











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Diabetes mellitus (DM) is a significant public health issue and a socioeconomic burden in Indonesia. In 2019, approximately 463 million adults around the world had diabetes; it is estimated to increase to 700 million by 2045 1. About 79 % of adults with diabetes lived in low- and middle-income countries 1. Indonesia is ranked as having the seventh-largest number of DM patients in the world, and the number of people with diabetes was 10.7 million (6.2 %) of the total population in 2019 1. DM caused 4.2 million deaths and at least USD 760 billion in health expenditure in 2019-10 % of total spending on adults 1. Diabetic foot complications constitute a major health burden, amounting to the single most substantial reason for hospitalization among diabetic patients. Up to 2-3 % of DM patients are thought to have an active foot ulcer with a lifetime risk of developing complications 2,3. The International Diabetes Federation states that 9.1 to 26.1 million people with diabetes will suffer from a diabetic foot ulcer (DFU) each year 4,5.
DFU is described as a full-thickness lesion appearing on the skin on the feet of people with diabetes, along with infection, and destruction of tissues due to neuropathy or peripheral artery disease (PAD) 6. Concerning long-term conditions, a DFU may ultimately prompt lower extremity amputation (LEA), thus reducing patients’ quality of life 7. DM had increased 11 times the incidence of foot ulcers, accounted for more than 80 % of all amputations, and risen hospital costs more than 10-fold 8-10. Most DFUs are asymptomatic at the beginning, and patients start to recognize it until non-healing ulcers become evident 11. Therefore, wound healing becomes longer and cause high medical costs. The improvement, innovation, and prevention agenda further highlights the need for better efforts on active chronic disease management to optimizing the utilization of healthcare resources.
The previous study reported that discomfort due to a DFU is the most common complaint among patients and significantly impacts the wound healing process 12. Discomfort refers to the attributes of communication, family and relationship, functionality, self-identity, physical and psychosocial symptom relief, spiritual activities and states, safety and security 13. Discomfort means unfulfilled human basic needs individually and holistically 14. Pain, stress, bad smell, sleep disorder, and daily activities disturbances were the most common complaints by patients with a DFU 11,12. Previous studies reported that feeling discomfort could affect the wound healing process 14,15. However, discomfort receives less attention from health care providers. Therefore, achieving a good quality of wound care requires that the nurse care for patients physically and psychologically. The purpose of this study is to explore wound severity, discomfort, and psychological problems (stress, anxiety, and depression) and its interaction in patients with a DFU.
Methods
Study design
The cross-sectional study design was employed to explore wound severity, discomfort, and psychological problems of patients with a DFU. This study was conducted at the inpatient of three public hospitals in Jakarta and one wound care clinic in Indonesia from January 2018 to September 2018. The hospitals in Jakarta take care of 300-350 DM patients (with or without DFUs) daily.
Participants
The study sample consisted of 140 patients with a DFU. The sample size was calculated using a rule of thumb, namely, 5 to 50 respondents for each variable being researched 16. The inclusion criteria were patients with a DFU, having a stable hemodynamic status, able to communicate in Bahasa, and willing to be respondents. A convenience sampling technique was used to select the participants.
Measures
Demographic characteristics and clinical information were collected, including age, gender, education level, marital status, working status, monthly income, body mass index, duration of the DFU, type of wound dressing, and smoking status.
The Bates-Jensen wound assessment tool (BWAT) was used to measure a chronic wound. This instrument consists of 13 indicators: wound size, depth, edges, undermining, necrotic tissue type and amount, exudate type and amount, skin color surrounding wound, peripheral tissue edema and induration, granulation tissue, and epithelialization. This instrument uses a Likert scale from 1 to 5 (1 being the healthiest and 5 the unhealthiest attribute for each characteristic). A score ranging from 1 to 12 indicates a good condition of the wound, 13 to 56 regeneration stage, and more than 60 wound degeneration 17. The reliability in the current study was 0.763.
The discomfort evaluation of wound instrument (DEWI) was used to evaluate the discomfort of patients with a DFU. The authors and colleagues developed this instrument in 2015. It consists of 11 items including the general perception of discomfort, physical discomfort (wound severity, pain, itching, fluid, odor), the physical impact of discomfort (immobility, frequency of changing dressing), the psychological impact of discomfort (frustration, anxiety due to injury), and worship disruption. In the current study, the content validity index was 0.83, and the factor loading ranged from 0.257 to 0.658.
The depression, anxiety, and stress scale (DASS) is a questionnaire that contains 21 items to measure negative emotional states: depression, anxiety, and stress. The total score was categorized as follows; normal (0-19), mild (30-59), moderate (60-89), severe (90-119), and very severe (> 120) 18. The reliability in the current study was 0.815.
Data collection procedure
Ethical approval was obtained from the ethical committee of the faculty of nursing, Universitas Indonesia, before data collection (E234O20). One research assistant was mutually trained for data collection. Participants were invited to join the study during their clinical visits and while hospitalized in the studied hospitals. Written informed consent was obtained from the participants involved. The researcher personally provided a questionnaire to the respondents and filled it out according to their answers. The time needed to fill out all questions was 10 to 20 minutes. All data were collected anonymously, and no personal identifiers were recorded.
Data analysis
Descriptive statistics were used to explore the discomfort of patients with a DFU. Categorical data were represented as count and proportion, while continuous data were indicated as mean and standard deviation or as median and interquartile range. A bivariate analysis was performed before path analysis to evaluate the correlation among variables. A path analysis was carried out to examine the interaction between wound severity, discomfort, and psychological problems. The Statistical Package for Social Sciences (SPSS 22.0, IBM, Chicago, Illinois) software was used for statistical analysis.
Results
Of 140 participants included in this study, 53.6 % were female and 91 % were married. More than half (52.2 %) were 55 and older, the mean age being 50.23 (SD: 7.82). Of the patients, 60 % had an educational level above senior high school and 51.1 % were government officers, with more than 60 % earning less than USD 341 or 5 million Rupiahs a month. For the clinical indicators, more than half were overweight to obese, non-smokers, and having a DFU of less than four weeks (Table 1). The means were as follows: discomfort 2.35 (SD = 0.33), depression (1.34 ± 0.41), stress (1.49 ± 0.48), and anxiety (1.43 ± 0.40) (Table 2). The average score of wound severity was 31.35 ± 9.96.
Table 1 Demographic and clinical information of patients with a DFU (n = 140)
| Variables | N (%) | |
|---|---|---|
| Age (year, mean ± SD) | 50.23 ± 7.82 | |
| < 55 years | 67 (47.8) | |
| > 55 years | 73 (52.2) | |
| Gender | ||
| Male | 65 (46.4) | |
| Female | 75 (53.6) | |
| Education level | ||
| Not at all | 7 (5) | |
| Under senior high school | 49 (35) | |
| Above senior high school | 84 (60) | |
| Marital status | ||
| Single | 13 (9.3) | |
| Married | 127 (90.7) | |
| Working status | ||
| Unemployed | 78 (55.7) | |
| Government officer | 52 (44.3) | |
| Monthly income (Rupiah) | ||
| Rp 0 - 3 million | 88 (62.8) | |
| Rp 3 - 5 million | 38 (27.1) | |
| > Rp 5 million | 14 (10.1) | |
| Body mass index | ||
| Underweight-normal | 66 (47.8) | |
| Overweight-obesity | 72 (52.2) | |
| Duration to date | ||
| < 4 weeks | 82 (59.4) | |
| > 4 weeks | 56 (41.6) | |
| Type of wound dressing | ||
| Conventional | 65 (46.4) | |
| Modern | 75 (53.6) | |
| Smoking status | ||
| Yes | 49 (35) | |
| No | 91 (65) | |
Source: Own elaboration.
Table 2 Score of discomfort, depression, stress anxiety, and wound severity among patients with a DFU (n = 140)
| Variables | Mean | SD | 95 % CI |
|---|---|---|---|
| Discomfort | 2.35 | 0.33 | 2.29-2.41 |
| Depression | 1.34 | 0.41 | 1.28-1.41 |
| Stress | 1.49 | 0.48 | 1.41-1.57 |
| Anxiety | 1.43 | 0.40 | 1.37-1.50 |
| Wound severity | 31.4 | 9.96 | 29.7-33.0 |
Source: Own elaboration.
Figure 1 depicts the top three prevalence of discomfort experienced by patients with a DFU. Mobility problems were identified as the most frequent discomfort, followed by sleep disturbance and pain. More specifically, patients have reported difficulty in walking (52.6 %), difficulty in doing daily activities (48.6 %), waking up easily (32.9 %), and throbbing pain (50 %).
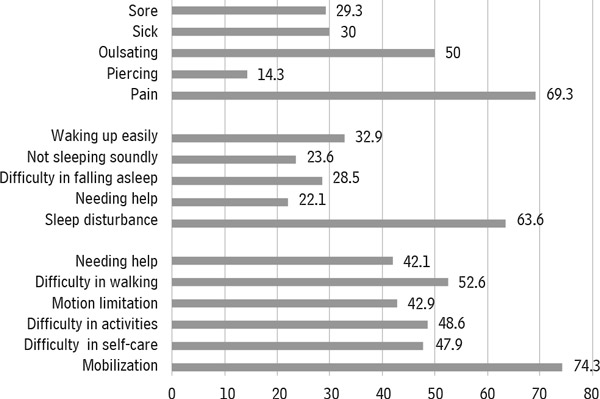
Source: Own elaboration.
Figure 1 Top three prevalence of physical discomfort characteristics of patients with diabetic foot ulcer (n=140)
The analysis showed a significant correlation between wound severity, discomfort, and psychological problems (p < 0.005). The discomfort was significantly associated with psychological problems, including stress, depression, and anxiety (p < 0.005). Table 3 shows that discomfort partially mediated the relationship between wound severity and psychological problems. In step 1, wound severity was significantly associated with discomfort, whose total effect was 0.41. In step 2, the impact of wound severity on psychological problems reduced but continue to be significant when the discomfort was entered in the model. The indirect effect of wound severity and psychological problems, as mediated by discomfort, was 0.11. In step 3, psychological problems were significantly associated with discomfort, whose direct effect was 0.72.
Table 3 Interaction between wound severity, DASS, and discomfort in patients with a DFU (n = 140)
| Coeff. | 95% CI | p-value | |
|---|---|---|---|
| Wound-Discomfort | 0.41 | 0.24-0.55 | < 0.001 |
| Wound-Discomfort-DASS | 0.11 | -0.05-0.26 | 0.05 |
| DASS-Discomfort | 0.72 | 0.54-0.87 | < 0.001 |
Note: DASS=depression, anxiety, and stress scale
Source: Own elaboration.
Discussion
Most subjects in this study were at a moderate level of wound severity. This study was supported by a previous study that reported a high prevalence of moderate level of wound severity in patients with a DFU 19. A DFU is a chronic wound that occurs due to vascular disorders, neuropathy, and immunosuppression and entails a high medical cost 20,21. DFUs could quickly develop into infections because high blood glucose becomes the right place for microorganism growth 22. Over 85 % of major amputations in patients with diabetes are preceded by foot ulceration 23. A moderate level of wound severity could affect the individual’s daily activity and may need some help from caregivers or family. Health care professionals need to provide an education to them regarding how to do their daily activities and increase social support to help patients with DFU. Also, preventative strategies, including annual diabetic foot screening and diabetic foot care interventions facilitated by a multidisciplinary team, should be implemented to enable early identification of diabetic patients at high risk of diabetic foot complications.
Patients with DFU experienced discomfort, specifically immobilization, sleep disturbance, and pain. The previous study reported that chronic wounds caused discomfort, including pain and difficulty in doing daily activities 24. The previous study suggested that providing physical comfort was necessary, and the main factors disrupting physical comfort were pain, noise, sleep disturbance, and immobilization 25. Although comfort may have a different meaning to different people, the previous study highlighted comfort significantly affected wound healing, reduced symptom burden, and improved daily activities and quality of life 26. However, the feeling of discomfort may be affected by cultural differences and gender issues; e.g., in Indonesia, men are expected to be strong, thus if they complain about something like discomfort, they may be considered weak. The interventions to manage a wound in patients with DFUs should enhance comfort level and consider the discomfort in male patients.
This study found that psychological problems, including anxiety and stress, were also reported by the patients with a DFU. Several studies have reported that patients with chronic wounds feel fear and anxiety about a long process of wound healing or even getting an amputation 15,25. However, previous studies did not include stress as an independent factor. The previous study also found that stress and depression are independent risk factors for the development of diabetic ulcers and increase the risk of death in patients with diabetic ulcers despite controlling glucose levels, diabetic ulcer severity, smoking, socioeconomic conditions, and other factors 15. Patients can feel stressed because of the pressure and situations they experience. Therefore, support from family is critical to helping patients to adjust and be more confident to take care of themselves.
The relationship between wound severity and psychological problems was mediated by discomfort. No previous study has been conducted to explore the mediating effect of discomfort on stress and psychological problems. Respondents experienced stress from moderate to severe, associated with higher degeneration of diabetic ulcers 19. There is a difference between discomfort and psychological problems. Discomfort is a direct and immediate feeling or general perception about the environment, while psychological problems are a feeling or perception that takes long to be perceived or experienced 11. According to Nurachmah et al. 26, someone who is injured will feel an imperfection, which ultimately results in emotional disturbances such as stress, anxiety, and depression. Wound care for patients with diabetic foot also needs to focus not only on the wound healing but also on the psychological problems and discomfort of patients. A comprehensive assessment of the psychological aspect should be integrated into wound care intervention.
Limitation
The limitation of this study is that the findings may not be generalized to the various patients in Indonesia because this study only collected data from three referral hospitals in Indonesia, and the country has 34 provinces distributed in more than seven big islands. Nonetheless, although selection bias in this research cannot be ruled out, our study recruited participants from two tertiary hospitals, which have similar demographic characteristics as to patients with a DFU across Indonesia.
Conclusion
In conclusion, this study indicated that patients with DFU experienced physical discomfort and psychological problems. The relationship between wound severity and psychological problems was mediated by discomfort. Future studies should explore more interaction models of discomfort in patients with DFUs using a longitudinal follow-up. Early identification of DFU severity and psychological problems should be integrated into wound care management.

