











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Syphilis, although an infection that is easy to diagnose and treat, still represents a serious public health problem. Characterized as a worldwide spreading disease, it affects nearly six million people annually, aged between 15 and 49 years old. Its reservoir is the contaminated human being, and transmission occurs mainly through sexual intercourse, without using a condom, with an infected individual or through vertical transmission during pregnancy1.
Of the several diseases that can be transmitted during the pregnancy-puerperal cycle, syphilis has the highest rates of congenital infection, with a 70 % to 100 % possibility of vertical transmission of this condition in the primary and secondary stages of maternal syphilis, decreasing to 30 % in the late and tertiary latent phases2.
Congenital syphilis is the infection of the fetus predominantly by the transplacental route by Treponema pallidum and it occurs in pregnant women who are not treated or treated inadequately, which can cause serious consequences such as spontaneous abortion, prematurity, stillbirth, death, in addition to psychological and social repercussions for the family and society3.
When observing the epidemiological panorama of congenital syphilis, an increase in the number of cases of this condition is evidenced. While the Pan American Health Organization's recommendation for Latin America and the Caribbean estimates 0.5 cases per 1,000 live births, the Brazilian rate is 6.54, considered 13 times higher.
In this context, the number of research studies related to the topic also rose. The occurrence of congenital syphilis has already been associated, among other factors, with the younger age group and the woman's low schooling5, as well as with late diagnosis of the pregnant woman and her partner 6. However, the search for factors related to congenital syphilis from the prenatal care process, with indirect assessment of the quality of care provided to pregnant women, is still incipient.
Even with the improvement of access and the proportion of coverage of prenatal care in the country, only a small percentage of women receive adequate assistance during pregnancy, which contributes to the occurrence of preventable injuries and unnecessary hospitalizations7, as is the case of congenital syphilis.
Thus, this study assumes that a qualified and timely prenatal care for the pregnant woman and her partner would reduce the number of congenital syphilis cases and of hospitalizations of neonates/children for treatment. The findings can provide subsidies to identify factors that can be improved in the area and help the professionals who provide prenatal care to insert new conducts and routines in the care of women. Thus, this study aims to identify the factors associated with hospitalizations due to congenital syphilis in neonates, based on the characteristics of prenatal care.
Materials and method
A case-control study carried out with puerperal women over 18 years old, with their newborns admitted to a reference hospital in mid- and high-complexity care of southern Brazil.
For the selection of the participants, the following inclusion criteria were respected: puerperal women who had a single child in the current pregnancy diagnosed with congenital syphilis after birth, users of the Unified Health System (Sistema Único de Saúde, SUS), and seen at the obstetrics service of the hospital when the pregnancy was resolved. For the selection of the controls, puerperal women with characteristics homogeneous to those included in the case group, and with a newborn without a congenital syphilis diagnosis, were considered. Only the main diagnosis recorded in the hospital admission authorization was considered.
Data collection by means of questionnaires with the mothers during the newborn's hospitalization occurred between July and November 2017. There was no refusal by the subjects to participate in the study. At the time of the interview, the medical records of the newborns and of the puerperal women were also obtained, in addition to the prenatal cards of the pregnant women. A pilot study was carried out for the adequacy and validation of the data collection instrument, built exclusively for this research. The instrument had socioeconomic, demographic and lifestyle habit variables, as well as related to reproductive history and assistance during prenatal care.
The inpatient unit was visited from Monday to Friday. The sociodemographic and economic characteristics, lifestyle habits, the variables of reproductive history and the evaluation of the prenatal care process were defined as independent variables in relation to the outcome of the study. To obtain the gestational age at birth, the one recorded in the newborn's medical record was adopted.
Sample calculation was performed using the Epilnfo 6.0 program, with the formula for case-control studies8. From the number of cases that totaled 13 in the collection period and considering a maximum type I (alpha) error of 5 %, a minimum statistical power of 80 %, and a 5 % exposure between controls, 52 controls were necessary. According to the epidemiological assessment of congenital syphilis cases in other studies and in view of a discrepant observation between cases and controls, it was decided to use a 1:4 ratio.
The cases group (n = 13) included the newborns diagnosed with congenital syphilis and was compared with the control group (n = 52), representative of the absence of the disease. The controls were matched to the cases by age and parity (number of children) to minimize or eliminate the confounding effect.
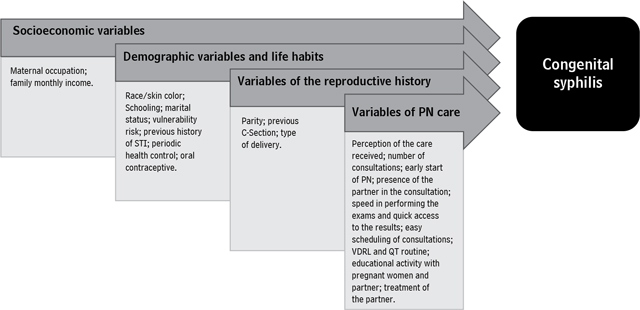
The hierarchical approach strategy and conditional logistic regression9 were used, whose regression coefficients represent the logarithms of the odds ratios, so as to try to explain the conceptual model of the occurrence of congenital syphilis. For the analysis, four hierarchical levels were considered, represented by the determinants of the distal, intermediate I and II, and proximal levels (Figure 1). The distal level consisted of the socioeconomic variables; the intermediate level was subdivided into I (demographic factors and lifestyle) and II (reproductive history), and the proximal level comprised variables related to the prenatal care process.
The hierarchical approach and conditional logistic regression allow quantifying the contribution of each hierarchical level and minimizing the underestimation of the effects of risk determination. The set of the variables of one level was analyzed independently from those of other levels and integrated the adjustments of the variables of subsequent levels, when statistically significant (p < 0.05); the same order was adopted for the other levels. The variables were maintained in the final model when the adjustments were adequate. The modeling process was composed of the selected variables.
A situation of risk and vulnerability was considered when an affirmative answer was given to any of these habits: smoking, alcohol, drugs, tattoos, piercing and more than two partners in the last year. For the periodic health control variable, gynecological or health professional monitoring before pregnancy was considered.
In addition, the variables investigated regarding the prenatal care process were the following: a) number of prenatal consultations (obtained by counting the records of the dates of the consulfations and considered adequate according to the gestational age [GA]); b) GA in weeks; c) early beginning of prenatal care (up to the 13th week); d) minimum of six consultations carried out adjusted according to the GA, considering it appropriate to hold one in the first trimester, two in the second trimester (from the 14th to the 27th week) and three in the third trimester (from the 28th week); e) obstetric clinical conduct (the measurement of blood pressure, weight, the measurement of the height of the uterine fundus and the recording of cardiofetal beats in all consultations considered adequate); f) complete vaccination schedule (considered appropriate due to the presence of vaccine records against tetanus, hepatitis B and influenza); g) laboratory tests (basic tests considered complete: blood typing, toxoplasmosis, HIV/AIDS, VDRL, hepatitis B, blood count, partial urine, urine culture and fasting blood glucose). All these aspects were assessed in a dichotomous way (for example: yes or no, adequate or inadequate, complete or incomplete), judged according to the guidelines recommended by the Brazilian Ministry of Health in assisting pregnant women10.
The data were entered with double entry and the statistical analysis was performed using the SPSS 20 software. The logistic regression analysis was conducted according to the plan proposed in the hierarchical approach. Logistic regression was used for each of the blocks of variables. For all the inferential statistical tests, a significance level of p < 0.05 was used. The quality of fit was assessed by the Hosmer-Lemeshow test. The multicollinearity assumption test was performed by the VIF (Variance-Inflation Factor) and calculated by multiple linear regression, adopting a VIF > 4 as the cutoff point for multicollinearity. The test showed no evidence of the presence of multicollinearity among the independent variables studied for multiple logistic regression.
The study was conducted observing the ethical standards and approved by the Committee of Ethics in Research with Human Beings of the Federal University of Fronteira Sul, under opinion No. 2,157,128 and Certificate of Presentation for Ethical Appreciation No. 69347917.9.0000.5564.
Results
Among the hospitalizations of children under one year old, 20 % (n = 13) were due to congenital syphilis; while among the controls, 80 % (n = 52) were due to other causes (respiratory tract infection: 36.5 %, prematurity: 25 %, jaundice:17.3 %, other causes: 21.1 %).
The mean age of the puerperal women was 24.1 years old (SD = 6.1) and the mean age of sexarche was 15.6 years old (SD = 1.3). In this study, the socioeconomic factors (distal hierarchical level) did not show an association with the occurrence of the outcome (Table 1). The intermediate level I and II variables - vulnerability risk, previous history of sexually transmitted infection (STI), use of oral contraceptives and parity - were significantly associated with the occurrence of hospitalizations (Table 2).
Table 1 Distribution of congenital syphilis cases according to the association between the variables of the distal hierarchical level, Brazil, 2017
| Variables | Case n = 13 (%) | Control n = 52(%) | Total n = 65 (%) | p-value |
|---|---|---|---|---|
| Maternal occupation | 0.280 | |||
| With an employment contract | 3 (23.1) | 13 (25) | 16 (24.6) | |
| Without an employment contract | 10 (76.9) | 39 (75) | 49 (75.4) | |
| Family monthly income | 0.306 | |||
| < 4 minimum wages | 11 (16.9) | 42 (64.6) | 53 (81.5) | |
| > 4 minimum wages | 2* (3.1) | 10 (15.4) | 12 (18.5) | |
* Chi-square test, with Yates correction. Source: Own elaboration.
Table 2 Distribution of congenital syphilis cases according to the association between the variables of the intermediate hierarchical levels I and II, Brazil, 2017
| Variables | Case n = 13 (%) | Control n = 52 (%) | Total n = 65 (%) | p-value |
|---|---|---|---|---|
| Intermediate level I | ||||
| Race/Skin color | 0.185 | |||
| White | 6 (9.2) | 30 (46.2) | 36 (55.4) | |
| Brown/Black/Asian | 7 (10.8) | 22 (33.8) | 29 (44.6) | |
| Maternal schooling | 0.193 | |||
| Up to 8 years | 9 (13.8) | 30 (46.2) | 39 (60) | |
| > 8 years | 4* (6.2) | 22 (33.8) | 26 (40) | |
| Marital status | 0.124 | |||
| Has a partner | 12 (18.5) | 43 (66.2) | 55 (84.6) | |
| No partner | 1* (1.5) | 10 (15.4) | 10 (15.4) | |
| Variables | Case n = 13 (%) | Control n = 52 (%) | Total n = 65 (%) | p-value 0.036 |
| Yes | 9 (13.8) | 20 (30.8) | 29 (44.6) | |
| No | 4* (6.2) | 32 (49.2) | 36 (55.4) | |
| Previous history of STI | 0.006 | |||
| Yes | 7 (10.8) | 8 (12.3) | 15 (23.1) | |
| No | 6 (9.2) | 44 (67.7) | 50 (76.9) | |
| Periodic health control | 0.201 | |||
| Yes | 6 (9.2) | 29 (44.6) | 35 (53.8) | |
| No | 7 (10.8) | 23 (35.4) | 30 (46.2) | |
| Oral contraceptive | 0.011 | |||
| Yes | 11 (16.9) | 24 (36.9) | 35 (53.8) | |
| No | 2* (3.1) | 28 (43.1) | 30 (46.2) | |
| Intermediate level II | ||||
| Parity | 0.043 | |||
| Primiparous | 5 (7.7) | 35 (53.8) | 40 (61.5) | |
| Multiparous | 8 (12.3) | 17 (26.2) | 25 (38.5) | |
| Previous C-Section | 0.127 | |||
| Yes | 7 (10.8) | 37 (56.9) | 44 (67.7) | |
| No | 6 (9.2) | 15 (23.1) | 21 (32.3) | |
| Type of delivery | 0.071 | |||
| Vaginal | 6 (9.2) | 12 (18.5) | 18 (27.7) | |
| Cesarean | 7 (10.8) | 40 (61.5) | 47 (72.3) | |
*Chi-square test, with Yates correction
#Considering smoking, alcohol, drugs, tattoos, piercing and number of partners in the last year greater than two.
Source: Own elaboration.
Of the variables related to the prenatal care process: 84.6 % (n = 55) positively evaluated the care received in primary care and 75.4 % (n = 49) stated that they had an easy time making appointments for care. The absence of the partner during the consultations (53.8 %), associated with their non-participation in educational activities (40 %), was directly associated with the outcome (Table 3).
Table 3 Distribution of congenital syphilis cases according to the association between the variables of the proximal hierarchical level, Brazil, 2017
| Variables | Case n = 13 (%) | Control n = 52 (%) | Total n = 65 (%) | p-value |
|---|---|---|---|---|
| Perception of the care received | 0.214 | |||
| Positive | 10 (15.4) | 45 (69.2) | 55 (84.6) | |
| Negative | 3* (4.6) | 7 (10.8) | 10 (15.4) | |
| Number of consultations | 0.083 | |||
| Sufficient | 5 (7.7) | 32 (49.2) | 37 (56.9) | |
| Insufficient | 8(12.3) | 20 (30.8) | 28 (43.1) | |
| Early start of PN | 0.185 | |||
| Yes | 8(12.3) | 38 (58.5) | 46 (70.8) | |
| No | 5 (7.7) | 14 (21.5) | 19 (29.2) | |
| Presence of the partner in the consultation | 0.028 | |||
| Yes | 11 (16.9) | 24 (36.8) | 35 (67.3) | |
| No | 2* (3.1) | 28 (43.1) | 30 (53.8) | |
| Speed in performing the exams | 0.099 | |||
| Yes | 5 (7.7) | 31 (47.7) | 36 (55.4) | |
| No | 8(12.3) | 21 (32.3) | 29 (44.6) | |
| Quick access to the results | 0.285 | |||
| Yes | 10 (15.4) | 40 (61.5) | 50 (76.9) | |
| No | 3* (4.6) | 12 (18.5) | 15 (23.1) | |
| Easy scheduling of consultations | 0.280 | |||
| Yes | 10 (15.4) | 39 (60) | 49 (75.4) | |
| No | 3* (4.6) | 13 (20) | 16 (24.6) | |
| VDRL* at 1st and 3rd trimester | 0.053 | |||
| Performed | 11 (16.9) | 30 (46.2) | 41 (63.1) | |
| Not performed | 2* (3.1) | 22 (33.8) | 24 (36.9) | |
| Syphilis rapid test | 0.035 | |||
| Performed | 1* (1.5) | 19 (29.2) | 20 (30.8) | |
| Not performed | 12 (18.5) | 33 (50.8) | 45 (69.2) | |
| Educational activity of the mother | 0.162 | |||
| Yes | 2* (3.1) | 16 (24.6) | 18 (27.7) | |
| No | 11 (16.9) | 36 (55.4) | 47 (72.3) | |
| Educational activity of the partner | 0.033 | |||
| Yes | 2* (3.1) | 24 (36.9) | 39 (60) | |
| No | 11 (16.9) | 28 (43.1) | 26 (40) | |
| Treatment of the partner | ||||
| Performed | 5 (7.7) | 0* (0) | 5 (7.7) | |
| Not performed | 8(12.3) | 52 (80) | 60 (92.3) | |
*Chi-square test, with Yates correction # VDRL - Venereal Disease Research Laboratory.
Source: Own elaboration.
It is noteworthy that all the patients diagnosed with syphilis (confirmed by the positive VDRL test) were referred to high-risk prenatal care and properly treated (84.6 % in the second trimester and 15.3% in the third trimester), according to the protocols in force in the country. However, only five of the partners were treated.
Table 4 shows the characteristics of the hospitalized neonates (cases and controls). The mean birth weight was 2,897 g (SD = 719 g).
Table 4 Characteristics of the hospitalized neonates according to the association with the occurrence of congenital syphilis, Brazil, 2017
| Variables | Case n = 13 (%) | Control n = 52 (%) | Total n = 65 (%) | p-value |
|---|---|---|---|---|
| Low birth weight | 0.025 | |||
| Yes | 8 (12.3) | 15 (23.1) | 23 (35.4) | |
| No | 5 (7.7) | 37 (56.9) | 42 (64.6) | |
| Gestational age | 0.078 | |||
| Preterm | 5 (7.7) | 9 (13.8) | 14 (21.5) | |
| Term | 8 (12.3) | 43 (66.2) | 51 (78.5) | |
| Exclusive breastfeeding | 0.036 | |||
| Yes | 9 (13.8) | 4* (6.2) | 29 (44.6) | |
| No | 20 (30.8) | 32 (49.2) | 36 (55.4) | |
| Skin-to-skin contact | 0.043 | |||
| Yes | 5 (7.7) | 35 (53.8) | 40 (61.5) | |
| No | 8 (12.3) | 17 (26.2) | 25 (38.5) | |
* Chi-square test, with Yates correction.
Source: Own elaboration.
Discussion
In this study, it was sought to identify the factors associated with the occurrence of congenital syphilis, in addition to proving that a qualified and timely prenatal care for the pregnant woman as well as for the partner would reduce the number of cases and of hospitalizations of neonates/children for the treatment. Maternal occupation and family monthly income (socioeconomic variables) were not associated with the outcome, despite knowing that the health and disease process can be socially modified. The findings of this study refute what is shown in the literature11, which can be explained by the social characteristics of women with better living conditions in the Brazilian South region.
In turn, the following were associated with the occurrence of congenital syphilis: vulnerability risk, previous history of STI, use of oral contraceptives and parity, in the light of other studies12-14. Vulnerability is understood as the possibility of exposing people to illness resulting not only from a set of individual aspects, but also from collective and contextual factors that make individuals more susceptible to the availability of resources to protect themselves15.
The use of drugs, understood as a situation of vulnerability in this study, increases the likelihood of involvement with multiple sexual partners, which, associated with the non-use of barrier contraceptive methods, can result in risk of STI contamination, in addition to unwanted pregnancies15.
On the one hand, being single can be related to the multiplicity of sexual partnerships and the risk of unprotected sexual activity. On the other hand, the trust conferred on the steady partner means that the woman does not use the condom or stops demanding its use. These combined facts underscore the low adherence to the STI preventive methods, which contributes to the uncontrolled spread of the disease15. It is added that the use of oral contraceptives by itself does not have a clinical correlation with the occurrence of the outcome, but reinforces the practice of unsafe sex since, for these women, the choice of the contraceptive method can be based only on contraception.
The number of children (parity) seems to have the same causal link, since multiparous women are at greater risk for the occurrence of congenital syphilis, as a result of the greater number of unprotected sexual relations. A research study carried out in Pakistan corroborated with the findings that parity and the use of contraceptives are related to greater occurrence of syphilis 14.
The absence of the partner in the consultation and his limited participation in the educational activities seem to be associated with the occurrence of congenital syphilis. It is necessary to intensify strategies that integrate and favor the partner's adherence to prenatal care during pregnancy. The partner's prenatal care is intended to promote the engagement of men in the actions of reproductive planning and in the monitoring of prenatal, childbirth and postpartum of their partners and in the care of the child's development, with the real possibility of improving the quality of life for all people involved and healthy affective bonds16.
Although the timely treatment of the partner is not associated with the occurrence of the outcome in this study, other studies identified that the occurrence of syphilis resulted, among other factors, from untreated sexual partners and inadequate treatments, which demonstrates the potential for dissemination related to the therapeutic regimen 5,17.
Another factor evidenced in the occurrence of the outcome was failure to perform the rapid test for syphilis, in the light of another study4. The offer of the rapid test, whether for the detection of syphilis or any other STI covered by the test, must be performed at any opportunity to assist the woman and her sexual partners. It is a resource that is easy to implement, yet highly cost-effective, considered an important tool in the diagnosis and early treatment of pregnant women and their partners17. Some characteristics have already been related to a greater chance of not undergoing the rapid test, such as black-skinned women, with low family income and schooling, in addition to few prenatal consultations4.
Another important factor evidenced by the study was the neonatal outcome. Despite the high number of congenital syphilis, the newborns in this study had a low degree of asphyxia and a reduced proportion of congenital malformations. Low birth weight was associated with the occurrence of congenital syphilis, in line with the findings described in the literature, which emphasize that, in addition to reduced weight, prematurity, stillbirth, neurological sequelae, and death can be seen in children with this condition11.
In addition, through the findings of this study, it was possible to show that the non-routine practice of skin-to-skin contact at birth, as well as the non-incentive to exclusive breastfeeding were associated with the presence of congenital syphilis. It is worth noting that breast milk does not transmit syphilis from the mother to the child and that, during breastfeeding, transmission can occur only if there is syphilitic breast injury, which is very rare18.
The same criterion applies to skin-to-skin contact, since Treponema pallidum is acquired by crossing the placenta or through direct contact of the child with an infected lesion at birth19.
Nevertheless, the type of delivery was not associated with the outcome. However, 72.3 % of the births were performed surgically, which may have explained the failure in the routine of skin-to-skin contact, as well as exclusive breastfeeding in high proportions.
It should also be noted that, even in a relatively short collection period, the number of congenital syphilis cases diagnosed was considerable, in view of all the efforts directed at educational measures, which can and should be implemented and provided in prenatal care.
Conclusions
Through the objectives proposed for this study, it was possible to identify that congenital syphilis presents several risk factors for its occurrence, both those socially identified in the literature and those related to the specific characteristics of the pregnant women. It was also possible to observe that the assistance inequalities existing in care, during the prenatal consultations, directly reflect on the occurrence of this condition.
In this sense, there is a need for Nursing to be more active in prenatal care, with the execution of consultations, investigation of health problems and educational activities for the couple, as well as early performance of rapid tests to identify the condition, in a timely manner and for complete treatment.
This study has some limitations: It is noteworthy that the hospitalizations analyzed were only those that occurred within the scope of the SUS, which constitutes a partial view of reality, in addition to the small population of cases studied, which limits the generalization of the findings. It is suggested to carry out future studies that include hospitalizations from the private system, with a view to comparing the factors associated with the occurrence of congenital syphilis in different areas.

