











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The operating room (OR) is a complex work structure in the health area and, with the quality and safety of the work processes, it must be continually monitored 1-3. The health sector, notably competitive and dynamic, promoted hospitals to offer higher quality of services through efficient evaluation systems to control, monitor, and improve the efficiency of the service provided by health organizations in the OR 4. The ORs are hospital units with large and costly resources 5,6 that often respond for the financial success of a hospital 6.
The quality of care provided in the OR is, thereby, a high priority for hospitals, especially during an era in which the provision of health care is increasingly challenging 3, which makes it essential to use efficient and accurate measuring systems as a useful tool, and allows managers to control and monitor health services 5. Numerous factors restrict the productivity and efficiency of the OR, including its structure, problems in managing human, financial, and material resources, among others 6.
In a review study of evaluation instruments in the OR, the authors highlight that the instruments are more frequent within the scope of the process, in addition to being essentially associated with the safety and risk culture proposed by the World Health Organization (WHO) 1. The measurement should be multidimensional and involve several components; however, what we frequently observe in health are indicators very focused on financial aspects, that is, on operational results, ignoring other indicators 4. That aspect highlights the need for further development of valid and more comprehensive instruments, integrating the different components of quality evaluation 1, among them, the structure indicators.
The structure deals with the relatively stable and necessary characteristics to provide care and integrates the resources and the organizational structure 7. Proper functioning of the OR also depends on the physical structure, new technologies, adequate materials and equipment, among others 8. While there is little doubt that technological advances have contributed to patient safety, the growing disparity between surgical innovations and the physical environment may contribute to an unacceptable number of adverse events that can be avoided 9.
In a literature review study on the environmental conditions of the OR, the authors, in 182 empirical cases, focus on some aspects related to the structure of the OR, like size, temperature, humidity and air quality, noise, and ergonomic design 10. In addition, another review study seeking to identify instruments to assess the culture of safety in ORs; of the 47 studies included, the authors state that although the culture of patient safety is considered important in healthcare, the number of studies using valid instruments is still quite small 11.
In health services, care is no longer centered on individual professions or specialties and converges on the organization as a whole, in which the principles and strategies of Total Quality Management include the rupture of professional barriers and better management of resources, with nursing playing a predominant role. Everyone should commit to improving the quality of the health services offered to patients and their families, especially in variables that may affect the quality and safety of the care provided.
Thus, the need and relevance of this study is reiterated, inserted in the nursing field, considering, on the one hand, the different roles nurses play in the intraoperative (instrumentalist nurse, circulating nurse, and anesthesia nurse), as well as the decisive role they hold as managers in the ORs.
However, the management systems used by nursing in the OR are highly subjective and do not integrate all the work components associated with the safety and quality of care 12, which justified the need for this research. From this problematic, it is emphasized that, despite the increasing use of health measurement instruments in health, it was not possible to find in the literature adequate instruments to evaluate the structure of the OR. Thus, this study sought to validate a scale designed to evaluate the structure in question (Scale of structure indicators in the OR - SIOR Scale). We believe that the research could become an important contribution to analyze, monitor, and improve the quality of service provided in the OR.
Materials and Method
This was a methodological study comprising the construction and validation of the SIOR Scale, following the steps recommended in the literature 9. In a review of the literature, we verified that emphasis has been placed on the importance of adequate psychometric evaluation of the measuring instruments, especially with regard to the evidence of its validity and reliability 13-17.
The construction of said scale, as well as the items included in it, results from prior studies. Initially, there was a first field study, of qualitative nature, when interviews were conducted with physicians, nurses, service directors, and members of the administration of hospital units to identify what dimensions would be necessary to include to evaluate quality in the OR. To the set of indicators resulting from the analysis of the previous data other indicators were added resulting from a systematic revision on instruments to evaluate quality in the OR 1. To gauge the new proposal of instrument, it was reviewed by a panel of experts through a focal group, from which resulted the 28-item scale within the structure used in the course 2.
The items of the scale are expressed in affirmative phrases, which must be answered through a Likert scale with five response options: “totally disagree”, “partially disagree”, “indifferent”, “partially agree”, and “totally agree”. Thereafter, a pre-test was conducted of the scale with 30 nurses who did not participate in the study. After applying the pre-test, it was possible to make some modifications in certain questions to avoid incongruities in the answers. Thus, the SIOR Scale was made up of 28 items.
The data were collected through a questionnaire with characterization of the participants and through the SIOR Scale. In relation to the sociodemographic characterization, the variables were gender, age, profession, professional category, type of block, years of professional experience, and years working in the OR. The questions in the SIOR Scale encompass variables associated with the facilities, environments, equipment, along with human, financial, and organizational resources. The questionnaire was applied through an electronic form to 1019 professionals working in the OR and who met the following inclusion criterion: Being a nurse or physician with direct action in OR for more than two years in Portugal. Data collection took place from January to May 2018.
Data treatment used the Statistical Package for the Social Sciences (SPSS), version 24. For the psychometric study, recommendations from the literature on the theme were followed 15. Namely, through the Kaiser-Meyer-Olkinque measure to compare simple correlations, and the principal components analysis with orthogonal varimax rotation, the factorial analysis was performed based on the Kaiser rule, excluding factor loads <0.30, in case of existing 13. In addition, a total explained variance greater than 40 was used, as well as the internal consistency evaluation through Cronbach’s alpha.
Regarding ethical considerations, the study was carried out after authorization from an ethics commission (Nº CES246-16) and then forwarded to the other institutions. Respondents were informed of the study and its objectives and of the voluntary nature of their participation, through informed consent. In addition, anonymity and confidentiality were guaranteed in all responses and the research participants’ right to privacy was ensured.
Results
The validation of the SIOR Scale, composed of 28 items, included 1019 professionals working in the OR, namely nurses (73.4 %) and physicians (26.6 %) from 71 Portuguese hospitals. Of these, 69.2 % were females, with a mean age of 43 years (± 9.7) and an average time of professional exercise of 19.5 (± 9.6) years.
Throughout the text, assessments regarding the psychometric characteristics of the scale are presented, especially with regard to their reliability and validity.
Table 1 presents data regarding the characterization of the minimum (Min), maximum (Max), median (Med), Mode and variation coefficient (Var Coeff). The categories of the Likert scale were designated by the respective orders, where it is observed that the participants’ answers cover the whole range of the scale, that is, from 1 to 5.
Psychometric characteristics of the SIOR Scale
After the individual study of the evaluation items of the SIOR Scale referring to the OR structure, we proceeded to an analysis of the conceptual structure of this scale through an exploratory analysis factor, keeping in mind the identification of the underlying factors of said assessment. Such factors allowed understanding the motivations behind the pattern found in the responses, as well as measuring the validity of said instrument for the objective sought.
At first, correlations were noted between the degrees of agreement of the various items, as well as the existence of many moderate correlations and a considerable number of high correlations. In addition, the inter-item medium correlation is 0.267, which is due to the existence of low correlations between some items (usual situation in any questionnaire, given that this value is acceptable). In turn, the corrected item-total correlations are all moderate or somewhat elevated, with the sole exception of item 19. Thereafter, we proceeded to calculate the adequacy measure of the Kaiser-Meyer Olkin sampling, presented in Table 2 for each item and for the whole scale (global value). Obtaining a value of 0.9 in the Kaiser-Meyer Olkin coefficient allowed gauging the adequacy of the analysis factor. The data revealed that the factorability of the correlation matrix is appropriate to perform a factor analysis from them.
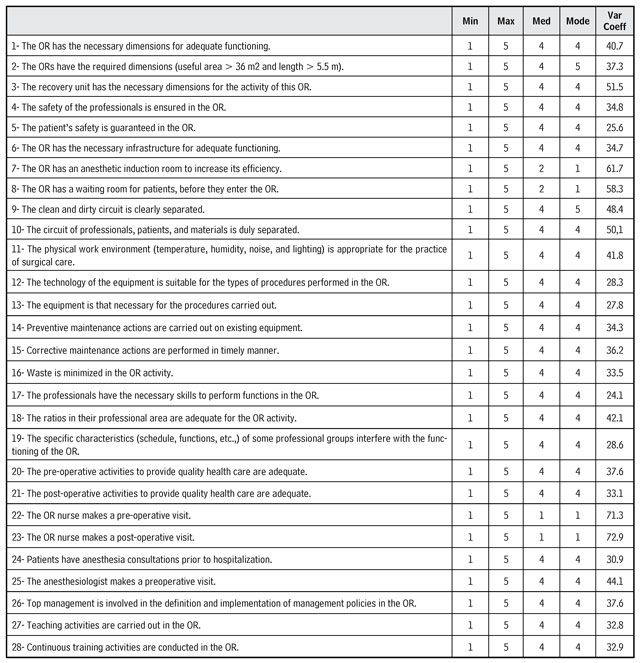
Table 2 Structure dimension subscale ― Adequacy measurement of the KMO sampling
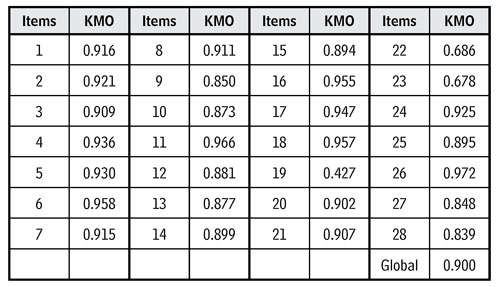
Source: Own elaboration.
The factor analysis was performed with extraction of factors through the principal components method, in which a solution was obtained of seven factors that included the 28 items of the scale and explained 62.1 % of the total variance. The results of the factor analysis forced to seven factors followed by varimax rotation and Kaiser Normalization are presented in the following table 3, with reference to communalities. That is, the percentage of variance of each item was explained together with the seven factors extracted. In the factor analysis, no item was excluded and all presented a correlation value ≥ 0.4.
With regard to the factorial structure obtained, it should be highlighted that factor 1 explained 31.30 % of the variance and is composed of five items, namely, 11, 12, 13, 14, and 15. Once the items are associated with the presence of equipment, technology, maintenance, and environmental characteristics, principally temperature, humidity, among others, the designation of “Environment and equipment” was attributed.
Factor 2 explained 8.16 % of the variance and it includes items 5, 16, 17, 18, 20, 21, and 26; because these items relate to human, organizational, and financial resources to provide quality care, as well as variables associated to safety, the factor was designated “Resources for quality and safety”.
Factor 3 already explained 6.33 % of the variance and saturate items 7, 8, 9, and 10. The items are related to the circuits inside the OR referring to the patient, professionals and clean and dirty circuits, which is why the factor was called “Circuits in the operating room”.
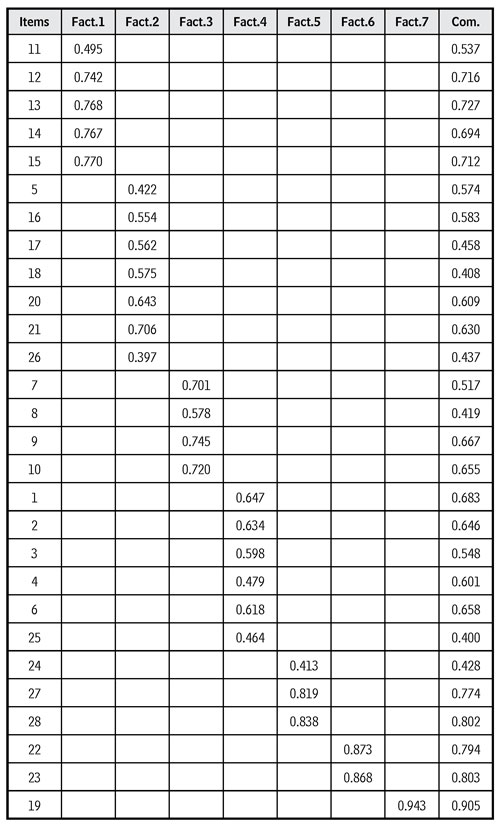
Factor 4, in turn, was composed of six items (1, 2, 3, 4, 6, and 25) and explained 4.58 % of the variance. The items relate to variables associated with the dimensions of the different OR structures and the necessary conditions for its functioning. Thus, we attribute to this factor the designation of “Facilities and operating requirements”.
With regards to factor 5, it explained 4.43 % of the variance and is composed of items 24, 27, and 28. The items relate to issues associated with education and training and to the set of activities aimed at promoting quality and way of performing in the practice. The factor was titled “Training and praxis in the operating room”.
With relation to factor 6, it was composed by items 22 and 23 and explained 3.69 % of the variance because it is associated with pre-and postoperative nursing visits. It was designated as “Continuity in nursing care”.
Lastly, factor 7 is composed of only one item (19) and explained 3.58 % of the variance. The item was not associated to any other, that is, it was isolated in a factor, meaning that the response pattern is different from all the other items. In fact, this item focuses on a very particular and diverse aspect of all the others, given that it refers to the specific characteristics of the professional groups, especially schedules, functions, etc., and how these interfere in the OR functioning. The factor was designated as “Specificities of professional groups”.
Although factor 7 only has one item, it was maintained by the relevance of its evaluation, highlighted by the review on the theme (1) and by the group of experts (2), especially regarding, for example, the schedule gap of the different professionals who integrate the surgical team.
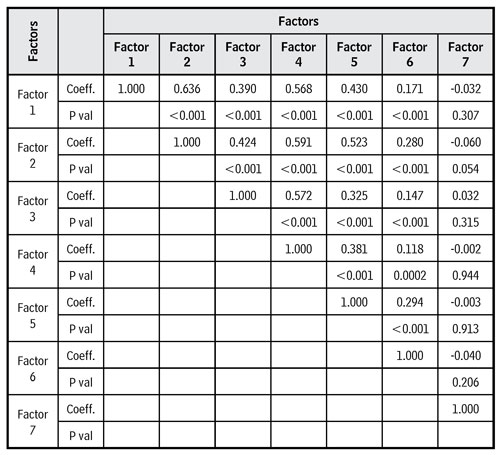
Spearman’s matrix of correlations between the factors is found in Table 4. The factor “Environment and equipment” (factor 1) had significant correlations with all the others, except with the “Specificities of professional groups” (factor 7). These correlations are all positive, although moderate with factors 2 to 5 and weak with factor 6.
The factor “Resources for quality and safety” (factor 2) had relevant correlations with the following factors, except with the “Specificities of professional groups” (factor 7). The correlations were also all positive, likewise moderate with factors 3 to 5 and weak with factor 6.
The factor “Circuits in the operating room” (factor 3) had significant correlations with the following factors, except with the “Specificities of professional groups” (factor 7). The correlations were all positive, although moderate with factors 4 and 5 and weak with factor 6.
The factor “Facilities and operating requirements” (factor 4) presented significant correlations with the following, except with the “Specificities of professional groups” (factor 7). The correlations were both positive, but moderate with factor 5 and weak with factor 6.
The factor “Training and praxis in the operating room” (factor 5) had significant, positive and weak correlation with factor 6 and a non-significant correlation with factor 7.
Already the factor “Continuity in nursing care” (factor 6) presented a non-significant correlation with the factor “Specificities of professional groups” (factor 7). It should be noted, therefore, that this last factor was not correlated with any of the others, being the only one in this situation.
In fact, the factorial weight of the item in factor 7 is very high (0.913), as well as the respective communality (0.905), which leads to admitting the utility of keeping this item in the scale, that is, the relevance of its validity. It was concluded, in fact, that it is a different aspect from all the others contemplated in the instrument, but it remains important, that is, it was considered that it is relevant to evaluate the functioning of the OR in the part given by this item and, therefore, opting to consider it valid and to keep it in the instrument.
For the quality evaluation of the factorial model obtained, it was possible to observe the matrix of the residuals, that is, the matrix of the differences between the existing correlations between the items and those estimated by the factorial model with the seven factors retained. Herein, 113 residuals were identified (that is 2 %) with an absolute value > 0.05, which indicates a good quality of fit, that is, when the waste percentage is < 50 %. In addition, the quality index of fit or Goodness of Fit Index (GFI) was 0.839, indicating good quality. In turn, the Root Mean Square Residual (RMSR) was 0.05, which also means that the fit has a good quality. In synthesis, the coefficients show overall that the fit has good quality.
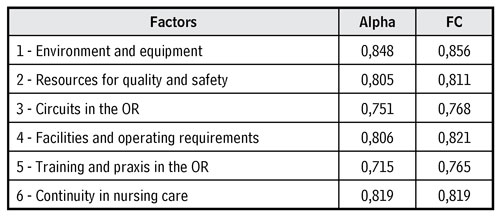
Finally, the reliability and the validity of the scale were evaluated. The values of Cronbach’s alpha coefficient and of reliability are found in Table 5. The last factor was not included because it had only one item and it was not possible to calculate. The alpha value for the whole scale was 0.907, which is very high and shows a very strong internal consistency. Referring to the composite reliability of all the factors, these showed high reliability.
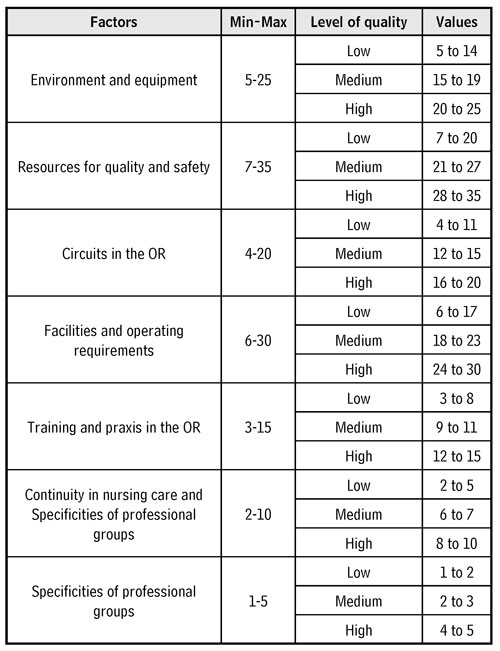
For their future application and according to the dimensions obtained to be applied as evaluation instrument of the structure in the OR, standardization criteria are proposed of the scale presented in Table 6.
Discussion
This study sought to validate a scale to evaluate the structure in the OR (SIOR Scale). Measurement in health is essential in scientific research and in clinical practice. Through the application of scales in health, decisions can be made, which is why the instruments must be reliable and valid. On the contrary, serious risk exists of obtaining inaccurate or biased results that may lead to erroneous conclusions 13. The SIOR Scale presents good validity and reliability indicators. It was possible to observe that the data obtained were subject to factor analysis. The KMO value obtained was 0.900 and permitted stating that the correlation matrix factor is good 14.
The factor analysis, with extraction of factors using the principal components method, by means of the Kaiser rule, permitted explaining 62.1 % of the total variance. Said analysis involved an acceptable number of factors and was considered the best solution in terms of interpretation and meaning of the dimensions. All the items collected, in the different factors, weights above or equal to 0.4. According to the authors, the parameters of the coefficient of reliability vary, but, in general, values below 0.40 are considered low reliability; between 0.40 and 0.69, moderate reliability; and above 0.70, high reliability 15. In the instrument presented, the majority of the items revealed high reliability. The correlational analysis among the items of the scale and the global scale also supports the suitability of the instrument.
The internal consistency of the scale established by Cronbach’s alpha showed adequate reliability indices for its global version (0.9) and for each of its factors, in which none of the results was below 0.7. Most researchers evaluate internal consistency through Cronbach’s alpha coefficient 16, but there is no consensus as to which Cronbach’s alpha coefficient values are ideal, but, in general, it is recommended to adopt coefficients > 0.70 13,14,16.
From the exploratory factor analysis with varimax rotation, the 28 items were grouped into seven dimensions, namely: “Environment and equipment”, “Resources for quality and safety”, “Circuits in the operating room”, “Facilities and operating requirements”, “Training and praxis in the operating room”, “Continuity in nursing care”, and “Specificities of professional groups”.
Referring to questions of “Environment and equipment”, the hospitals face increasing pressure to meet the demands, often contradictory, of providing a safe environment and, at the same time, control operational costs. Data based on scientific evidence is necessary to provide adequate information to manage the OR facilities and respond to said demands. Given this framework, the use of measurable environmental quality indicators can contribute to optimizing the cost and quality of an OR 18. Furthermore, the OR equipment plays a crucial role in caring for patients in a health environment. With the development of innovative and advanced equipment, surgeons are able to perform surgeries efficiently as it becomes easier to manage increasingly complex procedures; however, they represent high costs for the hospitals 19.
The factor “Resources for quality and safety” incorporated items referring to human, financial, and organizational resources promotors of a culture of safety in the OR. The safety issues associated with the checklist concept have been widely disseminated by the WHO as central guideline for care practice in the OR 1.
The factor “Facilities and operating requirements” evidenced some architectural aspects of these units. According to the authors, many ORs were built more than 30 years ago, and a common solution has been to increase the size of the surgical center to try to accommodate more equipment and larger teams. Nevertheless, most are inadequately designed to handle equipment, processes, technology, and people that a well-functioning contemporary OR needs 10. The ideal project of an OR must incorporate the best practices to reduce environmental contamination, but should also consider the optimal placement of equipment and recognize that circuits are critical to patient safety. The regulation of clean and dirty circuits is important to reduce the risk of infection 20. This aspect is visible in factor 3 referring to the “Clean and dirty circuit” in the operating room.
In addition, advances in surgery support the need for a greater focus on training and the surgical practice, by means of simulators and serious games in the training programs of the most diverse levels 21 and replicate them so there is better “Training and praxis in the operating room”, visible in factor 5.
Factor 6, titled “Continuity in nursing care”, reinforces the importance of the pre- and post-operative visits made by the OR nurse. In a study on the pre-operative visit made by nurses, the authors emphasize that preoperative teaching increases self-care skills, of patient compliance, and helps to reduce anxiety. The pre-operative visit made by the nurses also contributed to establishing a relationship based on trust between the staff and the patient, in addition to providing them with diverse information 22.
Related to the high costs of the ORs, in addition to the aforementioned materials, are the personnel costs (surgeons, anesthetists, nurses). Management of resources requires adequate coordination and permits better planning and efficiency of the ORs; however, synchronizing all these resources is no easy task 23, an aspect visible in the factor referring to the “Specificities of professional groups”.
The validated scale contemplates the essential indicators and dimensions to guarantee adequate evaluation of the OR structure. As a limitation of this instrument, it was considered that it was restricted to questions of structure, other instruments related to the process and the result are being developed and validated to ensure evaluation and monitoring of quality in the OR as a whole.
Conclusion
This study permitted evidencing the quality of the SIOR Scale, through evidences of how the measurement properties were evaluated to justify the selection of this instrument to measure the OR structure. The psychometric study of the Scale, composed by 28 items, permitted stating that it is a reliable and valid instrument. The factor analysis also permitted identifying seven dimensions, namely “Environment and equipment”, “Resources for quality and safety”, “Circuits in the operating room”, “Facilities and operating requirements”, “Training and praxis in the operating room”, “Continuity in nursing care”, and “Specificities of professional groups”. Said factors prove to be important aspects for a correct assessment of the ORs structure and integrate the amplitude of their indicators.
The measuring instruments play an important role in research, in the clinical practice, and in health evaluation. The definition of valuable, reliable, and useful quality indicators for applicability in the OR is a first step in the improvement process, but it is necessary to consider how these metrics can be used and how changes can be implemented. The items integrated in the scale permitted nurses to measure, evaluate, and monitor the structures of the OR and potentiate corrective measures to guarantee the quality and safety of care.

