











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
According to the WHO1, Diabetes Mellitus is a chronic disease that develops when the pancreas does not produce sufficient insulin or when the organism is not able to use it effectively; according to world statistics, by 2017, 425 million people presented this pathology and there were four million deaths, being the fourth cause of death in Latin America2.
According to the Colombian Health Situational Analysis corresponding to the same year, Diabetes Mellitus was the sixth cause of death with a mortality rate of 34.18 per 100,000 inhabitants and with 1,099,417 people affected by the disease, the rate being higher in women (58.9 %). The cases reported by the Northern Santander department were 29,516 with a prevalence of 2.1%, ranking 12th at the national level3; in the Erasmo Meoz University Hospital, 1,018 diabetic patients were recorded who were seen in the Internal Medicine service and its specialties.
Hospital readmissions represent a problem of major relevance for the health services worldwide; in Catalonia, the mean of readmissions due to Diabetes Mellitus complications in 2016 was 4.6%4. A study conducted in Colombia revealed that 1 out of 10 patients are readmitted within 30 days, generating a longer stay in comparison with their first admission5.
Diabetes Mellitus is a pathology in which outpatient treatment is easily interrupted by the patients, making them susceptible to presenting complications such as retinopathy, nephropathy, neuropathy, and cardiovascular diseases that need hospitalization and alter the biopsychosocial sphere; this implies a major challenge since diagnosis represents important changes in lifestyle since, without adequate educational support, the outcomes can be anxiety, depression, and deterioration in the quality of life, which is translated into decreased self-care6. The aforementioned can be avoided with timely support in disease management, this being one of the Nursing staff’s competencies, thus managing that the patients understand their disease and adhere to the treatment to prevent possible readmissions.
To reduce the number of complications, the Pan American Health Organization (PAHO)7 launched an action plan for the prevention and control of non-communicable diseases in the American continent (2013-2019), thus urging to introduce mechanisms that improved care quality, follow-up, and assessment with interventions targeted at the control of non-communicable diseases.
According to Dorothea Orem’s theory, one of the desired objectives is to enhance the self-care activities in the patient using the supporting educational system, whose purpose is to offer guidance on the actions that must be performed in case of deviations from health, this being the approach for implementing the preparation plan for hospital discharge.
Internationally, in Spain, Mexico and Ecuador, studies have been conducted in which it is shown that health education at discharge and phone follow-up manages to reduce the number of complaints and hospital readmissions, thus increasing therapeutic adherence and self-care; it is considered that this process must be led by the Nursing staff, not only providing the patients with recommendations for the subsequent medical controls but also explaining the disease process and how they must adjust the changes to their lifestyle8-11.
In Colombia, several projects have been developed centered on assessing self-care capacity and therapeutic adherence in patients with chronic diseases after the development of educational sessions, and studies have also been documented proposing the structure of a preparation plan for hospital discharge with the fundamental participation of the Nursing professional12-14.
In Northern Santander, no experiences of developments of this type of plan have yet been documented; the Erasmo Meoz University Hospital, a reference institution for the region, lacks a care plan for after hospital discharge targeted at diabetic patients to provide the information that the patient and primary caregiver need to prevent readmissions due to the disease complications.
Because of the above, gaps are evidenced concerning the implementation of preparation plans for hospital discharge at the local level, the reason why the following research question was set forth: Does the application of the preparation plan for hospital discharge generate any effect on adherence to treatment and the self-care agency capacity in patients with Diabetes Mellitus?
Materials y methods
This paper is a longitudinal and quasi-experimental study guided by Dorothea Orem’s theory on the development of a preparation plan for hospital discharge in patients with Diabetes Mellitus. Patients who met the following criteria were included:
Individuals come of age (18 years old or over).
Having been admitted to the health institution in the period from June to September 2019.
Having been treated in the Internal Medicine, Specialty Surgery, or Urgency services of the Erasmo Meoz University Hospital.
Intentional or convenience sampling was employed as the recruitment phase was developed, which lasted 10 weeks. The sample size was calculated having as a reference the health institution’s databases with the admissions due to Diabetes Mellitus in the months before the study, estimating a total population of 120 individuals. A 95 % confidence level was proposed for the Z parameter, which adopts a value of 1.96; therefore, it was possible to handle a 5 % error margin, considering a 50 % success probability, and the result obtained was a sample of 90 individuals. Subsequently, during the follow-up phase, which lasted two months for each patient, two of them died during the process, continuing and ending the study with a sample of 88 patients; also, the study included the participation of 36 caregivers.
The execution was conducted in the following phases:
First phase: design of the ABC (Adherence to treatment, Providing knowledge, and Self-care capacity; from Spanish: “Adherencia al tratamiento, Brindar conocimientos and Capacidad de autocuidado”) of the preparation for hospital discharge in people with diabetes; recruitment, initial appraisal and assessment of the self-care agency capacity and of adherence to treatment in each of the services offered by the institution. The “therapeutic conduct: disease or lesion” instruments12 were used, with high reproducibility (0.98) and questions grouped in eleven indicators with Likert-type scale results, namely: 1 never, 2 rarely, 3 occasionally, 4 frequently, and 5 constantly shown; in addition, the “scale to assess the self-care agency capacity (ASA)” elaborated by Isemberg and Evers was implemented with a Cronbach’s alpha of 0.74; this scale was adapted and modified for Colombia in 2004 by Edilma De Reales15 and comprises five categories: very low self-care agency: 24-43, low self-care agency: 44-62, fair self-care agency: 63-81, and good self-care agency: 82-96.
Second phase: the preparation plan for hospital discharge was developed with education for self-care of the 88 patients and 36 caregivers who were present, and was conducted in the hospitalization services.
Third phase: follow-up was performed and an individual record was managed in Microsoft Excel for two months through phone calls every week; also, counseling was provided to the patients or, in case this was not possible, to the family member who answered the call, and home visits were conducted when the patients expressed doubts regarding their treatment, how to handle the glucose meter or the healings.
Fourth phase: home visits were conducted to perform the final assessment of the self-care agency capacity and therapeutic adherence, by applying the instruments used in the initial assessment with comparison purposes.
The ABC of the preparation for hospital discharge in people with diabetes was structured as follows: comprehensive assessment of the patients and the caregivers; patient assessment according to the health domains that fit their condition, by applying the following instruments or scales: Folstein’s Mini-Mental State Examination (MMSE)16, with eleven items that assess the cognitive function; Competence for care (CUIDAR)17 with 20 items that include six dimensions with stratification in high, medium and low ranges; the Lawton and Brody scale for the instrumental activities of daily living (IADLs)16 with a classification of 0-1: total dependence, 2-3: severe dependence, 4-5: moderate dependence, 6-7: slight dependence; and 8: independence, and with a reproducibility index of 0.94. Diabetic foot screening18 was also performed, classified as risk 0: without loss of protective sensation, without peripheral disease and deformities; risk 1: loss of protective sensitivity plus deformity; risk 2: loss of protective sensitivity plus peripheral disease; and risk 3: ulcer or amputation history. Similarly, Wagner’s scale19 was used for the classification of the existing ulcers on the diabetic patients’ feet. For the frequency of phone follow-up, the risk classification at discharge14 was used, which assessed the complexity of the care associated with the treatment with four items (number of medications > 5, parenteral administration route, control medication, and invasive devices); low risk was determined if these parameters were negative with medium or high competence for home care, and high risk was indicated if the patients presented at least one of these conditions and low or medium competence for home care.
Education to patients or caregivers was based on the application of the ABC (Treatment adherence, providing knowledge, and self-care capacity) educational methodology contained in the booklet-type support material that was developed by the researchers, which was socialized with the patients and the caregivers at the first meeting during 30 minutes, and later at the follow-up in another session of the same duration to reinforce knowledge and clarify doubts.
Referral to the support groups is only performed when criteria such as deterioration of the nutritional status, complications resulting from the disease, and changes in mental state are identified; it is worth noting that none of these cases was recorded in the study; therefore, no need for referrals arose. The frequency of the follow-up to be performed was determined according to the instrument for risk classification at discharge: if it was classified as low, follow-up was performed every 15 days and, if high, every week.
Data analysis was performed in Microsoft Excel 2016 and the Statistical Package for the Social Sciences (SPSS) software, version 22.0. With the presentation in tables and graphs, parametric (Student’s t for paired samples) and non-parametric (Wilcoxon) tests were used, considering p-values < 0.05 as statistically significant according to normality distribution in which the Shapiro-Wilk and Kolmogorov-Smirnov tests were applied, with a 95 % confidence level and a 5 % error margin. The following was set forth as an alternative hypothesis: the implementation of a preparation plan for hospital discharge manages to exert a positive effect on the self-care agency capacity and adherence to treatment in diabetic patients; in opposition, the null hypothesis was also proposed: the implementation of a preparation plan for hospital discharge has a null effect on the self-care capacity and adherence to treatment in diabetic patients.
Considering the ethical aspects, the research was classified in the category of research without risk; informed consent was applied, in which all aspects regarding the study were explained, both verbally and in written form. Likewise, the authors’ approval was obtained to use the instruments employed, as well as acceptance from the Ethics Committee of the health institution, always acting under the principles of autonomy, beneficence, and non-maleficence.
Results
A total of 88 individuals participated in the study; their sociodemographic characteristics are shown in Table 1: 53 % were women and the predominant age group was from 61 to 70 years old, with 34 %; the participants are married or in a consensual union, with 35 % each marital status; 33 % has complete elementary school, and 69 % is unemployed. Of the health characteristics shown in Table 2, it was found that 32 % have a diagnosis time of between 6 and 10 years and that 73 % present some comorbidity, with arterial hypertension (AHT) being the most frequent (50 %).
Table 1. Sociodemographic characterization
| Variable | n | % | |
|---|---|---|---|
| Gender | |||
| Male | 41 | 47 % | |
| Female | 47 | 53 % | |
| Age | |||
| 20-30 years old | 1 | 1 % | |
| 31-40 years old | 2 | 2 % | |
| 41-50 years old | 8 | 9 % | |
| 51-60 years old | 23 | 26 % | |
| 61-70 years old | 30 | 34 % | |
| 71+ years old | 24 | 28 % | |
| Marital status | |||
| Single | 15 | 17 % | |
| Married | 31 | 35 % | |
| Consensual union | 31 | 35 % | |
| Widowed | 7 | 8 % | |
| Separated | 4 | 5 % | |
| Schooling level | |||
| University | 1 | 1 % | |
| Technical | 1 | 1 % | |
| Complete high school | 9 | 10 % | |
| Incomplete high school | 14 | 16 % | |
| Complete elementary school | 29 | 33 % | |
| Incomplete elementary school | 25 | 29 % | |
| None | 9 | 10 % | |
| Occupation | |||
| None | 61 | 69 % | |
| Autonomous worker | 16 | 18 % | |
| Employee | 10 | 12 % | |
| Pensioner | 1 | 1 % | |
Source: The authors.
Table 2. Health characteristics
| Variable | n | % |
|---|---|---|
| Diagnosis time | ||
| 0-5 years | 22 | 26 % |
| 6-10 years | 28 | 32 % |
| 11-15 years | 18 | 20 % |
| 16-20 years | 12 | 13 % |
| 21-25 years | 6 | 7 % |
| 26 years or more | 2 | 2 % |
| Comorbidity | ||
| Yes | 64 | 73 % |
| No | 24 | 27 % |
| Pathologies | ||
| AHT (arterial hypertension) | 47 | 50 % |
| Circulatory diseases (CHF, heart failure, embolism, venous thrombosis, peripheral vascular disease, stroke) | 15 | 16 % |
| Renal diseases (CKD, UTIs, prostatic hyperplasia) | 10 | 11 % |
| Metabolic diseases (hypothyroidism, obesity) | 6 | 7 % |
| Musculoskeletal diseases (osteoarthrosis, arthritis) | 4 | 4 % |
| Pulmonary diseases (pneumonia, COPD, asthma, pleural stroke) | 4 | 4 % |
| Liver diseases (cirrhosis, hepatitis) | 3 | 3 % |
| Hematologic diseases (idiopathic thrombocytopenic purpura, anemia) | 2 | 2 % |
| Cancer (colon, leukemia) | 2 | 2 % |
| Diseases of the nervous system (Parkinson) | 1 | 1 % |
| BMI (Body Mass Index) | ||
| Underweight | 6 | 7 % |
| Normal | 36 | 41 % |
| Overweight | 28 | 32 % |
| Obesity | 18 | 20 % |
| Insulin dependence | ||
| Yes | 40 | 45 % |
| No | 48 | 55 % |
Source: The authors.
Within the appraisal scales employed, 86 % of the participants were identified as with normal mental performance, with medium competence for self-care (63 %), followed by a low level of competence (34 %); of the 36 participating caregivers, 72 % presented medium competence. Regarding the dependence level, it was evidenced that 36 % presented slight dependence, followed by moderate level (26 %); the screening for the classification of the risk for diabetic foot revealed that 63 % were at risk 0 (no changes) and, for Wagner’s scale, 94 % of the participants did not present lesions.
Follow-up was performed once a week via phone calls during the two months proposed, with a total of 685 calls; six home visits were conducted at the patients’ request to clarify doubts regarding adequate administration of medications, healings, and use of the glucose meter. At the end of the follow-up period, the assessments were conducted, through 86 home visits and two phone assessments, as the patients were not in the metropolitan area of Cúcuta.
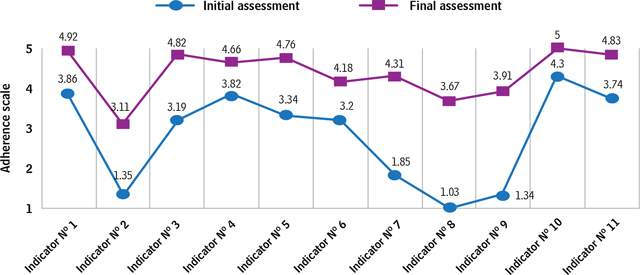
Regarding the therapeutic adherence shown by the patients, significant differences were found in all the indicators when comparing the initial assessment and the final one after the application of the preparation plan for hospital discharge employing Wilcoxon’s non-parametric test, in which a positive effect was accepted if p < 0.05. The indicators that presented the greatest positive effect were indicator 7 (monitors the changes in the disease status), indicator 8 (monitors the treatment’s secondary effects), and indicator 9 (recognizes the disease complications), with an adherence degree scale ranging from “never shown” to “frequently shown” (Figure 1).
Concerning the global score obtained in the initial and final assessments, a significant difference was obtained in the parametric Student’s t-test (0.000029) (Table 3), accepting the alternative hypothesis which set forth that the implementation of the preparation plan for hospital discharge would manage to exert a positive effect on adherence to treatment in diabetic patients.
Table 3: Statistical analysis of the general score of therapeutic adherence
| Variables | n | Mean | SD | Median | Normality as per Shapiro-Wilk | Significance as per Student’s t-test for paired samples p<0.05 |
| IA | 88 | 2.82 | 1.19 | 3 | p>0.05 | 0.000029 |
| FA | 88 | 4.38 | 0.6 | 4 | p>0.05 |
SD: Standard Deviation; IA: Initial Assessment; FA: Final Assessment.
Source: The authors.
By analyzing the effect generated by the preparation plan for hospital discharge on adherence to treatment according to gender, it was found that both men and women were categorized as with an adherence level of “frequently shown”, with scores of 4.44 ± 0.26 and 4.30 ± 0.26, respectively; as was the case in the “presence of comorbidity” and “insulin dependence” variables, in which the scores fell into the “frequently shown” scale, with their affirmative and negative answers being similar, thus determining that the presence or absence of comorbidity and insulin dependence do not exert any influence on the patients’ level of therapeutic adherence.
The diagnosis time ranges fell into “frequently shown” therapeutic adherence, headed by the group of people with 16 to 20 years of diagnosis time, with 4.45 ± 0.26 points. With the dependence level, the independent participants presented “frequently shown” adherence, followed by those with total dependence, also in the same scale. A statistically significant change validated by the parametric and non-parametric tests was found according to data distribution, except on the “high competence for self-care” variable, in which no significant change was recorded (Table 4).
Table 4. Distribution of therapeutic adherence by variables
| Variables | n | Mean | SD | Median | Normality | Significance | ||||
| Gender | Women | IA | 47 | 2.91 | 0.46 | 2.82 | SW p<0.05 | Wilcoxon p<0.05 | ||
| FA | 4.30 | 0.26 | 4.27 | SW p>0.05 | ||||||
| Men | IA | 41 | 2.71 | 0.60 | 2.82 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.44 | 0.26 | 4.45 | SW p>0.05 | ||||||
| Comorbidity | Yes | IA | 64 | 2.83 | 0.50 | 2.82 | KS p>0.05 | Wilcoxon p<0.05 | ||
| FA | 4.34 | 0.27 | 4.36 | KS p<0.05 | ||||||
| No | IA | 24 | 2.77 | 0.63 | 2.82 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.42 | 0.27 | 4.45 | SW p>0.05 | ||||||
| Insulin dependence | Yes | IA | 40 | 2.72 | 0.48 | 2.82 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 4.36 | 0.30 | 436 | SW p>0.05 | ||||||
| No | IA | 48 | 2.90 | 0.57 | 2.86 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.37 | 0.24 | 4.36 | SW p>0.05 | ||||||
| Years of diagnosis | 0-5 | IA | 22 | 2.85 | 0.54 | 2.68 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 4.38 | 0.26 | 4.31 | SW p>0.05 | ||||||
| 6-10 | IA | 28 | 2.83 | 0.56 | 2.86 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.33 | 0.31 | 4.36 | SW p>0.05 | ||||||
| 11-15 | IA | 18 | 2.78 | 0.53 | 2.73 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.32 | 0.25 | 4.31 | SW p>0.05 | ||||||
| 16-20 | IA | 12 | 2.72 | 0.53 | 2.82 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.45 | 0.26 | 4.45 | SW p>0.05 | ||||||
| 21-25 | IA | 6 | 2.81 | 0.64 | 2.91 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.37 | 0.24 | 4.36 | SW p>0.05 | ||||||
| Dependence level | Total | IA | 9 | 3.24 | 0.45 | 3.09 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 4.41 | 0.30 | 4.36 | SW p>0.05 | ||||||
| Severe | IA | 3 | 2.77 | 0.44 | 2.64 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.31 | 0.18 | 4.27 | SW p>0.05 | ||||||
| Moderate | IA | 23 | 2.67 | 0.54 | 2.73 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.33 | 0.25 | 4.36 | SW p>0.05 | ||||||
| Slight | IA | 32 | 2.74 | 0.55 | 2.73 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.38 | 0.31 | 4.45 | SW p>0.05 | ||||||
| Independence | IA | 11 | 3.04 | 0.51 | 3.18 | SW p>0.05 | Paired t p<0.05 | |||
| FA | 4.43 | 0.29 | 4.55 | SW p>0.05 | ||||||
| Competence for care | Low | IA | 28 | 2.70 | 0.55 | 2.64 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 4.34 | 0.23 | 4.36 | SW p>0.05 | ||||||
| Medium | IA | 57 | 2.84 | 0.52 | 2.82 | KS p>0.05 | Wilcoxon p<0.05 | |||
| FA | 4.37 | 0.28 | 4.36 | KS p<0.05 | ||||||
| High | IA | 3 | 3.48 | 0.28 | 3.55 | SW p>0.05 | Paired t p>0.05 | |||
| FA | 4.51 | 0.41 | 4.55 | SW p>0.05 | ||||||
SD: Standard Deviation; IA: Initial Assessment; FA: Final Assessment; SW: Shapiro-Wilk; KS: Kolmogorov-Smirnov.
Source: The authors.
In the initial assessment of the self-care agency capacity, a mean of 61.48 points was found, falling into the “low self-care agency capacity” scale; whereas in the final assessment, a mean of 80.43 points was observed, which reflects a fair self-care agency capacity; significance was verified by means of the Wilcoxon’s test, with p < 0.05 (Table 5) and accepting the alternative hypothesis in which it is stated that the effect of the plan is positive.
Table 5. Statistical analysis, self-care agency capacity
| Variables | n | Mean | SD | Median | Normality - Kolmogorov-Smirnov | Significance - Wilcoxon’s test p<0.05 |
| Initial ASA | 88 | 61.48 | 8.22 | 61 | p>0.05 | 0.00 |
| Final ASA | 88 | 80.43 | 6.04 | 81 | p<0.05 |
ASA: Appraisal of Self-care Agency; SD: Standard Deviation.
Source: The authors.
Regarding gender, it was found that both men and women were categorized as with fair self-care agency capacity in the range of its average scores; as was the case in the “insulin dependence” variable, in which the scores are similar both in the group that self-administers insulin and in the group that only takes oral medications. The patients who do not have any other disease showed greater self-care agency capacity with an approximate average value of 82 points (good), in opposition to those who do have some other disease, with 80 points (fair).
The diagnosis time ranges fell into fair self-care agency capacity, except in the patients with recent diagnoses. Regarding the dependence level, at the end of the study, the participants who were classified as with total and severe dependence showed good self-care agency with an approximate average value of 82 points, differently from the other categories, which fell into the fair scale (see Table 6).
Table 6. Distribution of the self-care agency capacity according to the variables
| Variables | n | Mean | SD | Median | Normality | Significance | |||
| Gender | Women | IA | 47 | 61.34 | 8.67 | 60 | SW p>0.05 | Paired t p<0.05 | |
| FA | 80.30 | 6.20 | 81 | SW p>0.05 | |||||
| Men | IA | 41 | 61.76 | 7.84 | 62 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 80.95 | 5.94 | 82 | SW p>0.05 | |||||
| Comorbidity | Yes | IA | 64 | 61.17 | 7.44 | 61 | KS p>0.05 | Paired t p<0.05 | |
| FA | 80.08 | 5.66 | 80.5 | KS p>0.05 | |||||
| No | IA | 24 | 62.5 | 10.22 | 61 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 82 | 6.79 | 82.5 | SW p>0.05 | |||||
| Insulin dependence | Yes | IA | 40 | 61.38 | 9.91 | 61 | SW p>0.05 | Paired t p<0.05 | |
| FA | 80.38 | 6.44 | 80 | SW p>0.05 | |||||
| No | IA | 48 | 61.67 | 6.67 | 61.5 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 80.58 | 5.66 | 82 | SW p>0.05 | |||||
| Years of diagnosis | 0-5 | IA | 22 | 62.64 | 6.60 | 66 | SW p<0.05 | Wilcoxon p<0.05 | |
| FA | 82.36 | 4.67 | 83 | SW p>0.05 | |||||
| 6-10 | IA | 28 | 61.79 | 10.9 | 62 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 79.61 | 6.13 | 80 | SW p>0.05 | |||||
| 11-15 | IA | 18 | 59.06 | 7.78 | 59 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 80.61 | 5.91 | 82.5 | SW p>0.05 | |||||
| 16-20 | IA | 12 | 60.58 | 7.48 | 60.5 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 79.5 | 7 | 79.5 | SW p>0.05 | |||||
| 21-25 | IA | 6 | 64.67 | 8.66 | 64 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 78.33 | 8.43 | 76.5 | SW p>0.05 | |||||
| Dependence level | Total | IA | 9 | 63.89 | 7.18 | 66 | SW p<0.05 | Paired t p<0.05 | |
| FA | 81.56 | 4.97 | 79 | SW p<0.05 | |||||
| Severe | IA | 3 | 59 | 7.55 | 59 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 82.15 | 5.97 | 84 | SW p>0.05 | |||||
| Moderate | IA | 23 | 59.74 | 7.60 | 61 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 78.26 | 5.21 | 78 | SW p>0.05 | |||||
| Slight | IA | 32 | 61.81 | 7.97 | 60.5 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 81.06 | 6.43 | 82 | SW p>0.05 | |||||
| Independence | IA | 11 | 65.55 | 10.98 | 68 | SW p>0.05 | Paired t p<0.05 | ||
| FA | 80.64 | 6.68 | 83 | SW p>0.05 | |||||
| Competence for care | Low | IA | 28 | 58.89 | 7.15 | 58 | SW p>0.05 | Paired t p<0.05 | |
| FA | 80.75 | 6.54 | 82 | SW p>0.05 | |||||
| Medium | IA | 57 | 62 | 7.94 | 63 | KS p>0.05 | Paired t p<0.05 | ||
| FA | 80.28 | 5.81 | 80 | KS p>0.05 | |||||
| High | IA | 3 | 77.33 | 5.13 | 76 | SW p>0.05 | Paired t p>0.05 | ||
| FA | 82 | 5.56 | 83 | SW p>0.05 | |||||
SD: Standard Deviation; IA: Initial Assessment; FA: Final Assessment; SW: Shapiro-Wilk; KS: Kolmogorov-Smirnov.
Source: The authors.
Discussion
In this study, what was stated in the situational health analysis of Colombia for 20173 is reasserted, since there was a 53 % predominance of the female gender with the disease, which coincides with previous studies12-13,20-21.
Regarding age, the relevant group was that from 61 to 70 years old, similar to another study in which the most frequent age group was from 66 to 69 years old13. Taking as a reference Dorothea Orem’s theory about self-care, it can be asserted that age is a conditioning factor that exerts a negative influence on people since the greatest incidence of the disease was recorded in the oldest participants; this leads us to think that the cause of this affectation is that, in older adults, self-care actions are influenced by the aging process that entails deviations from health22.
Regarding therapeutic adherence, it becomes relevant to contrast the indicators that obtained greater effects due to the intervention performed: monitors the changes in the disease status, monitors the treatment’s secondary effects, and recognizes the disease complications. Two of the studies found in the bibliographic review were also compared, in which the same instrument was implemented12-13.
For the “monitors the changes in the disease status” indicator, the initial assessment obtained a mean of 1.85 points (rarely shown) and, in the final assessment, the mean was 4.31 points (frequently shown), only the initial assessment in which the individuals rarely recorded their changes being similar; likewise, the “monitors the treatment’s secondary effects” indicator obtained a mean of 1.03 points in the initial assessment (never shown), equaling one of the antecedents12.
In its turn, the “recognizes the disease complications” indicator obtained an initial average of 1.34 points (never shown), a similar value to that obtained in one of the studies conducted by Universidad Industrial de Santander in which the patients did not recognize the possible disease complications; the opposite was observed for the final assessment, which obtained a mean of 3.91 points (frequently shown), differently from other studies in which the individuals did not present any increase in the ability to recognize the complications12-13.
Finally, when assessing the general score for therapeutic adherence in the assessments of this research, the initial one revealed a mean of 2.82 points, being similar to what was obtained in the study of therapeutic adherence of patients with arterial hypertension and Type 2 Diabetes Mellitus where the mean also fell into the “occasionally shown” scale12; besides, a median of 4 was obtained in the final assessment, being similar to the research on self-efficacy and therapeutic adherence in people with Type 2 Diabetes Mellitus where the median was 3.7 points13; therefore, it can be noticed that there was a significant change in the general scores, thus confirming that the preparation plan for hospital discharge implemented in diabetic patients exerted a positive effect on their therapeutic adherence.
On the other hand, the initial self-care agency capacity for this study presented a mean of 61.48 points, falling into the low agency scale and bearing some resemblance with a study conducted in the same health institution, which showed low self-care agency capacity in hypertensive patients23; in opposition, the study resulting from an educational intervention for the self-care of hospitalized patients with Type 2 Diabetes Mellitus (2016-2017) revealed an initial mean of 43.79 points, this value representing very low self-care agency capacity11,21.
According to the results obtained in the final assessment, the average score was 80.43, which falls into the fair self-care agency scale. This value bears some resemblance with the study conducted in myocardial revascularization patients in which an average of 77.07 points was obtained; it is to be emphasized that no patient fell into the very low self-care agency capacity scale, which is following this study24; also, a pilot study in patients undergoing peritoneal dialysis obtained a mean of 66.4 points, falling into the same scale, which demonstrates that the educational interventions on the patients do exert an effect on the improvement in their self-care agency capacity25.
In opposition to both assessments of this research, the study on self-care agency in patients with Type 2 Diabetes Mellitus differs from the average results, since more than 90 % of its population presented good self-care agency20.
According to the above, if the significance level between the study assessments is considered to assess the effect on the self-care agency capacity, a statistically significant difference was determined (p<0.05) employing Wilcoxon’s test, rejecting the null hypothesis and accepting the alternative one, which is under one of the studies in which this same comparison was made by applying the same non-parametric test, and a difference was found between the pre- and post-test assessments21. Likewise, it is to be mentioned that, in the Nursing educational intervention study on the self-care capacities of people with Type 2 Diabetes Mellitus by Tenosique and Tabasco, it was determined that there is indeed a positive effect on the patients after an educational intervention9 which is included within the components of the ABC for the preparation of hospital discharge in people with diabetes.
In the final score obtained about self-care agency capacity, an improvement was evidenced in the universal self-care requirements embedded in the instrument, which establishes that continuous stimulation of diabetic patients is necessary to attain an improvement in the self-care agency capacity, as set forth by Orem in one of her main assumptions, taking into account the concept of help methods of such theory26.
Among the implications inherent to the Nursing staff there must be a greater appropriation of Dorothea Orem’s theory of self-care deficit, which sets forth that the role of the professional is to encourage the patients to take the lead in their self-care, leveraging their role as educators to bridge possible knowledge gaps related to the pathology and the management of their health. Likewise, health institutions can contribute to this initiative, by adopting plans to empower users in self-care after their hospitalizations.
Conclusions
In the beginning, the participants presented “occasionally shown” therapeutic adherence, with 2.82 points; and the most relevant aspect was their lack of knowledge about their disease, as well as low self-care agency capacity: 61.48 points.
After the implementation of the preparation plan for hospital discharge, “frequently shown” therapeutic adherence was obtained, with 4.38 points and with significance according to the Student’s t-test (0.000029), p<0.05, and fair self-care agency capacity (80.43 points), with p-value < 0.05 significance according to Wilcoxon’s test, thus showing a favorable variation jointly between the measures before and after implementing the plan, both for therapeutic adherence in each of its indicators and for self-care agency capacity.
When comparing therapeutic adherence and self-care agency capacity with the gender, presence of comorbidity, insulin dependence, dependence level, diagnosis time, and competence for self-care variables, a statistically significant change was found in all, in which a p-value<0.05 is observed between the initial and final measurements.
Finally, through the statistical analysis performed, the implementation of the preparation plan for hospital discharge in people with Diabetes Mellitus had a positive effect, since the statistical p-values were < 0.05 in both variables assessed; in other words, the educational intervention was effective on therapeutic adherence and self-care agency capacity, thus reasserting the alternative hypothesis, which allows reflecting on the importance of exercising the guidance, education and patient follow-up role during their hospitalization and after discharge, being determinant in the process of adaptation to the disease, enhancing self-care and therapeutic adherence for the maintenance of health, as set forth by Orem in her theory, which reflects the evident need to conduct activities aimed at the development of these roles by the Nursing professional.
Study limitations
The sample size of the different services, for having been selected by estimating a population with this chronic disease condition possibly treated during a period in the institution.
Not implementing a control group when working with an estimated population possibly treated with this health condition.
Deterioration/Complication in the patients’ health status, or even their death.
Lack of participants’ cooperation when not informing their new street address or phone number during the follow-up process.
Lack of previous studies on the research theme or of projects aimed at the preparation for hospital discharge.
The project does not include verifying if the health institutions implemented the educational products and materials generated.

