged 18 years or older with abdominal neoplasias admitted to the INCA’s Cancer Hospital I (or INCA/HCI). Data collection was performed through the application of the MSAS-BR scale in the form of individual interviews, after the patients were given previous information concerning the objectives of the research, agreed to participate in the study and signed of the informed consent form. Due to the educational deficit of most of the participants, the chosen instrument consisted in an interview, replacing the self-applied questionnaire, as recommended in a previous study during the first stage of instrument validation 9. Inclusion criteria favored the participation of patients over 18 years old, presenting cancers whose primary origin was the abdomen-pelvic region, including liver, stomach, colon, rectum and pancreas, regardless of staging. The exclusion criteria comprised patients with cognitive disorders previously evaluated through the Mini-Mental exam, those in a position to compromise the veracity of the answers and individuals presenting neoplasia or metastasis to the Central Nervous System (CNS) whose information was obtained through medical records.
For the collection of additional data, a form prepared by the authors was used, including sociodemographic and clinical information, such as age, sex, marital status, educational level, race, primary diagnosis, the presence of metastasis, device use and location (outpatient or inpatient). This information was obtained through patient interviews. Another questionnaire included the Memorial Symptom Assessment Scale (MSAS). The MSAS is a 32-item evaluation tool developed to measure the prevalence of symptoms and three associated characteristics (frequency, severity and distress) concerning the physical and psychological aspects experienced by cancer patients in the week prior to the interview. Symptom scores represent the means of three dimensions, where the highest symptom scores represent higher frequency, greater severity, and greater distress. The mean frequency and standard deviation distribution for each MSAS item was obtained.
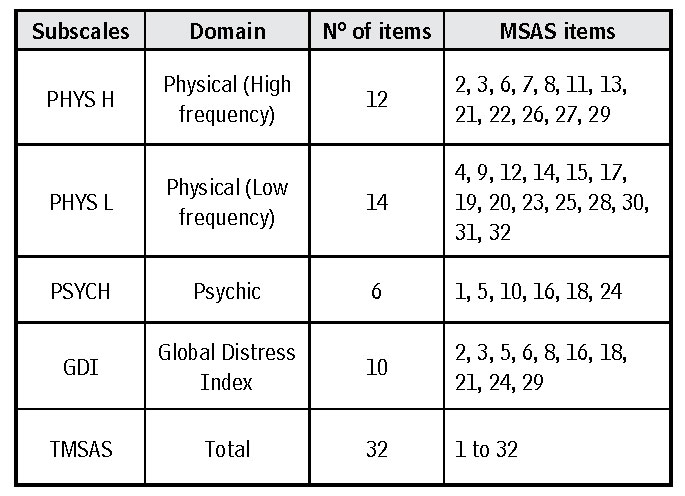
The MSAS symptom scale is further divided into subscales that assess psychological symptoms: (PSYCH), comprising six items, (PHYS H), which evaluates physical high frequency symptoms, consisting of 12 items and (PHYS L), which evaluates physical symptoms presenting relatively low frequency, comprising 14 items. A fourth subscale containing four psychological symptoms and six physical symptoms is also present, which assesses the global distress index (GDI), which may present significant variations when applied, for example, to out- and inpatients, and is considered the most useful subscale, in clinical terms. Finally, an index that consists of the means between the three domains and all items (TMSAS) was also applied. The subscales and their respective items are described in Table 1. It is important to indicate that the subscale scores represent the means of their comprising items. The MSAS reveals good results regarding reliability and validity in the cancer population, as described in previous studies. The scale reliability was satisfactory in the retest tests. The Kappa weighted index values obtained for each item of the scale ranged between 0.69 and 0.96. Regarding the subscales, the index value was of 0.84 for high-frequency physical symptoms, 0.81 for low-frequency physical symptoms, 0.81 for psychological symptoms, and 0.78 for the GDI 8.9. It is important to highlight that the scale, because it comprises an inventory, does not present a cutoff point for patient classification. Thus, its main objective is to describe symptom frequency and, when necessary, patient classification in studies are established, usually through the median presented in the surveys 9.
When a symptom is experienced, its score is determined by the mean intensity, frequency, and distress scores, or, when applicable, only by intensity and distress scores. Thus, the scores for each subscale were calculated and the association between subscales, demographic variables (sex, age, education, race, marital status) and clinical status (tumor location, the presence of metastasis, type of care and presence of any device) were evaluated. An Analysis of Variance (ANOVA) test was applied to the categorical variables and a statistical significance level of 95 % was accepted. The data analyses were performed using the SPSS Statistical Package, version 22.
Patients were approached in the abdomino-pelvic surgery ward, at a time when they were not vulnerable or in a situation that would compromise the decision to participate in the study.
Regarding ethical aspects, the study complied with the ethical and legal specifications of Resolution 466/12, of the National Health Council/Ministry of Health, which regulates research involving human beings. The study was authorized by the INCA Ethics and Research Committee (CEP), through a substantiated opinion number 863.339, on November 8, 2014, and does not involve any conflicts of interest.
Results
The study population presented a discrete male predominance (52.0 %), with little over half of the patients categorized in an age group of 60 years old or more (52.0 %). The majority (60.0 %) declared themselves white. A predominance of a high school level of education (49.0 %) was observed, with only 16.0 % of the interviewees at the university level. Regarding marital status, a higher prevalence of married individuals was noted, representing 61.0 % of the population. Considering tumor location, a higher frequency of colon tumors was observed, at 42.0 %, followed by stomach and rectum, both at 22.0 %. A total of 60.0 % of the patients did not present metastases (Table 2).
In general, concerning symptom frequency, the category representing low/medium severity was the most recurrent response of patients to most of the symptoms, when present. The most frequent symptoms were “shortness of breath” (66.7 %), “sadness” (65.8 %), “problems with sexual desire or activity” (65.0 %), “difficulty swallowing” (62.5 %) and “nervousness” (62.1 %). The less cited category was that representing low severity for most variables. Regarding intensity, the category referring to “moderate” severity was the most frequent response. The highest percentages for this category were “diarrhea” (64.7 %), “problems with sexual desire or activity” (63.2 %), “lack of energy” (58 %), “concerns” (57.3 %) and “pain” (55.9 %). Finally, with regard to distress, the prevalent category referred to average severity symptoms, with the highest percentage in this category comprising “difficulty in concentrating” (100 %), “sadness” (60.0 %), “mouth sores” (50.0 %), “itching” (50.0 %) and “dizziness” (47.4 %). The less cited category was that referring to the absence of distress (Table 3).
The most prevalent symptoms were “weight loss” (64.0 %), “pain” (56.0 %), “dry mouth” (50.0 %), “concerns” (49.0 %), “I do not seem like myself” (48.0 %) and “lack of energy” (45.0 %). The least prevalent symptoms were “itching” (12.0 %), “sweating” (11.0 %), “coughing” (11.0 %), “difficulty swallowing” (9.0 %), “difficulty concentrating” (6.0 %) and “mouth sores” (2 %). Many patients reported not having symptoms. However, among those who did severity was high, since the means of the items, whether for intensity, frequency or distress, increased considerably when analyzing the group presenting symptoms separately (Table 4).
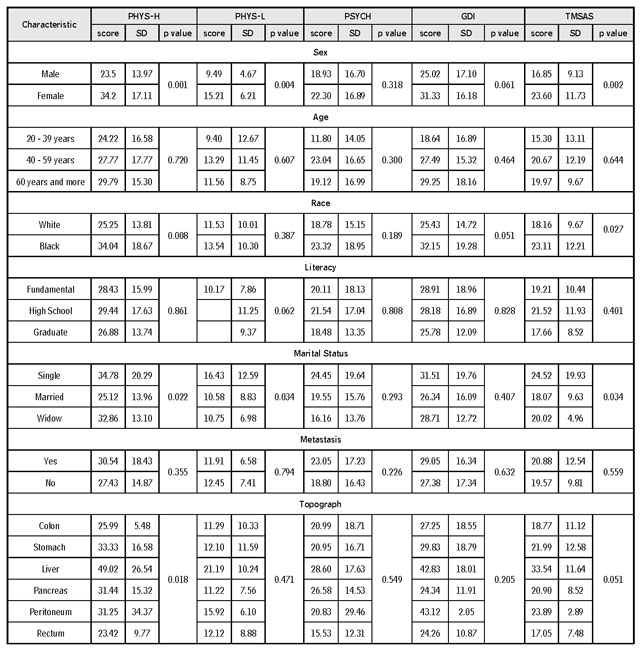
When assessing the differences in the score of total symptoms and subscales by variable category, no difference in symptom severity (totals and subscales) for age, schooling and the presence of metastasis was observed. Regarding sex, a statistically significant difference was identified for high-frequency physical symptoms (PHYS-H) (p = 0.001), low-frequency physical symptoms (PHYS-L) (p = 0.004) and for the general scale (TMSAS) (p = 0.002), with higher severity complaints among women. Concerning race, significance was observed for high-frequency physical symptoms (p = 0.008) and the general scale (p = 0.027), and borderline significance was noted for the GDI (p = 0.051), with complaints of greater severity among blacks and mulattos. Concerning marital status, statistically significant differences were found for high frequency physical symptoms (p = 0.022), low frequency physical symptoms (p = 0.034), and for the general scale (p = 0.034), with a higher complaint of severity among unmarried patients (single and widowed/separated). Finally, more frequent complaints of the severity of high-frequency physical symptoms were observed for patients with liver cancer (p = 0.018) (Table 5).
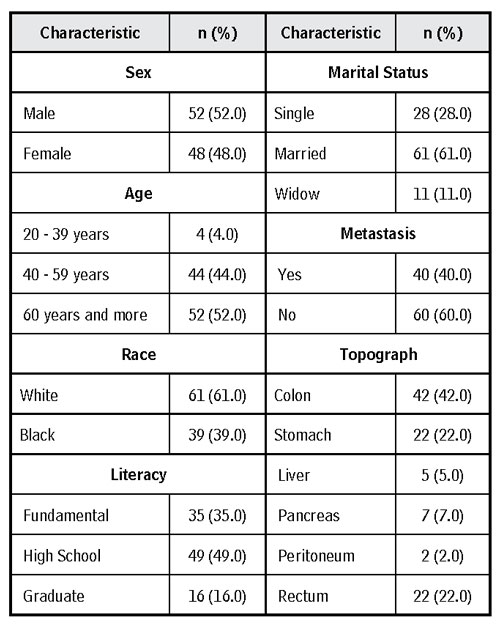
Table 3 Frequency of the MSAS symptoms concerning frequency, intensity and distress (n = 100)
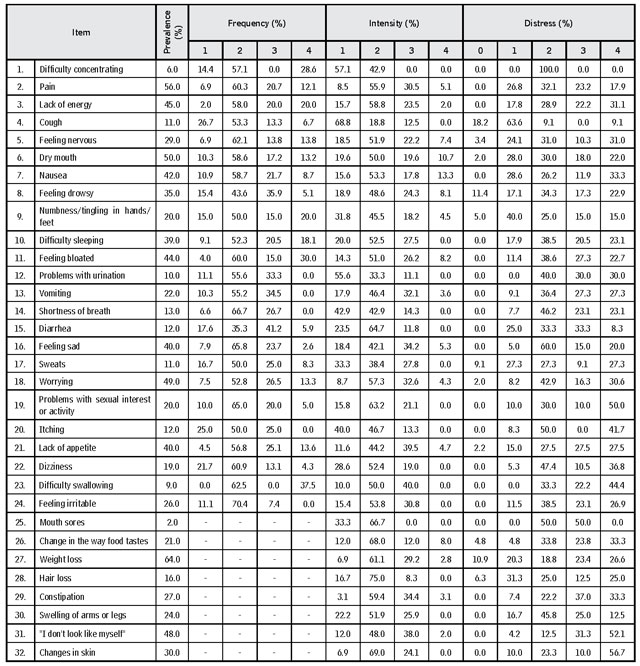
Source: Own elaboration.
Table 4 Summary of the MSAS test items statistics (n = 100)
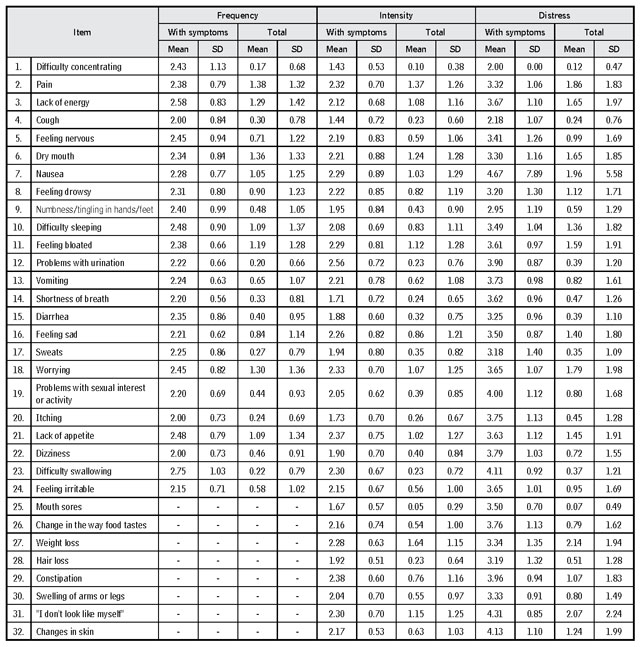
Note: SD stands for standard deviation.
Source: Own elaboration.
Discussion
Cancer patients consistently experience physical and psychological symptoms regarding both illness and treatment. When the symptoms are not identified (especially psychological ones, which will, consequently, not be treated) the illness will deteriorate the quality of life of cancer patients 10.
Studies by other authors corroborate the results obtained herein. Regarding symptom frequency, for example, Tranmer et al. 11 analyzed physical and psychological symptoms in cancer patients, and observed that the three most prevalent psychological symptoms were “concerns” (61 %), “difficulty sleeping” (55 %) and “sadness” (55 %), whereas physical symptoms consisted in “lack of energy” (83 %), “dry mouth” (82 %) and “pain” (78 %). Similarly, Kolankiewicz 12, when assessing the profile of 268 patients undergoing oncologic treatment for the validation of the MD Anderson Symptom Inventory (MDASI), with mean participant age of over 60, described that the frequent symptoms were “fatigue” (63.1 %), “difficulty remembering things” (56.2 %), “dry mouth” (54.9 %) and “concerns” (54.7 %). Thus, even in the case of distinct populations, symptom similarities are observed.
It should be noted that women have a subtler self-perception of health than men, and therefore, present more complaints concerning symptom severity. In this regard, Dun et al. 13 state that women report higher levels of depression and anxiety compared to men, which is corroborated by Miakowski et al. 14, who reported that higher rates of depression in females are due to the fact that women report their anxieties more easily than men. It is important to note that this perception can be divergent according to marital status, since married patients count on greater social support from their families. In fact, Dun et al. 13 consider that social support directly affects patient quality of life.
With regard to topography, liver cancer has been highlighted as the type of cancer whose symptoms are described as being of greater severity. In fact, this is a highly lethal topography. It is mainly related to the high incidence of unresectable metastatic disease in this group, which leads to poor prognoses. In addition, an aggressive management of disease symptoms and treatment-related symptoms is particularly critical in preserving patient functional status and quality of life 14. The main symptoms in this type of cancer, according to that study, are pain, fatigue and weight loss. Regarding colon and rectum cancer, the different forms of therapeutic intervention may lead to a deconstruction of the patient’s self-image, as a result of colostomy, which alters patient quality of life, in addition to the most common symptoms, also observed herein, including fatigue and physical distress 15.
It is important to note that the MSAS is restricted to describing the severity of 32 symptoms. A strong point of this study is the possibility of the analysis of a large scope of symptoms. However, several instruments are currently available for the evaluation of multiple symptoms, but differing in the number of assessed symptoms, level of measurement (ordinal, nominal, continuous, etc.) and the evaluation period to which they refer to (i.e. the last 24 hours, the last week, the last month, etc.). The most frequently applied are the Symptom Distress Scale (SDS), Memorial Symptom Assessment Scale (MSAS), Rotterdam Symptom Checklist (RSC), Edmonton Symptom Assessment (ESAS) and, more recently, the MD Anderson Symptom Inventory (MDASI) 16,17.
In addition, symptoms are usually manifested in combination with each other and should be investigated through multiple symptom assessment tools. Studies demonstrate that combinations or groupings of symptoms are more important than individual symptoms, and that simultaneous symptoms are likely to be multiplicative in nature and have catalytic effect on one another 18. Regarding this proposed analysis, the cluster concept has been proposed as a new direction to better understand the complexity of the multiple symptoms experienced by cancer patients. Symptom clusters are defined as groups of at least two or three simultaneous symptoms related to each other 17,18. In this sense, Boeira et al. 18 carried out a systematized research and pointed out that symptom clusters comprise “neuropsychological” and “gastrointestinal” symptoms. The authors also emphasize that the symptoms have an effect on each other, and, when observed alone, are not specific and sensitive. Thus, the evaluation of these combinations or clusters will present a direct impact on the quality of care provided to cancer patients 19,20.
Therefore, cancer patients are prone to numerous symptoms due to the complexity of the disease and their own way of dealing with changes in their health status. Transformations arising from the disease lead to both psychological and physical symptoms. Therefore, it is extremely important for health professionals to identify these multiple symptoms, from the time of admission to discharge, in order to be able to provide direct care, and for patients who will benefit from the intervention, as symptom summaries allow for this care coverage. In order to do so, clinical protocols should be reviewed, so that this action may be incorporated into patient service routines.
Conclusions
The present study aimed to evaluate the most frequent symptoms presented by patients diagnosed with abdominal cancer by applying the MSAS-BR scale. Symptoms were identified and their relationship with characteristics (such as tumor location, gender, age and marital status) were evaluated. The described symptoms, especially when applying the MSAS subscales, indicate the need for a view that goes beyond physical aspects, and that the psychological and behavioral repercussions that these symptoms generate should be exploited, which may present a significant impact on the quality of life of cancer patients.
It is important to emphasize that cancer patients present symptoms that surpass the physical and material sence: It also affects the emotions of the patient. Such symptoms are multifactorial and can be influenced from diagnosis to treatment. These patients require a holistic view from their health professionals, as several of the symptoms may be related to each other. This indicates the importance of support instruments, so that symptoms may be evaluated in a contextualized manner, allowing health professionals to intervene more effectively and adequately, through a multidisciplinary team.

