











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Prenatal care is, globally, one of the priority programs offered within the scope of primary health care. In line with the recommendations of the World Health Organization, the primary objective of prenatal care is to identify possible pathologies, anomalies, or congenital- fetal complications at an early stage 1,2.
Quality prenatal care involves a comprehensive set of procedures and guidelines for pregnant women, provided within the scope of primary health care 3. In Brazil, around 90 % of pregnant women receive prenatal care. However, the quality of this care is a critical issue and increasingly requires interprofessional strategies to understand it in a broader and more contextualized way 4.
The national survey conducted between 2011 and 2012 showed that although Brazil had made significant progress in prenatal coverage (98.7 %), only 73.1 % of pregnant women had the minimum number of six appointments recommended by the Ministry of Health 5,6. Another study shows that discontinuity of prenatal care, especially in rural areas, is the main factor impacting both access to and the quality of prenatal and postnatal care 7.
Countries, in general, have demonstrated important initiatives related to improving the pregnancy-puerperium cycle. Studies show that sustainable development goals, especially those related to reducing maternal, neonatal, and infant mortality, can be achieved through collegiate and intersectoral efforts between the various actors and services 8-11.
Although there are initiatives and efforts to expand coverage and improve care for pregnant women in primary health care, maternal and child health continues to be an important subject of investigation. Investing in management and the prenatal qualification network, based on constructivist and interprofessional approaches, has repercussions in terms of expanding professional knowledge and favorable outcomes in labor and birth, including a reduction in maternal and neonatal morbidity and mortality 12-14.
Thus, to contribute to the qualification of prenatal care and the achievement of sustainable development goals, the following research question was posed: How can prenatal care and management be qualified from an interprofessional perspective? This study aimed to describe interprofessional prenatal care and management strategies in the context of primary health care.
Materials and Methods
This is a qualitative, exploratory, and descriptive study performed between August and December 2022. This approach was chosen because of the possibility of constructing meanings that favor reaching perceptions, perspectives, and experiences that cannot be reduced to specific, linear variables. The consolidation criteria for qualitative research reports were considered throughout the process (Coreq [15]).
The data was collected using an instrument to analyze the content of infographics produced by 26 health professionals from the south of Brazil, as an evaluation activity for a 40-hour prenatal qualification course. The infographics were developed by the interprofessional teams of the primary care center (around seven members in each team) and posted on the virtual learning environment (VLE) by one of the 26 professionals included in this study.
The professionals responsible for posting the infographics on the VLE had previously taken part in a prenatal qualification course, in person and synchronously, run by two professors from a higher education institution in southern Brazil, in partnership with the local municipal health department. The lecturers responsible for running the prenatal course already had expertise in running courses in this same modality and were widely involved in local health services through teaching and research activities.
The topics covered in the prenatal course and discussed by experts in the field were prenatal care from an interprofessional perspective; birth planning; empowerment for childbirth; infectious diseases during pregnancy; gestational and fetal anomalies; breastfeeding; partner prenatal care, and others.
Among the 26 professionals who composed the corpus of this study were nurses, doctors, dentists, psychologists, and nursing technicians who work in primary health care, more specifically in basic units that are part of the Unified Health System (SUS), and who provide prenatal care. The inclusion criteria were health professionals who had demonstrated 100% attendance at all the prenatal course activities. And, as an exclusion criterion, professionals who had not posted the evaluation activity on the VLE within the stipulated timeframe.
The data was collected, more precisely, by analyzing the content of the infographics posted on the VLE of the institution of origin of the two dynamic teachers of the prenatal course. Participants were encouraged to develop the infographics with their colleagues to broaden their perspectives on management and prenatal care. They were provided with an infographic template and a guiding question for creating the infographic: What management and care strategies do you consider to be relevant to improving prenatal care in your health unit?
The content of the 26 infographics included in this study was analyzed using the thematic content analysis technique proposed by Minayo 16, systematized in three phases: 1st pre-analysis phase—detailed reading and analysis of the content of all the infographics, review of the hypotheses and proposed objectives to guide the in-depth analysis of the data; 2nd material exploration phase—systematic and critical analysis of the content of the infographics to generate initial thematic categories; 3rd data treatment phase - inference, interpretation and final delimitation of the thematic categories. The data analysis phase was conducted by the researchers and then validated by the study participants.
To comply with ethical issues, the recommendations of Resolution 466/2012 of the Brazilian National Health Council were complied with. To maintain anonymity, the participants’ statements were identified only by the letter “P” (participant), followed by an Arabic numeral: P1... P26. The participants were contacted by the researchers (principal investigators) who ran the prenatal qualification course. Before signing the informed consent form, they were informed of the objectives, the methodology used, their right to free access to data and to withdraw from the study at any time. Thus, their informed consent to the research was given in writing, voluntarily and autonomously, using the aforementioned form. The project was approved by the Franciscan University’s research ethics committee under No. 5.183.232 and was granted ethics approval certificate No. 54380521.2.0000.5306.
Results
Of the 26 professionals who posted infographics on the VLE, 13 were nurses; 5 were doctors; 3 were dentists; 3 were psychologists, and 2 were nursing technicians. All of them work in primary care centers in the south of Brazil, have been working in the area for more than two years, and are on average 42 years old.
As for the infographics, a representative figure of those posted on the VLE is presented for illustration purposes.
The data analyzed made it possible to define three thematic categories: “The necessary intersectoral and interprofessional coordination;” “Responsibilities built and shared between pregnant women and professionals,” and “Planning and qualification of workflows and processes.”
The Necessary Intersectoral and Interprofessional Coordination
In their presentations, the participants mentioned the need to evolve and gradually look towards more participatory, dialogical, and interactive prenatal care and management processes, with the inclusion of various health actors. The professionals generally acknowledged that health processes are still fragmented, disciplinary and sectorized. They showed that one professional often does not know and value what the other is doing and, likewise, one team/ sector does not value the initiatives of the other sectors. From this point of view, they demonstrate the following strategies:
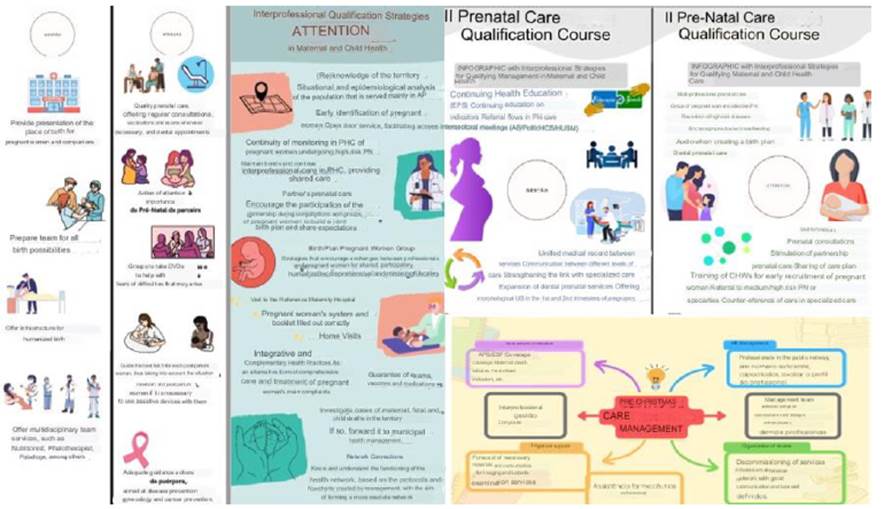
Source: Compiled from the infographics posted on the VLE
Figure 1 Infographic Showcasing Strategies to Improve Prenatal Care and Management
Carrying out promotion and prevention actions involving other sectors of the public administration. [P3]
Inclusion of different subjects in the analysis and decision-making processes, in the expansion of policy in general and health in particular, in a place of formulation and agreement on tasks and collective learning. [P6]
In health care, we must all look at the mother, baby, family and community and remember that Brazil’s Unified Health System is about co-management and comprehensiveness. [P12]
Intersectoral coordination, embodied in the decentralization of decisions and effective communication between the different health professionals, services and sectors, is an important proactive strategy to guarantee the quality and effectiveness of quality prenatal care, thus contributing to favorable outcomes in childbirth and the postpartum period. This qualification can be achieved through:
Decentralizing decisions and bringing management, staff and users closer together. [P11]
Creating a WhatsApp group made up of pregnant and postpartum women in the area, professionals and managers as a quick and effective participatory management tool. [P13]
Decentralizing prenatal care by setting up multi-professional teams in Primary Health Care. [P21]
According to the participants, prenatal care is still centered on a specific professional, in this case usually the doctor or nurse. All of them recognized the importance of interprofessional work in health, but few knew how to conduct this dialogue between professionals, services and sectors. The participants indicated that in prenatal care, dentists, psychologists, physiotherapists, nutritionists and other professionals also play an important role in providing comprehensive care to pregnant and postpartum women.
Promoting actions that involve all health professionals and not just nurses and doctors. [P9]
Prenatal consultations interspersed between all professionals. Counter-referral to specialized care. [P18]
Development of an integrated information system between all points in the network. [P22]
Strengthen the referral and counter-referral instrument with maternity wards/ambulatories and postpartum communication. [P15]
In addition to the disciplinary nature of prenatal care, several participants mentioned the work overload resulting from the lack of other professional areas. In one speech, the professional pointed out that she needed to attend to eight pregnant women in her shift to cope with the 60 pregnant women in her area. In addition, she recognized that she was unable to provide quality prenatal care or even create a bond with pregnant women, which is considered an essential strategy for effective care and achieving the proposed objectives.
Responsibilities Built and Shared between Pregnant Women and Professionals
The participants generally recognized that the quality of prenatal care and management is the result of a set of actions shared between pregnant women, health professionals, and managers. At the same time, they signaled that pregnant women need to be encouraged to play a leading role in the pregnancy-puerperium journey.
Providing qualified care so that pregnant and postpartum women can have more autonomy and actively participate in the whole process. [P12]
Joint and collaborative care between pregnant women and professionals at all stages. We need to encourage and respect the autonomy of pregnant women as a quality criterion and not consider the decisions of professionals alone. [P25]
The participants highlighted the importance of continuing health education as a tool for inducing new knowledge and practices. They also mentioned the importance of integration processes between educational institutions and health services, to promote feedback between theory and practice.
Permanent education is the key. The healthcare network always needs to be nourished by shared knowledge. [P3]
Provide technical and pedagogical support for health teams. [P5]
Hold weekly team meetings to discuss cases and the demands of professionals to achieve comprehensive prenatal care. [P16]
Qualify training in undergraduate and residency courses, especially for those who do internships in management and who are involved in maternal and child care. [P26]
Some professionals stressed the importance of pregnant women’s groups, based on systematized meetings and with the participation of the companion. They acknowledged that the units need to ensure an environment that aggregates and enhances dialogic processes so that professionals and pregnant women feel welcomed and motivated to build new knowledge and practices.
Strengthen the pregnant women’s group with the participation of partners and family members. [P7]
Pregnancy groups with the support of the interprofessional team and strengthening links with universities. [P9]
Qualify the spaces, the reception and ensure an adequate environment for health professionals and users. [P23]
The bond between professionals and pregnant women is established through dialogic movements and shared spaces for building knowledge. However, this bond is hampered by the high turnover of professionals in primary care centers.
We advocate welcoming women with active listening, health education, screening pregnant women, the participation of the accompanying person and the creation of a professional-user bond. [P24]
Along the same lines, continuing health education processes should strengthen and expand teamwork and encourage inter- professionalism. Most of the professionals recognized that the quality and effectiveness of prenatal care are the result of joint efforts between all the players in the health sector.
Agreements with educational institutions to promote continuing education. [P2]
We need to guarantee prenatal consultations with alternating medical and nursing professionals. Extend assistance to other professional categories such as dentistry, social work, nutrition, physiotherapy to expand care. [P17]
We need to set up oral health teams in all the health units that don’t have a dental service. [P23]
The results show that professionals want to evolve in the shared construction of knowledge and responsibilities between the various health actors. On this path, welcoming, an aggregating environment, active listening, early access to appointments and the professional-user bond are strategies that should be considered and encouraged.
Planning and Qualification of Workflows and Processes
Participants showed a growing desire to improve workflows and work processes through systematic planning and evaluation of prenatal care and management in the context of primary health care.
Qualification of flows between sectors. [P1]
Flowchart for the early collection of pregnant women in Primary Health Care. [P7]
Organize the presentation of the place of delivery for pregnant women and their companions. [P9]
Better organize appointments, monitoring of vaccinations and tests and dental appointments. [P12]
Plan guidance during home visits and guidance in schools to clarify doubts. [P18]
The professionals also demonstrated the importance of planning health actions, based on prospective goals that include everything from educational and family planning activities to functional and structural conditions, as well as the appropriate sizing of human resources.
Planning of care actions for the newborn, puerperal women and their families, definition of educational actions and goals and the correct allocation of human resources within primary care and the health sector, technological, financial and infrastructure resources, among others, in order to achieve the objectives. [P7]
Family planning actions: anti/pre/post-conception. [P18]
We need planning with all the health professionals. [P23]
Planning was mentioned as a quality strategy. The professionals recognized that decisions regarding normal childbirth require planning actions that need to be considered by pregnant women and families throughout prenatal care.
Plan guidance for pregnant women on the benefits of normal childbirth. [P1]
The birth plan needs to be discussed between professionals and pregnant women/ families in order to reduce the number of cesarean sections by providing information during consultations and health groups. [P6]
In order to carry out the planning and organizing functions, we need to develop aspects of leadership in order to make actions dynamic and continually evaluate them. [P22]
Planning was also considered for programs to prevent and manage gestational diseases, such as congenital syphilis and others. From this perspective, the professionals pointed out that all actions need to be planned and continually evaluated to monitor improvements along the way.
Planning promotion and prevention actions involving other sectors of the public administration. [P14]
Permanent education for the multi-professional team on the clinical management and prevention of congenital syphilis. [P24]
The planning and qualification of workflows and work processes, in the view of professionals, is imperative for achieving better results in maternal and child health. However, this path must not lead to a lockdown of the work process or reduce it to rules and routines. Planning, as a management tool, should guide decision-making and define objectives for achieving agreed goals.
Discussion
Among the wide range of aspects related to the qualification of prenatal care and management mentioned by professionals, some deserve to be highlighted in this discussion. This requires a framework capable of broadening the discussion and enabling forward- looking strategies that induce better practices. The framework that best meets these expectations is complexity thinking.
The first aspect refers to the fact that the infographic was built collegially by the various members of the health team. This dialogic and collaborative process of construction sparked the need to review internal protocols and flowcharts, as well as the desire for change among professionals. Therefore, this approach to building knowledge should be considered promising in inducing new knowledge and practices in health.
The collaborative construction of the infographic, from the perspective of interprofessional management and care, led to the need to conceive the whole in the parts, as well as the parts in the dynamics of the whole. This provocation was expressed to the extent that the professionals recognized that the work process needs to be networked and shared between the different professionals, sectors, and services. The participants were challenged to perceive health demands beyond their field of vision and to scrutinize the manager’s challenges in promoting interconnectivity in health.
To bring together and integrate separate pieces of knowledge, complexity thinking recognizes that it is necessary to conceive of the part to understand the whole, as well as to encompass the whole to know the part, i.e., each point/node in the health network or system. Under this impetus, studies show that complexity thinking induces advances in the field of knowledge, in other words, a new conception of knowledge itself that puts an end to the specialization, simplification and fragmentation of knowledge and practices 17-20.
New approaches are therefore required in the training process for health professionals, capable of transcending traditional methodologies centered on the accumulation of specific and disciplinary information. Achieving complex thinking —expanded and interprofessional— requires the construction of dispersed and random knowledge to form an integrated whole. For the author of complex thinking, information is not knowledge. Knowledge is associated with the organization of information 21. But how can we create and promote knowledge in which the user/pregnant woman is the protagonist in strategic decision-making?
The professionals in this study, albeit in an incipient way, showed the need to achieve a new way of thinking about health. Studies corroborate this thinking by demonstrating the relevance of intuiting expanded and interprofessional approaches, capable of integrating, dialoguing and building knowledge and practices in a horizontal, collaborative and systemic way 22-25.
Another element that was strongly discussed in the prenatal qualification course and which was evident in the content of various infographics is related to the planning of health actions. It was noted that, in many services, care for pregnant women is carried out in a punctual, linear and verticalized way, i.e., there is no planning with procedural evaluation of health actions. This aspect particularly concerns health managers who base their management on traditional vertical models. In this sense, the question arises as to who are the professionals that occupy health management positions and how to qualify the management process in the light of complexity thinking.
It can therefore be seen that most of the weaknesses pointed out by professionals can be overcome with simple, low-cost measures. Most of the time, the origin of these problems lies in the inability to listen to and dialog with the various actors in the network. Sometimes, the attitude of the “manager-in-chief” paralyzes work processes and makes it impossible for all the actors in the health network, including pregnant women and their companions, to participate prospectively.
From the perspective of complex thinking, the management process is woven simultaneously with circularity, complementarity, interdependence and interactivity. The manager-leader, unlike the manager-in-chief, can promote mechanisms of inclusion and participation, in which the different players are protagonists in the construction of new and more advanced health knowledge. The gesture-leader is thus represented collectively and collaboratively in the situation and as a consequence of the relationships and interactions of its actors. It develops from the notion of the whole and the part, both in mutual interaction, whose success is deliberated by the quality of the interactions 26-28.
Qualifying maternal and child health based on the results achieved implies supplanting traditional management and care models, and especially qualifying health work processes based on dialogic and collaborative approaches. Studies reinforce this argument by emphasizing that cooperation between health professionals is essential for fostering best practices in maternal and child health 29,30. Instead of unilateral and predictable processes, the process of prenatal management and care needs to lead to circular and complementary paths, from the perspective of interprofessionality.
Conclusion
Interprofessional prenatal care and management strategies in the context of primary health care are associated with overcoming fragmented and dichotomous approaches, as well as the prospect of more participatory, dialogic and interactive prenatal care and management processes, with the inclusion of various health actors.
Just as other studies have shown the need to advance approaches that broaden and contextualize prenatal care, in this study the participants suggested the inclusion of new players in the work teams to strengthen interprofessional strategies. Although in an incipient and superficial way, the professionals recognize the need to evolve and achieve a new way of thinking about health, i.e., an expanded way of thinking, capable of integrating, aggregating and enhancing collaborative initiatives and processes.

