











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Customer satisfaction with nursing care is a cross-sectional theme in all care contexts. Its definition is not unanimous in the literature because it is a multidimensional concept and difficult to operationalize 1. However, the influence of nurses’ professional experience on patient satisfaction is consensual, indicated as the factor that most influences satisfaction as a whole. 2.
In Nursing, the patient satisfaction assessment precedes its definition. The first instrument to measure satisfaction was developed in 1957, when nursing care was assessed by total nursing care hours and available care hours 3. Later, in 1975, an instrument emerged to measure satisfaction, which included the dimensions: professional technical behavior, intra- and inter-personal expressions, and trust and educational relationships 4. This instrument highlighted the association between expectations and satisfaction, defining patient satisfaction as the degree of congruence between their expectations about the ideal care and the care actually received. During the 1980s studies increased on the quality of care and which included satisfaction as a quality indicator. However, research has proliferated exponentially in the last decade, attributed to the active role of patients in health care 1. Currently, care satisfaction is frequently assessed in different contexts, generally considering this concept as the patient’s opinion about the nursing care received 5. It is an indicator of the quality of care provided, and it is more common in its evaluation to use questionnaires to measure client satisfaction within the hospitalization context 6.
Regarding child hospitalization, traditionally, adults, professionals and caregivers are used to assess satisfaction, and the opinion of the child has been poorly studied 7-13. Nevertheless, the need to involve children in decisions affecting them 14-16 and to consider their opinion is generally accepted. Efforts have increased in the search for ways to listen to children and integrate their perspectives 17. These are the result of the growing recognition of children’s rights, particularly in the international context and in the hospital environment 12. In addition, children have been excluded from participating in scientific research due to ethical/legal reasons and the need to protect them 18.
Within the hospital context, children are at risk of seeing their rights neglected or undervalued due to the perception that they are immature and/or unable to express their opinion 19. Thus, this article is based on the belief that children, like adults, have particular perspectives, skills, along with the right to be heard and to speak for themselves provided appropriate methodologies are used 20. The main theme is satisfaction with the quality of nursing care during hospitalization.
Development of measurement instruments constructed and validated specifically for the pediatric population permit more realistic knowledge of their opinion. It has been verified that few valid instruments exist that consider children as users of health services 7. Moreover, it is particularly important to measure satisfaction in the most vulnerable groups, such as children 21, given that they are the most dependent on nursing care.
The literature review permitted identifying the instrument Children Care Quality at Hospital (CCQH) applied specifically on school-age children 22-23. This instrument enables gathering basic information about children’s satisfaction with their nursing care experience and helps to identify key areas to improve care quality when care does not meet their expectations. In this sense, its application to other cultural contexts is justified by the potential to gain knowledge on the child’s view of nursing care, which contributes to improving the quality in practice with a genuinely child-centered approach.
The CCQH was developed in Finland to measure the quality of nursing care from the child’s perspective. It is based on children’s expectations and definitions regarding the quality of pediatric nursing care 24-25, on quality indicators of previous studies, and partly on the definition of nursing care quality by adult patients 26. The instrument was developed in three phases: in phase I, a first version was built based on the literature review submitted to expert panel; in phase II, the instrument was applied to a sample of 41 children and rated by 19 nurses; thereafter, it was reformulated and again applied to a sample of 16 children; phase III measured the instrument’s psychometric characteristics, namely construct validity through the principal components method and internal consistency by calculating Cronbach’s alpha: nurses’ characteristics (0.557), nurses’ activities (0.809), and nursing environment (0.761) 22.
In its final version, the CCQH is comprised of 49 items divided into three categories: nurses’ characteristics, nurses’ activities e nursing environment, categorized according to a Likert scale from 1 to 3, in 30 items, using words and faces (1 = never =  ; 2 = sometimes =
; 2 = sometimes =  ; 3 = always = ☺), and from 1 to 4 in the remaining 19 items, with the agreement scale and using teddy bear images. Higher scores indicate greater satisfaction.
; 3 = always = ☺), and from 1 to 4 in the remaining 19 items, with the agreement scale and using teddy bear images. Higher scores indicate greater satisfaction.
Given the relevance and timeliness of the theme, we consider it appropriate to adapt the instrument into Portuguese so that it can be used within the context of child hospitalization. Thus, the objective of this study was to structurally adapt and validate the CCQH questionnaire for this language.
Methodology
This is a methodological study that included translation, cross-cultural adaptation, and obtaining initial psychometric properties of an instrument that allows measuring the satisfaction of school-age children (7-11 years of age) with nursing care within the hospitalization context. This study is part of a PhD thesis in Nursing, underway at the Institute of Health Sciences at Universidade Católica Portuguesa in Portugal.
After the formal authorization by the original author of the CCQH, the first phase comprised the transcultural adaptation of the instrument for Portuguese from Portugal, according to internationally established procedures, into five stages: initial translation by two translators, synthesis of both translations, back-translation, expert panel, and pretest application 27, as verified in Figure 1. A second phase evaluated the instrument’s psychometric properties with the application of the questionnaire in Portuguese to a sample of 252 children between 7 and 11 years of age.
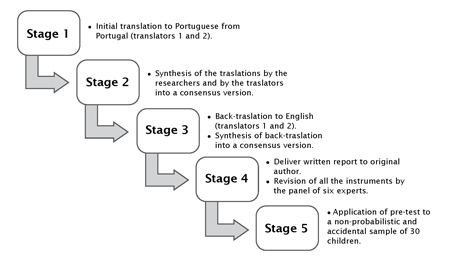
Source: own elaboration.
Figure 1 Flowchart of the procedure of cultural adaptation of the CCQH instrument.
The first phase sought to guarantee the linguistic and conceptual equivalence to ensure the content validity of the instrument’s Portuguese version, whereby following the methodological procedures of translation, adaptation, and cultural validation. The translation process aimed at producing a document from the original language (English) to the intended language (Portuguese) 28. The instrument was translated by two individuals, both fluent in the English language: a translator in the area of Nursing and a translator without knowledge in the area, as recommended 27. The translations were synthesized into a single document by the researchers and by the translators, subsequently producing a consensus version. The next step was the back-translation stage, which was carried out by two individuals, both with native English and without scientific training in health. These versions were again synthesized by translators and researchers into a single consensus document.
This was followed by the adaptation phase of the instrument under analysis, defined as a process of considering the differences between the two cultures to ensure equivalence of meaning 28. The document was sent to the original author of the CCQH instrument, as well as the detailed report of the results associated with the phases mentioned.
In the third phase a panel of experts was created 27 for effects of cultural validation. The panel was made up of two professors from the scientific area of Nursing experienced in the use of the method of transcultural adaptation; two nurses specialized in infant and pediatric health, a Portuguese professor, and a translator. This stage sought to ensure that the instrument had the same properties as the original instrument so it could be applied in the same manner 28. The content validity index that measures agreement among evaluators was calculated, considering the value above 0.9 as reference 6. Among the 49 items that make up this instrument, it was verified that only two items (“my intimacy is protected” and “there is privacy”) were not concordant among all the experts. A content validity index of 0.96 was found. After the revision and verification of the linguistic issues by a Portuguese teacher, the pre-test version was constituted, submitted to a non-probabilistic and accidental sample 6, constituted by 30 children hospitalized in a hospital pediatric service, maintaining the same application criteria listed in the original version: children from the age group from 7 to 11 years, with at least 24 hours of hospitalization, who could speak and write in Portuguese and who had the capacity to respond to the items of the instrument (alone or with help). The following were established as exclusion criteria: children with psychiatric or neurologic pathology, with delayed development, and children in outpatient regime.
To apply methodological procedures of instrument validation, the sample size must be defined a priori and must vary between 2 and 20 valid responses per variable 29. In this case, the instrument has 49 items and five answers were defined for each variable, with a sample > 245. Thus, after the pretest, the instrument was applied between January 2015 and December 2016, for an average period of three months by each institution. This period was selected because it was considered adequate to obtain the desired number of children. The population comprised hospitalized children, with selection of a sample of 252 children, which maintains the same inclusion and exclusion criteria. The instruments were applied directly by the principal researcher, agreeing on how to access the sample and apply the instruments with the nursing manager in each service.
The Statistical Package for Social Sciences, version 24, was used for the statistical analysis. To assess the CCQH construct validity, the principal component analysis method was used; applying the Kaiser method and the Kaiser-Meyer-Olkin test (KMO > 0.6) along with Bartlett’s sphericity test (BET < 0.05). The latter to ensure the suitability of the factorial model to the correlation matrix to perform factor analysis (calculation of the degree of homogeneity or similarity of the various items or questions of the instrument). Verification was made that the number of items of the original instrument remained.
To assess the internal consistency, the calculation of the Cronbach’s alpha coefficient was used. Knowing that the alpha coefficient value could vary from 0 to 1 and that an adequate internal consistency appears with values > 0.70, which indicates that the questions are similar or homogeneous without being redundant 6,30. It is one of the most commonly used measures and is defined as the correlation expected between the instrument used and other instruments in the same universe and the number of items measuring the same characteristic 6.
This study was registered with the National Data Protection Commission (Registry 1.644/2015) and approved by the ethics committees of the hospitals involved.
In the application of the instrument, verbal and written consent was requested from both parents and children. Anonymity and confidentiality of responses were ensured, and the Informed Consent Form was provided. Using simple language, the study was explained to the children, so that they could make a reasoned decision about their participation 15,18. The objective was presented, as well as what was requested of them and the expected completion time. It was also assured to all children that not participating would not have any consequences or risks, emphasizing, as benefits, the importance of participating and expressing their opinion. There were no situations of refusal to participate either by parents or children.
Results
The first phase applied 30 questionnaires, and the children, generally, stated having understood the instrument and the questions. One 8-year-old child reported not understanding the words “programmed” and “honesty”, and two 7-year-old children reported not understanding the word “intimacy”. The definition of the terms was used as a clarification strategy. The words were explained by the researcher with simpler terminology. Given that the number of children (n = 3) Who reported difficulties was lower than 15 % of the total of children surveyed, it was decided to keep the instrument 31 after the pre-test.
The 252 children participating in the study had a mean age of 8.9 years (SD = 1.4), and were mostly of male gender (52.8 %). Regarding the motive for the hospitalization, most of the children referred to sudden illness as reason for their hospitalization (n = 247), 17.4 %, because they got hurt (n = 44), and 66.8 %, because they got very sick (n = 165). With reference to the duration of the hospitalization (n = 252), verifying Median = 3 and IQR = 3.
The instrument is composed by three domains: “Nurses’ characteristics”, “Nurses’ activities” and “Nursing environment”. Regarding the domain “Nurses’ characteristics”, exploratory factor analysis was conducted, using the principal component analysis method; applying the Kaiser method, having identified a factorial structure with a domain (eigenvalues ≥ 1 and saturation of the item in the factor ≥ 0.35) (Table 1).
Table 1 Factor analysis of the domain “Nurses’ characteristics”
| N.º of the item | Item abbreviated | Saturation value of the item in the factor of the domain “Nurses’ characteristics” |
|---|---|---|
| 2 | “pleasant” | 0.80 |
| 5 | “honest” | 0.75 |
| 1 | “kind” | 0.72 |
| 2 | “competent” | 0.67 |
| 4 | “fun” | 0.61 |
| Eigenvalue Explained variance | 2.57 51.29 % |
Source: own elaboration.
Through analysis we confirm the one-dimensional existence, whose explained variance total is of 51.29 %; in the application of the KMO test, a value of 0.79 was obtained, within an appropriate variance interval 32. In turn, the saturation of the item in the factor varies between a maximum of 0.80 in the statement “my nurses are pleasant” and a minimum of 0.61 in the statement “my nurses are fun”. We verified that the Cronbach’s alpha coefficient has a value of 0.75, which allows considering that it presents internal consistency 33.
The domain “Nurses’ activities” is constituted by three subscales: “Caring, entertainment, and support”, “Physical care and treatment”, and “Education”.
An exploratory factor analysis was performed of the subscale “Caring, entertainment, and support”, considering 238 participants with valid responses. As can be verified in Table 2, we confirm the one-dimensional existence, whose explained variance total is of 31.09 %.
Table 2 Factor analysis of the domain “Nurses’ activity”, subscale “Caring, entertainment, and support”
| N.º of the item | Item abbreviated | Saturation value of the item in the factor in the subscale “Caring, entertainment, and support” |
|---|---|---|
| 5 | “my opinions are considered” | 0.67 |
| 7 | “I am given comfort” | 0.62 |
| 4 | “I am listened to” | 0.60 |
| 10 | “they take care of me like my parents” | 0.60 |
| 2 | “they talk about interesting things” | 0.59 |
| 6 | “I am encouraged” | 0.58 |
| 8 | “I am informed about what I could do at the hospital” | 0.54 |
| 9 | “they encourage me to participate in the care” | 0.53 |
| 3 | “my intimacy is protected” | 0.46 |
| 1 | “they play with me” | 0.50 |
| 11 | “they pay attention to my favorite food” | 0.39 |
| Eigenvalue Explained variance | 3.42 31.09 % |
Source: own elaboration.
From the application of the KMO test to determine the adequacy of the sample and the possibility of performing the factor analysis, a value of 0.72 was obtained, within an appropriate variance interval 32. The saturation of the item in the factor varies between a maximum of 0.67 in the statement “my opinions are considered” and a minimum of 0.39 in the statement “they pay attention to my favorite food”. The value of the Cronbach’s alpha coefficient is of 0.76, which is why it may be considered that the subscale under study has internal consistency 33.
The following subscale, “Physical care and treatment”, was also subject to exploratory factor analysis and, as verified in Table 3, we confirm the one-dimensional existence, whose explained variance total is of 49.64 %.
Table 3 Factor analysis of the domain “Nurses’ activity”, subscale “Physical care and treatment”
| N.º of the item | Item abbreviated | Saturation value of the item in the factor in the subscale “Physical care and treatment” |
|---|---|---|
| 2 | “help me to eat” | 0.82 |
| 3 | “help me to take a shower” | 0.78 |
| 4 | “help me to GO to the bathroom” | 0.76 |
| 1 | “relieve the pain” | 0.34 |
| Eigenvalue Explained variance | 1.99 49.64 % |
Source: own elaboration.
For this subscale, the value of applying the KMO test is 0.61, within an adequate variance interval 32. In turn, saturation of the item in the factor varies between a maximum of 0.82 in the statement “help me to eat” and a minimum of 0.34 in the statement “relieve my pain”. This value is marginal to the lower limit; however, this is a relevant item in the child-nurse relationship, which is why it is accepted in the analysis. Regarding the internal consistency, Cronbach’s alpha coefficient is 0.66. It is a marginal value, hence, according to the criteria 33, it may be considered that the subscale has an acceptable internal consistency.
The third subscale of this domain is “Education” and, through the exploratory factor analysis, using the principal component analysis method, we confirmed its one-dimensionality whose explained variance total is 37.82 % (Table 4).
Table 4 Factor analysis of the domain “Nurses’ activity”, subscale “Education”
| N.º of the item | Item abbreviated | Saturation value of the item in the factor in the subscale “Education” |
|---|---|---|
| 10 | “when can I go back to my games” | 0.69 |
| 8 | “the care to have at home” | 0.68 |
| 9 | “when can I GO back to school” | 0.65 |
| 6 | “how to move around the hospital” | 0.65 |
| 2 | “my treatment” | 0.65 |
| 7 | “the duration of my hospitalization” | 0.61 |
| 5 | “what can I eat and drink” | 0.60 |
| 1 | “the reason for my hospitalization” | 0.59 |
| 3 | “my medication” | 0.50 |
| 4 | “my procedures (how to draw blood or get an X-ray)” | 0.48 |
| Eigenvalue Explained variance | 3.78 37.82 % |
Source: own elaboration.
Application of the KMO test revealed a value of 0.72, within an adequate variance interval 32. Saturation of the item in the factor varies between a maximum of 0.69 in the statement “when can I go back to my games” and a minimum of 0.48 in the statement “my procedures (how to draw blood or get an X-ray)”. The Cronbach’s alpha coefficient value is 0.82, which permits considering that the subscale has good internal consistency 33.
Concerning the third and final domain of the questionnaire, “Nursing environment”, the exploratory factor analysis revealed a factor structure with three factors: “Social environment”, “Physical environment”, and “Emotional environment” (Table 5).
Table 5 Factor analysis of the domain “Nursing environment”
| N.º of the item | Item abbreviated | Factor 1 Social environment | Factor 2 Physical environment | Factor 3 Emotional environment |
| 9 | “there is privacy” | 0.72 | ||
| 10 | “my parents accompany me” | 0.65 | 0.13 | |
| 11 | “my relatives can visit me” | 0.61 | 0.14 | |
| 7 | “my stay has been pleasant and comfortable” | 0.60 | 0.30 | |
| 8 | “it’s easy to find places like the bathroom” | 0.51 | 0.15 | |
| 13 | “the nurses keep me company” | 0.39 | 0.359 | |
| 12 | “my friends can visit me” | 0.30 | 0.14 | |
| 3 | “there are enough videos and games” | 0.13 | 0.76 | 0.23 |
| 4 | “there is enough manual work” | 0.36 | 0.69 | |
| 2 | “there are enough books and magazines” | 0.53 | 0.62 | |
| 5 | “there are enough toys” | 0.58 | ||
| 14 | “other children hospitalized keep me company” | 0.39 | 0.51 | 0.11 |
| 6 | “there are appropriate place for being with my family” | 0.48 | ||
| 1 | “time goes by fast” | 0.34 | ||
| 18 | “I’m afraid of doctors” | 0.80 | ||
| 19 | “I’m afraid of pain” | -0.14 | 0.12 | 0.76 |
| 15 | “I’m afraid of being alone” | 0.26 | 0.65 | |
| 17 | “I’m afraid of nurses” | 0.42 | -0.36 | 0.57 |
| 16 | “I’m afraid of the injections” | 0.42 | -0.37 | 0.50 |
| Eigenvalue Explained variance | 3.19 16.80 % | 3.03 15.93 % | 2.34 12.31 % |
Source: own elaboration.
Through the factor analysis, we confirmed the multidimensional existence, with three factors, whose explained variance total is of 45.05 %. Application of the KMO test yielded a value of 0.71 and it is within an appropriate variance range. 32. With respect to the internal consistency, the study resorted again to the calculation of Cronbach’s alpha coefficient, obtaining values between 0.77 and 0.68 (marginal value that can be considered valid), which permits confirming the internal consistency 33, as noted in Table 6.
Discussion
Development of the CCQH in its original version took place in three phases and was an instrument of interest for use with hospitalized children 22. This study sought to translate and adapt the CCQH instrument for Portuguese from Portugal, as a tool to measure satisfaction with the quality of nursing care provided within a hospitalization context in school-age children (7-11 years of age), from their own perspectives.
In the initial process, the equivalence of meaning was obtained by following the methodological process and validating the course with the author of the original instrument. Given the specificity of some terms and their cultural and linguistic significance, the use of the initial translation procedure, synthesis of the two translations, back-translation, expert panel, and pre-test application were central to ensuring the CCQH equivalence.
It should be noted that the process of translating and adapting research instruments requires less time and costs than the creation of research instruments. In addition, it permits the comparison of results among the population, which translates into fundamental scientific progress to develop knowledge 27.
The adaptation of the instrument for Portuguese from Portugal maintained the 49 items that comprise the original instrument. This number of items can be considered too long for some children 22; however, in this sample, none of the children reported this aspect. In the adaptation process, the original instrument designations were maintained and, in general, there was an increase in the internal consistency values in all CCQH domains and subscales. In the first domain, “Nurses’ characteristics”, there was an increase in the Cronbach’s alpha value (0.75) in relation with the original instrument (0.56) 22, which demonstrates that the items measure the attribute. The literature identifies that the personal characteristics of the nurses are recognized by the school-age children 34. They value knowing nurses as people 19, being an aspect identified as the best experience during hospitalization 7, but also as expectation of care. The characteristics that integrate the instrument, kind 19, competent 23, pleasant 16, fun, and honest 15,24 are identified in research on this theme.
In relation to the second domain, “Nurses’ activities”, in the original instrument, the author considered five subscales: “Entertainment”, “Caring and communication”, “Initiative support”, “Education”, “Physical care and treatment”. The translated version identified three subscales in this domain: “Caring, entertainment, and support”, which includes all the items of the subscales “Entertainment”, “Caring and communication”, and “Initiative support”, as well as the item “pay attention to my favorite food”, framed in the subscale “physical care and treatment” in the original instrument. The second subscale includes all the items of the subscale in the original instrument, “Physical care and treatment”, except for the item already indicated. In turn, the third subscale identified (“Education”) in this domain coincides with that in the original instrument and includes all subscale items.
The domain “Nurses’ activities” is reported in the literature as relevant and important for children 16-17; however, it is a broad category that can encompass several items. It includes aspects related to the development of activities by nursing professionals during the clinical practice. We emphasize that the aspects that constitute this category are interrelated. For example, children are expected to provide information prior to the procedures in a respectful environment while providing distraction 19, which fits in the subscale “Caring, entertainment, and support” that integrates the translated CCQH version. The differences found are probably related with this aspect, but also with cultural issues that source of satisfaction/dissatisfaction in Portuguese children.
Among the most valued aspects in this domain, we find the supply of information and entertainment 7,17. Children Express satisfaction when they are provided information about the care in a way they can understand 35 and which allows them to be active in the care process. When they are not explained the care, for example, regarding the moment of performing the procedures 18, they express their dissatisfaction. They also expect nurses to conduct entertainment activities that help them to have a more positive view of the procedures 36 and to pass time 11.
Regarding the third domain, “Nursing environment”, the original author considered three subscales: “Physical environment”, “Social environment”, and “Emotional environment”. The version of the instrument in Portuguese from Portugal also identified three subscales, with variation in the items. Thus, the first subscale, “Physical environment” (factor 1), verified that the items overlap with those from the original subscale, except for the items “my stay has been comfortable and pleasant” and “it is easy to find places, like the bathroom and the playroom”, which passed to the second subscale (“Social environment” - factor 2); and the item “other children hospitalized keep me company” passed from the subscale “Social environment” to this subscale. In relation to the second subscale, the items also overlap, except for the item already mentioned. Lastly, in the subscale “Emotional environment” (factor 3), the items overlap integrally. The environment during the child hospitalization is also reported in the literature as source of satisfaction/dissatisfaction among children (23, 36-38). These highlight physical aspects, like care-related equipment (such as infusion pumps) as unknown and threatening 39. Also identified are the social environment, related to the interaction with professionals and other hospitalized children and the emotional environment. This refers to the feeling of well-being that allows them to live the hospitalization experience in a more enjoyable manner. It permits the child to be more autonomous and participative in the care 40 and, consequently, it generates satisfaction.
The results found reveal the possibility of the CCQH being used to assess the satisfaction of hospitalized children with the quality of nursing care. The statistical tests conducted to validate the construct of the domains of quality of care of children hospitalized, through three domains, show logical relations and the contribution of the 49 items for the instrument as a whole.
Conclusion
The CCQH instrument permits contributing new knowledge, inasmuch as it provides the unique perspective of school-age children on their hospitalization experience. It permits identifying key aspects, valued by children, which can be worked by nurses to make nursing care more adapted and satisfactory to children.
The CCQH questionnaire was adapted and validated for Portuguese to study its domains. The final version of the instrument consisted of 49 items distributed across three domains: nurses’ characteristics, nurses’ activities and nursing environment.
The analysis performed demonstrated empirical evidence of the CCQH questionnaire in Portuguese. The adaptation and validation process, according to international guidelines, as well as the analysis of the psychometric properties of construct validity and internal consistency, allow concluding that this is a reliable and valid instrument to assess satisfaction with the quality of nursing care from the perspective of hospitalized children.
The CCQH version adapted for Portuguese from Portugal is an instrument that can be used by nurses, within the hospital context, to measure children’s satisfaction with the quality of nursing care, which contributes to improved care.

