











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Chronic kidney diseases (CKD) are quickly increasing worldwide and represent important events for public health, as a significant percentage of affected individuals progress to death. Thus, this population demands a health system organized in terms of the appropriate process and structure, so that qualified care occurs, with treatment for such diseases, according to their needs 1.
In the publication of Ordinance 389/2014, which defines the criteria for the organization of the care line of the person with CKD, replacement therapies for kidney function are peritoneal dialysis, hemodialysis and kidney transplantation, when the individual has advanced CKD 2.
Kidney transplantation is a safe and successful surgical strategy consisting of the removal of a healthy kidney from one individual (living or deceased donor) to another (recipient), to maintain lost or ineffective kidney functions. Kidney transplantation, although not the definitive "cure" for the disease, provides, among the therapeutic options, a better quality of life for chronic kidney patients 3-9.
Thus, considering kidney transplantation a substitute therapy, that is, a treatment for CKD, the kidney transplant recipient is still a person living with CKD. Thus, it is necessary to understand that, throughout its treatment, it permeates the three levels of complexity of health care: primary, secondary and tertiary, according to the organization of the care line of the person with CKD. The success of kidney transplantation is directly linked to the health and support network in which the transplanted person is inserted. Thus, during therapy, hospital admissions, high complexity procedures, follow-up of the specialized outpatient clinic and follow-up of primary care in its home location may be necessary 2,10,11.
In this perspective, because it is a highly complex treatment, kidney transplantation requires specificities from the nursing team during their care 12-14. For this, nurses must systematize their actions, their care provided and interventions with periodic evaluation of patients. Thus, the health care provided to the transplanted becomes quality and safe care, since this performance is based on scientific evidence 15,16.
In this sense, the nurse, being the leader of the nursing team, actively participates in all stages of the organ transplantation process, since his activities are broad and specialized, and the satisfactory evolution of the patient is related to the care provided to him and directly to the technical-scientific quality of the professional nurse. It has the task of coordinating the nursing service, early diagnosing problems, proposing solutions and developing health education activities in daily work focusing on technical-scientific deficiencies 17-23.
When we think of nursing care for transplanted patients, the entire postoperative period stands out until outpatient and home care for graft maintenance 24. It is emphasized that, in this process, health professionals, patients and their families are involved.
It is believed that follow-up should be performed both in primary health care (PHC) and in specialized care. However, it is perceived, in practice, that transplanted patients are followed by PHC from their municipalities in a non-effective way and that many professionals have disabilities regarding the competencies and skills in this theme.
This care, besides being important for the strengthening of PHC and being configured as an instrument that induces co-responsibility and quality to continuously improve health outcomes, is essential for the maintenance of the graft in the transplanted patient, because it allows better adhering to drug treatment as an action to protect health; promotion and prevention actions for diseases such as opportunistic infectious diseases; promotion of sexual health; health recovery actions such as reducing anxiety about doubts and treatment difficulties, and greater emotional support for the user and family involved; health rehabilitation actions 25-27.
Therefore, research on this theme is of great relevance to the health area, especially for nursing because they contribute to the quality of care provided to this patient audience, assistance that is still very specialized and little widespread in undergraduate studies. Thus, it is essential to awaken, in nursing professionals, the care of the transplanted patient at any level of complexity in health.
From the above, the study aims to map nursing care in kidney transplant patients through the scoping review.
Materials and method
A scoping review was carried out that followed the methodology recommended by the Joanna Briggs Institute 28. This methodological strategy is considered a robust approach to synthesize the relevant literature on health, being used to answer comprehensive questions and map evidence for practical decision-making and research 29.
To this end, the following steps were performed in the study: 1) elaboration of the guiding question of the scoping review; 2) identification of relevant studies; 3) sorting of studies; 4) analysis of the collected data and 5) treatment, synthesis and presentation of the results.
A protocol was elaborated for the structuring and development of the research, which contained the objective of the study, the research question, the eligibility criteria, the research strategy, the databases used for data collection, the definition of variables for data extraction and how the data would be presented. The entire protocol was based on the parameters of the participants, concept and context (PCC) strategy, in which "P" is population, "C", concept and "C", context. The scoping protocol was registered in the public domain (https://osf.io).
Thus, for the study in question, the defined population consisted of patients submitted to kidney transplantation; the concept is related to nursing care in kidney transplant recipients, and the context, to the postoperative period of kidney transplantation in hospitals and PHC. All the results found in the scoping review on the subject were included from the PCC strategy. Thus, the study has as a guiding question to identify which nursing care is described in the national and international literature to patients undergoing kidney transplantation. In addition, it has as inclusion criteria texts available in full - in Portuguese, Spanish and English - and texts that address nursing care in kidney transplant patients.
Initially, the descriptors were identified through the Descriptors in Health Sciences (DeCS) - words in Portuguese - and the Medical Subject Headings (MESH) - terms in English - which make up the mnemonic PCC of this research. They are: (P) kidney transplantation OR (C) nursing OR nursing care AND (C) postoperative period.
The second and third stage of the scoping review that corresponds to the identification and selection of studies that fall under the research occurred from December 2020 to January 2021. PubMed, Cumulative Index of Nursing and Allied Health (CINAHL), Web of Science, Latin American and Caribbean Health Sciences (LILACS) and SciELO databases were performed in the Databases. for the research of studies in the grey literature, such as theses, dissertations, manuals, protocols, guidelines and bulletins, we use the Scientific Repository of Open Access of Portugal (RCAAP), the Thesis Bank of the Coordination for the Improvement of Higher Education Personnel (Capes), to the National ETD Portal, Theses Canada, the National Health Surveillance Agency (ANVISA), the Brazilian Ministry of Health, the Federal Nursing Council, the Brazilian Organ Transplant Association and the Brazilian Society of Nephrology.
As a search strategy used for the research, we have (Kidney Transplantation) OR (Nursing OR Nursing Care) AND (Postoperative Period) for the databases in Portuguese and (Kidney transplantation) OR (Nursing OR Nursing Care) AND (Postoperative Period) for the international databases.
Scientific articles, dissertations, theses, manuals, guidelines, protocols and bulletins were defined as eligibility criteria; published and available in full online; in Portuguese, Spanish and English; and that address nursing care in kidney transplant patients. In turn, they were not included in the editorial scope and experience reports. There was no temporal delimitation in the search performed.
By evaluating the titles and abstracts of the identified studies, the preliminary selection was made. Then, the selected publications were read in full, according to Figure 1. The relevance of the articles for the review was analyzed by two independent reviewers.
The fourth stage of the scoping review aimed at the treatment, synthesis and presentation of the results was performed by collecting the data contained in the publications included in the final sample, in a spreadsheet built-in Microsoft Excel Office 365, with support for the variables listed in the research protocol: type of document, year of publication, journal, country of origin, language, study objective, type of research, study sample, main results about nursing care in kidney transplant patients identified and conclusion of the study.
After data analysis, they were synthesized and presented using tables. To facilitate the understanding and visualization of the data, the studies were coded as follows: "E" (study), followed by Arabic numerals 1, 2, 3, ... 15, to assume representation E1, E2, E3, ... E15.
The level of evidence and the level of recommendation of the studies were classified according to the proposal of the Joanna Briggs Institute 28.
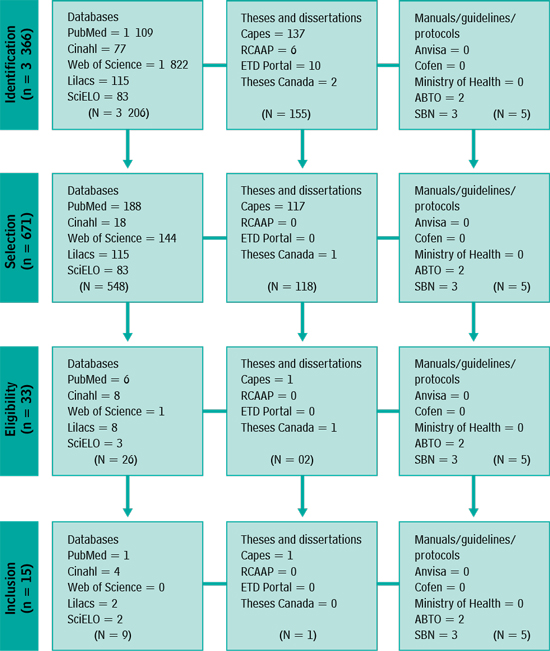
Souce: Flowchart for the scoping review (adapted from Prisma)
Figure 1 Scheme of the study selection process.Natal, Brazil, 2021.
To facilitate the reader's understanding and through the materials selected in the scoping review, nursing care for kidney transplant patients was classified as: nursing care to kidney transplant recipients in the immediate, middle, and late postoperative periods, and nursing care for kidney transplant recipients in PHC.
Results
The final sample of the scoping review consisted of 15 publications (100%). Among these, there are articles (60 %), manuals (6.6 %), dissertations (6.6 %), protocols (6.6 %), guidelines (13.6 %) and bulletins (6.6 %). Most publications have a quantitative approach (86.6 %); on methodological design, 60% of the studies are descriptive, 13.3 %, transversal character, 6.6 %, observational and 20.1 %, others.
As for the country of origin, 93.3 % of the material comes from Brazilian studies. In view of the sample found, the publications started in 2006 and ended in 2021. Most publications were in 2006, followed by 2007, 2013 and 2016, each year with two publications on the subject, according to Table 1.
Table 1 Characterization of the included studies. Natal, Rio Grande do Norte, Brazil, 2021.
| Study code (reference) | Study aim | Country (year) | Type of study/ approach/type of publication/level of evidence |
|---|---|---|---|
| E1 | Have evidence-based recommendations on Covid-19 vaccination for kidney transplant recipients. | Brazil (2021) | Descriptive/qualitative/ Bulletin/5a |
| E2 | Evaluate the knowledge of nurses in patient care in the immediate postoperative period of kidney transplantation. | Brazil (2020) | Exploratory, descriptive/ qualitative/article/4b |
| E3 | To know the complications that led patients to re-intern in the first year after kidney transplantation and develop strategies to reduce them. | Brazil (2018) | Retrospective/ quantitative/dissertation |
| E4 | Identify the care performed by people with kidney transplantation for the maintenance of the transplanted organ. | Brazil (2017) | Descriptive/qualitative/ article/4b |
| E5 | To recognize the facilities and difficulties that people with CKD experience after kidney transplantation. | Brazil (2016) | Descriptive/qualitative/ article/4b |
| E6 | To analyze the perceptions of transplant patients and health professionals about kidney transplantation. | Brazil (2016) | Exploratory, descriptive/ qualitative/article/4b |
| E7 | Review sorting parameters, prevention and management strategies for diabetes mellitusbefore and after transplantation. | Brazil (2014) | Descriptive/bibliographic review/article/4a |
| E8 | To analyze the quality of life of people with chronic kidney failure undergoing hemodialysis compared to transplant patients. | Brazil (2013) | Descriptive, cross/ quantitative/article/4b |
| E9 | Clarify the basic doubts that occur in the period after kidney transplantation. | Brazil (2013) | Descriptive/qualitative/ manual/5a |
| E10 | Conduct a bibliographic survey about the role of care and educator of nurses in kidney transplantation. | Brazil (2012) | Descriptive, retrospective/ bibliographic review/ article/4a |
| E11 | Systematize the actions and planning of care provided to patients submitted to kidney transplantation by the nurse professional. | Brazil (2008) | Descriptive/qualitative/ protocol/5a |
| E12 | To identify nursing diagnoses in the immediate postoperative period of patients undergoing kidney transplantation and to raise nursing actions proposed by the Nursing Interventions Classification for nursing diagnoses identified in patients undergoing kidney transplantation. | Brazil (2007) | Descriptive, transversal character/qualitative/ article/4b |
| E13 | Identify nursing care recorded in the medical records of clients in the postoperative period of kidney transplantation; discuss the implications of records for nursing care; evaluate nursing care. | Brazil (2007) | Descriptive/ observational study/ article/4b |
| E14 | To present recommendations for the practice of kidney transplantation, based on evidence published in the literature and clinical experience. | Brazil (2006) | Descriptive/qualitative/ guideline/5a |
| E15 | To present recommendations for the practice of kidney transplantation, based on evidence published in the literature and clinical experience. | Brazil (2006) | Descriptive/qualitative/ guideline/5a |
Source: Own elaboration.
Table 2 gathers the main findings, classifying them in nursing care after kidney transplantation (immediate, mediated and late) and PHC.
Table 2 Main nursing care in kidney transplant patients mapped in the scoping review. Natal, Rio Grande do Norte, Brazil, 2021.
| Classification of post-kidney transplant nursing care | Main results |
|---|---|
| Immediate post-operative nursing care | • Carrying out the systematization of nursing care 30. • Maintaining bed rest for the first 24 hours and guiding the patient not to exert physical effort 1-5,15,22,23,27-32. • Clinical evaluation of the sign and symptoms of sudden anuria, for the prevention of kidney artery thrombosis 29-31. • Monitoring the level of consciousness and cough reflex 30,33. • Monitoring of systemic signs and symptoms and sites of infection such as the surgical wound 15,32,34. • Carrying out medication handling 15,33. • Control of hemodynamic status, blood pressure, respiratory function and capillary blood glucose levels 31,33,35-37. • Monitoring the hydration situation, performing volume replacement, controlling diuresis every hour, weighing in fasting, assessing waist circumference and laboratory results regarding fluid retention 4,15,30,36,38-40. • Care with an indwelling urinary catheter for the prevention of urinary tract infections 15,33. • Care with surgical drains 15,33,36. • Administration of a light diet after 8 to 12 hours of fasting if clinical conditions exist 15. • Limiting the number of visits 15,30,33. |
| Immediate post-operative nursing care | • Carrying out the systematization of nursing care 30. • Monitoring of systemic signs and symptoms and sites of infection such as the surgical wound 15,30,31,34. • Carrying out medication administration 15,33. • Control of hemodynamic status, blood pressure, respiratory function and capillary blood glucose levels. • Continuous monitoring of vital signs, patient weight in fasting 4,15,16,30,38-40). • Recording and evaluation of diet acceptance; maintenance of care with indwelling bladder catheter, with the removal of the bladder catheter on the 4th postoperative day 1,3. • Monitoring the hydration situation; performing volume replacement; diuresis control every hour; weighs in fasting; evaluation of waist circumference and laboratory results regarding fluid retention 1,30,31,34. • Beginning of guidance on adherence to treatment/follow-up and information on side effects resulting from immunosuppressive agents or rejection 15,36,38. • Exercise of the caregiving and educator role 36. • Early detection of complications related to the surgical procedure 33,36,37,39. • Assessment of the presence of hemorrhage, hematomas in the surgical wound and dressing changes 31,33,38. • Encouragement to walk as early as possible 33. |
| Late postoperative nursing care | • Prevention of surgical wound infection and urinary infection, in addition to the removal of surgical stitches 30,31,40. • Offering recommendations on the correct use of immunosuppressants and other necessary medications 15,36,38. • Guidance on the importance of attending scheduled outpatient appointments; exams scheduled weekly during the first 30 days; monitoring of vital signs, capillary blood glucose; dietary recommendations; regular physical activity; obesity prevention; avoidance of alcohol and tobacco 15,31,37. • Exercise of the caregiving and educator role 36. • Advice on staying away from people with contagious diseases or animals and frequent hand washing 40. • Avoidance of lifting heavy objects, pulling or pushing large objects, because between the 6th and 8th week, the surgical wound must heal completely 15,30. • Clinical evaluation of the emergence of lymphoceles; evaluation for the presence of a palpable mass, hydronephrosis and edema of the lower limb on the transplant side 38. |
| Nursing care for kidney transplant recipients in PHC | • Regular maintenance of follow-up with consultations by the multidisciplinary team 36,40. • Exercise of the caregiving and educator role 36. • Encouragement of scheduled exams; monitoring of vital signs; regular physical activity; obesity prevention 36,40,41. • Encouraging healthy habits, such as eating less sodium and protein, with lots of fiber and fluid intake 27. • Guidance on avoiding alcohol and smoking, as well as hygiene care and infection control 40. • Guidance on medication care and the importance of adherence to the use of medications, especially immunosuppressants 31,36,37,39,40. • Guidance on returning to sexual activity and family planning 4,16. • Avoidance of abdominal exertion and exercises in the first months after surgery 39. • Guidance on the use of sunscreen and avoiding the sun 16,35. • Monitoring the patient from the beginning of the evolution of their disease to a better quality of life after the procedure 16,33,34,37. • Orientation of the patient to always walk with their identification card about their transplant condition, in addition to their medication 15,32,34,36. • Updated vaccination card - including Covid-19 vaccination 41. • Evaluation of signs and symptoms suggestive of cytomegalovirus infection, especially in the first three months 37. • Evaluation of signs and symptoms of chronic rejection (progressive worsening of kidney function, presence of proteinuria, less than 1.0 g/day in 50% of cases), presence of arterial hypertension (> 90%)15,34-36). |
Source: Own elaboration.
Among nursing care after kidney transplantation (immediate, mediated, late), the material studied has as main findings to control hemodynamic status, blood pressure, respiratory function and capillary glucose levels; monitor the hydration situation; perform volume replacement, diuresis control every hour; fasting weigh; evaluate abdominal circumference and laboratory results related to fluid retention; monitor systemic signs and symptoms and sites of infection such as the surgical wound; care with an indwelling urinary catheter for the prevention of urinary tract infections; detect early complications related to the surgical procedure; initiate guidance on treatment/follow-up and inform about side effects resulting from immunosuppressive agents or rejection (Table 2).
On the extra-hospital care that also involves PHC, it was identified to encourage healthy habits, such as feeding with less sodium and proteins, with many fibers and fluid intake; guide to avoiding alcohol and smoking, in addition to hygiene care and infection control; guide care with medications and the importance of adhering to the use of medications, especially immunosuppressants; check the vaccine card and guide the one that is up to date; evaluate signs and symptoms suggestive of cytomegalovirus infection, especially in the first three months; evaluate signs and symptoms of chronic rejection (progressive worsening of kidney function, presence of proteinuria, less than 1.0 g/day in 50% of cases); the presence of hypertension (> 90°%), as observed in Table 2.
Discussion
Given the predominance of descriptive studies developed in Brazil, in the final sample of the scoping review, it is evident the need for studies related to this theme focused on clinical practice and with scientific productions with a better level of evidence, making reliable publications that empower the care nurse and assist him in decision making.
Nursing care for kidney transplant patients is essential for the maintenance and preservation of the graft and quality of life of the patient. This care constitutes the basic structure for the patient in the post-transplant period because nursing is the category that is present 24 hours next to the patient during hospitalization and that also monitors and monitors the responses of the organism along with the three levels of health complexity 40.
Research developed on the culture of patient safety in kidney transplantation showed the need for continuous improvement of the nursing professional in the face of theoretical and practical knowledge related to transplantation. It is noteworthy that the nursing professional must be trained and have the skills and competence to assist the transplanted patient to enable safe care for patients and staff, a better quality of care provided, a higher graft survival and better quality of life for kidney transplant recipients 42.
Considering the classification used in the review of the scope in question for nursing care for kidney transplant recipients in the immediate, middle and late postoperative periods, and nursing care for kidney transplant recipients in PHC, results were found for each classification.
For this, nursing care in the immediate postoperative period is vital, being considered a care for critical care. In the first 24 hours after kidney transplantation, nursing actions aim to prevent complications and prioritize the continuous evaluation of general health status with noninvasive monitoring of vital signs and evaluation of the nursing team of 1 hour/1 hour in the first 12 postoperative hours, which allows early and appropriate interventions for each type of worsening. This period of great potential for hemodynamic instability, cardiovascular and neurological complications, important metabolic alterations and the need for replacement of parenteral fluids in large volumes that require intensive care for the maintenance of life 5,23,43,44-49.
The main complications of this period are related to the surgical procedure of kidney transplantation, such as: kidney artery thrombosis, hemorrhage, kidney surgery, urinary obstruction; and non-surgical complications such as acute graft rejection 37,41. Therefore, the care of the nursing team should be based on clinical evaluation based on physical examination and laboratory tests for monitoring kidney function, pulmonary and cardiovascular function, with emphasis on monitoring the hydroelectrolytic balance and signs and symptoms of kidney injury 5,23,33,50.
Nursing care in the middle postoperative period is a continuity of the surveillance of these patients. The main complications in this period are kidney vein thrombosis, bladder fistula, urinary fistula, kidney shop hematoma, urinary infection and hypertension.
The emphasis of care in this period is the monitoring of the hydro-electrolytic balance, care for infection prevention, pain control, maintenance and stimulation of pulmonary function, early ambulation, restoration of gastrointestinal functions and restoration of kidney function 37,51-53.
In this moment of care still in the hospital environment, it is extremely important to create the bond between professionals and the patient, because the longevity of the graft, the quality of life of the recipient and self-care are associated with his/her treatment' and the latter, directly linked to the relationships established throughout the health network. Thus, the professional must establish a dialogical relationship with the client, with a clear language, holistic treatment, individualized, considering their socioeconomic, cultural, religious and cognitive condition 37,41,53-58.
How far from the surgical procedure, surgical complications are more difficult to happen, but they may still be present, coming to light, more predominantly, clinical complications 59. Thus, we can say that, in the late postoperative period, the most common complications are lymphocele, urinary infection, cytomegalovirus infection, systemic arterial hypertension, diabetes mellitus, rejection of the acute or chronic graft 32,37,41,60-65.
However, late nursing care is based on the care of the surgical wound, the scores of laboratory results of the general state of health and kidney function, but the care of guidance to the recipient and family members regarding the use of immunosuppressants, the importance of returning to consultations and the performance of scheduled tests, maintenance of dietary recommendations and physical activity, among others 15,32.
This study highlights the inclusion of nursing care for kidney transplant recipients in PHC. As important as the follow-up of kidney transplant recipients in secondary care, that is, in the specialized outpatient clinic, it is the follow-up of it in PHC in the basic units and in the family health strategy in the municipalities of origin.
It is important to highlight that the kidney transplant patient is still a patient with CKD and should be inserted in the health care network at the three levels of complexity, according to their need.
Published in March 2014, Ordinance 389 defines the criteria for the organization of the care line of the person with CKD. Thus, it is the responsibility of PHC to perform educational activities and support self-care, expanding the autonomy of the person with CKD, such as stimulating and guiding therapeutic adherence, updating the vaccination card, personal and home hygiene care, and care for the prevention of opportunistic infections due to immunosuppression 2.
It is the responsibility of specialized outpatient care to maintain communication with the multidisciplinary teams of the other components of the Health Care Network 2. This shows that networking among the levels of complexity of care for patients with CKD is extremely important.
Moreover, the potential of studies of this nature is considered by synthesizing and mapping knowledge that ensures a care practice based on scientific evidence and allows decision-making. Added to this theme and the evidence summed up for nursing professionals working with kidney transplant patients in a perspective of guidance and support to safe nursing care practices.
The heterogeneity of the selected studies and even the possibility of vice-studies in individual studies described are uncontrolled characteristics in this type of study and is considered as a limitation of the research. Another limiting feature would be the non-inclusion of material published and available in full in a non-free online medium that could add scientific value to this scoping review. The scarcity of studies focused on nursing care in the international literature was listed as a complicating feature, but not controlled in this type of study.
Conclusion
It was concluded that the study allowed mapping nursing care to kidney transplant patients in the immediate, immediate, late and PHC postoperative periods.
The mapping of nursing care to kidney transplant recipients provides the strengthening of the care offered in the health care network and is configured as an instrument that induces co-responsibility and quality intending to continuously improve health outcomes. An important driver for the praxis (action-reflection-action) of science and for the valorization of nursing.
Given the complexity that the patient submitted to kidney transplantation presents, it is necessary that the nurse who assists this public be trained to conduct care efficiently in the face of the complex situations resulting from the clinical profile of patients, developing their practice of competent care for safe decision-making, ensuring patient safety and based on scientific evidence.
The insertion of primary health care in the care of kidney transplant patients becomes a differential of this study. In addition, this care is considered essential in the process for graft maintenance in transplanted patients, as it allows better treatment support, promotion and prevention of diseases such as opportunistic infectious diseases, reduction of anxiety regarding doubts and difficulties of treatment and greater emotional support for the user and the family.

