











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
A spinal cord injury is an event that generates significant negative repercussions on the well-being and quality of life 1,2 of those who suffer from it. Its etiology is mainly traumatic in origin 3 and results in partial or complete loss of motor, sensory, and autonomic innervation below the lesion level 4. People with spinal cord injury are at high risk of developing other conditions that can be life-threatening, such as neurogenic shock 5,6, respiratory failure 5,6, pneumonia 5,6, deep vein thrombosis 5,6, pulmonary thromboembolism 5,6, urinary tract infections 5,6, and autonomic dysreflexia 6,7.
Autonomic dysreflexia (AD) manifests as the loss of coordinated autonomic responses and cardiovascular control 8. It commonly occurs after the fourth week after the injury 9. Its prevalence ranges from 48% to 90% in people with complete and incomplete spinal cord injuries 10. Physiologically, it is caused by a massive sympathetic discharge triggered by noxious visceral or somatic stimuli originating below the level of the lesion 11.
In 1988, the North American Nursing Diagnosis Association (NANDA) approved the AD as a nursing diagnosis 12. It belongs to domain 9: coping and stress tolerance, class 3: neurobehavioral stress/ behavioral responses that reflect brain nerve function. NANDA-I defines this diagnosis as the life-threatening, uninhibited sympathetic response of the nervous system to a noxious stimulus after a spinal cord injury at the seventh thoracic vertebra (T7) or above 12. In the 2021-2023 version of NANDA-I, this diagnosis comprises 16 defining characteristics and 26 related factors grouped into six categories: gastrointestinal stimuli, musculoskeletal-neurological stimuli, regulatory and situational stimuli, reproductive-urological stimuli, and others 12. It has five risk population groups and 13 associated problems 12.
A nursing diagnosis must be comprehensive and sufficient in all its elements to support care in daily practice. In clinical practice, the identification of AD is essential for its timely intervention and the anticipation or prevention of even more severe events such as acute myocardial infarction 13, cerebrovascular disease 14, and even death 14,15. Therefore, nurses must have this diagnosis, whose components are specific and coherent, so they can accurately interpret the human responses of the person with spinal cord injury. Disciplinary knowledge constantly evolves with nursing practice, and as research clarifies that knowledge, it is crucial that the NANDA-I terminology be strengthened and updated with these changes 12.
Nursing diagnoses delineate complex phenomena that can be better understood in the light of situation-specific theory. In that sense, developing a situation-specific theory allows for progress in the review and validation process. A situation-specific theory is defined as a set of concepts and statements about the concepts that address a specific population and a specific health condition 16.
The statements about the concepts include their theoretical and operational definitions and the links between them. These theories can provide a basis for developing the knowledge of the discipline, explaining and expanding specific phenomena related to the nursing practice 16, as is the case of nursing diagnosis. However, no situation-specific theory was found in the scientific literature that describes or explains the nursing diagnosis of AD in adults with spinal cord injuries using a nursing theory as a reference. Due to the above, the objective of this study was to construct a situation-specific theory for the nursing diagnosis of AD derived from the adaptation model of Sor Callista Roy.
Methods
This theoretical study followed the five stages de Oliveira Lopes et al. 17 proposed for developing middle-range theory. These were defining the approach to construct the theory, defining key concepts, developing a pictorial diagram, building propositions, and establishing causal relationships and evidence for practice.
Definition of Theory Construction Approach
For the construction of the situation-specific theory for the diagnosis of AD, we used the Roy adaptation model, which is based on two theoretical pillars: adaptation and human systems 18. Adaptation as a concept refers to the process and result of the integration of the human being with his environment, while a human system corresponds to the set of interdependent parts that constitute a whole 18. Adaptation is a change that is generated in the presence of a stimulus. Roy defines a stimulus as everything that produces a response and constitutes the point of interaction of the environment with the human system 18. There are focal, contextual, and residual stimuli.
We also performed a scoping review to confirm the antecedents and consequences of AD with the scientific literature. We followed the methodology proposed by the Joanna Briggs Institute for developing scoping reviews 19. The questions that guided the review were: What are the antecedents of AD in adults with spinal cord injury? What are the consequences of AD in adults with spinal cord injury? Studies developed with adults with spinal cord injury, which investigated or described the antecedents or consequences of AD, were included. Primary studies of quantitative or qualitative design were considered for inclusion. No time limit was established for study selection because AD is still a little-known human response among health professionals, patients, and family caregivers.
The search strategy aimed to find published and unpublished literature (grey literature) in Spanish, Portuguese, and English. For this, the three-step search strategy was followed. In the first step, an initial search was conducted in the PubMed portal and the CINAHL database to identify studies on the review topic. The keywords in the title and abstract were placed, as well as the index terms used to describe the articles. In the second step, a search equation was adapted to all the databases, portals, or search engines included in the review, using the keywords and index terms identified in the first step (Appendix I). In the third step, a search for additional studies was performed in the literature references found. The three stages were developed by two reviewers independently.
Electronic searches were performed in the PubMed portal, in the CINAHL, BVS, ProQuest, and Science Direct databases. The unpublished literature was searched using Google Scholar, the Catalog of Theses and Dissertations (Capes), and Open Dissertations. All identified studies were sent to the Zotero reference manager, where duplicates were removed. Two reviewers independently conducted the entire study selection process. First, all studies identified in the searches were assessed, applying the inclusion criteria to titles and abstracts. The references of the studies that passed this phase were imported into the JBI SUMARI —JBI System for the Unified Management, Assessment, and Review of Information— 20. Finally, the full texts of the selected studies were retrieved to verify if they met the review’s inclusion criteria. When there was no consensus between the two authors regarding the study selection, a third reviewer was consulted to analyze and define the study’s inclusion in the review.
Data were extracted by one reviewer and verified by a second reviewer using an Excel spreadsheet. The antecedents and consequences identified in the studies were compared and grouped according to the listings in the NANDA-I to identify those that were identical, similar, or new. After this, they were classified into environmental stimuli (focal or contextual stimuli) and ineffective behaviors considering Roy’s adaptation model.
Definition of Main Concepts
In this study, we focused on two categories of concepts that were later integrated to form the SST. The first category of concepts pertains to the defining characteristics, related factors, populations at risk, and associated conditions proposed by the NANDA-I for the nursing diagnosis of AD. Defining characteristics are observable cues/inferences that cluster as manifestations of diagnoses 12. Related factors are antecedent factors with a patterned relationship with the human response and can be modifiable by independent nursing intervention 12. At-risk populations are groups of people who share sociodemographic characteristics that cause each member to be susceptible to particular human responses unmodifiable by the nurse 12. Associated conditions are medical diagnoses, diagnostic/surgical procedures, medical/surgical devices, or pharmaceutical preparations. These conditions are not independently modifiable by the nurse 12.
The second category of concepts includes ineffective behaviors, environmental stimuli, and the physiological adaptive mode under Roy’s adaptation model 18. Behavior is the internal or external actions and reactions under specified circumstances 18. Ineffective behavior is those responses that do not contribute to the integrity of the human adaptative system 18. Ineffective behaviors in the physiological mode are a manifestation of the integrity of the neurological function 18. Environmental stimuli are conditions, circumstances, and influences surrounding and affecting the development and behavior of persons, including residual (those stimuli having a determinate effect on the behavior of the individual), focal (internal or external stimuli immediately confronting the person), and contextual stimuli (all stimuli internal or external, affecting the situation; contribute to the behavior triggered by the focal stimuli) 18. Considering the scope of the SST, we did not consider the coping processes (regular and cognitive subsystem) as a concept.
According to the researchers’ judgment, it was determined that the defining characteristics are conceptually equivalent to ineffective behaviors, and the related factors and associated conditions are equivalent to focal stimuli. At the same time, populations at risk correspond to groups of people who can be inferred as vulnerable based on contextual stimuli. Nurses can influence focal or contextual stimuli to promote the adaptation of individuals with AD.
In the studies in the scoping review, we identified defining characteristics, related factors, populations at risk, and associated conditions for the nursing diagnosis of AD. Subsequently, these elements were analyzed through the lens of the previously mentioned Roy’s adaptation model concepts, leading to the categorization of these elements as either ineffective behaviors or environmental stimuli.
Developing a pictorial diagram
We developed a graphical representation to facilitate understanding the causal relationships of SST for the nursing diagnosis of AD.
Construction of propositions
We elaborate statements that explain the concepts and establish the associations between two or more concepts of the SST for the AD nursing diagnosis.
Establishment of Causal Relationships and Evidence for Practice
In this stage, the causal interrelationships and the evidence for nursing practice were established and described better to understand the clinical use of the nursing diagnosis. The causal relationships between the environmental stimuli and the study phenomenon were launched from the causation models proposed by de Oliveira Lopes et al. 17.
Results
Definition of the Theory Construction Approach
The search process in the different databases was conducted between August and September 2021, where 2413 potentially eligible studies were identified. After removing duplicates, the 1398 titles and abstracts were read, of which 209 met the eligibility criteria. Subsequently, the full texts of the same were obtained for review, resulting in the compliance of 94 studies with the established eligibility criteria. Figure 1 shows the selection and inclusion process of the studies.
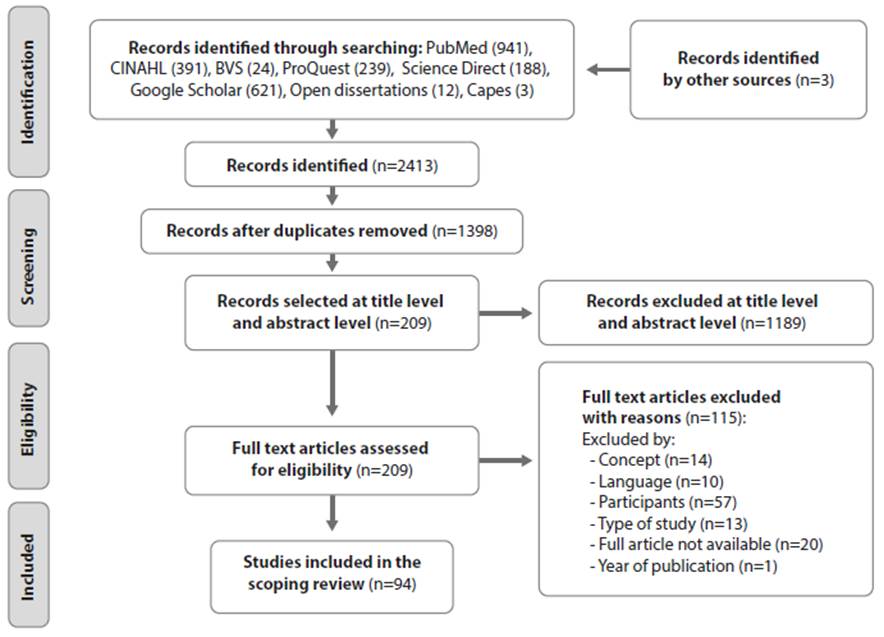
Source: Prepared by the authors
Figure 1 PRISMA Flow Diagram of the Study Selection and Inclusion Process
The articles included in the review were published between 1991 and 2021. Regarding the study design, 70 were case reports, 13 studies were case series, three were retrospective reviews, six were cross-sectional, and two were randomized clinical trials. The contribution of each of the included studies in identifying defining characteristics, related factors, populations at risk, and associated conditions of AD is presented in Appendix II.
Definition of Main Concepts
The concepts are related to the ineffective adaptation of individuals with spinal cord injury to focal, contextual, and residual stimuli and their consequent adaptive behaviors in the physiological mode to these etiological agents.
Through the scoping review, we identified 19 related factors listed in the NANDA-I; of them, 14 were categorized as focal stimuli and two as contextual stimuli from the perspective of the adaptation model. The related factors classified as focal stimuli were bowel distention, digital stimulation, suppositories, constipation, fecal impaction, wound, muscle spasm, bladder distention, bladder spasm, sexual intercourse, range of motion of exercises, enemas, constrictive clothing, and positioning. The related factors, cutaneous stimulation, skin irritation, sunburn, pressure over a bony prominence, pressure over genitalia, difficult passage of feces, and environmental temperature fluctuations, were not identified in any articles included in the review. The related factors, irritating stimuli below the level of injury and painful stimuli below the level of injury, were not considered to compose the final list of focal stimuli of the situation-specific theory because any of the triggering environmental stimuli for AD come from below the level of the lesion and are considered as irritating or painful stimuli. Also, we identified five new related factors that NANDA-I does not list: pressure ulcers, sexual stimulation, transfer, manual bowel evacuation, and breastfeeding. These were categorized as focal stimuli.
As the related factor instrumentation was considered ambiguous, we defined it as any manipulation of the urinary tract or gastrointestinal used for visualization, sample collection, and diagnostic or therapeutic purposes; this includes cystoscopy, urodynamic tests, colonoscopy, sigmoidoscopy, and anoscopy, among others. Based on this definition, instrumentation should be part of the associated conditions listed in NANDA-I for the diagnosis of AD and not of the associated factors, as is currently the case. Finally, the related factors, inadequate caregiver knowledge of the disease process and inadequate knowledge of the disease process by a person with spinal cord injury, were classified as contextual stimuli.
About 13 associated conditions were listed for diagnosis by NANDA-I, and the scoping review confirmed eight of them; these were bone fractures, detrusor sphincter dyssynergia, renal calculi, digestive system diseases, surgical procedure, urinary catheterization, venous thromboembolism, and urinary tract infection. We did not identify substance withdrawal, epididymitis, heterotopic bone, ovarian cyst, or pharmaceutical preparations as focal stimuli in the literature. However, other associated conditions not included by NANDA-I were identified; these were premenstrual symptoms, hyperthyroidism, Charcot spine, diseases of the urinary system, intramuscular injection, ejaculation, uterine contractions, chronic abdominal aortic dissection, musculoskeletal diseases, severe hyponatremia and hypokalaemia, breast congestion, and syringomyelia. The associated conditions were classified as focal stimuli also.
Of the 16 defining characteristics listed in the NANDA-I, the scoping review allowed us to identify 13 of them: paroxysmal hypertension, diaphoresis above the injury, bradycardia, tachycardia, pilomotor reflex, chilling, horner’s syndrome, blurred vision, nasal congestion, conjunctival congestion and pallor below the injury. The defining characteristics, red blotches on the skin above the injury, and diffuse pain in different areas of the head were not identified as written in NANDA-I; however, we identified flushing above the injury and pounding headaches in most of the included studies. The researchers considered these last terms for the theoretical derivation. The scoping review did not identify the defining characteristics of chest pain, metallic taste in the mouth, and paresthesia. However, we identified six defining characteristics not included in the NANDA-I: anisocoria, anxiety, double vision, hypothermia, nausea, and palpitations. All defining characteristics identified were categorized as ineffective behaviors in the physiological model.
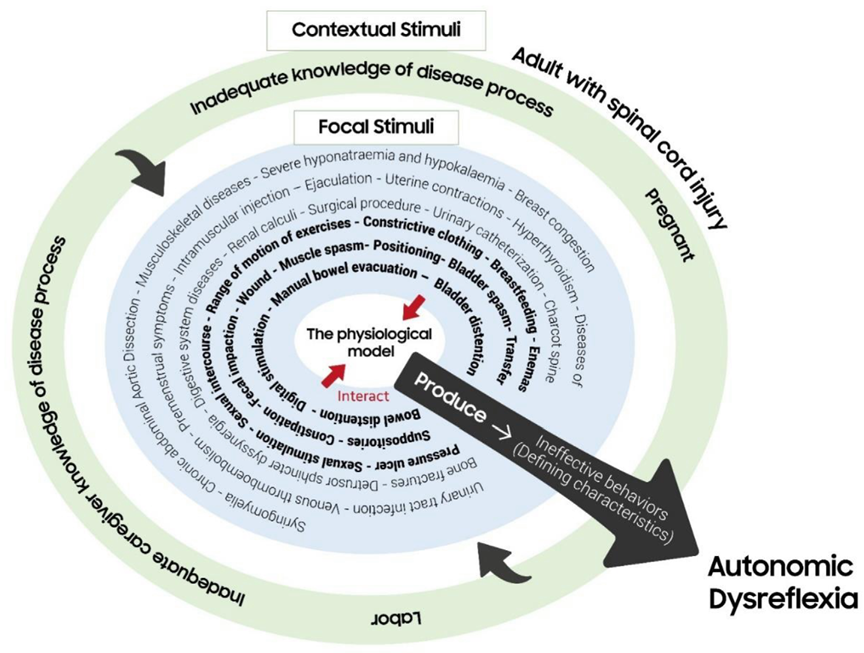
Pictogram F
Figure 2 summarizes the situation-specific theory for the AD nursing diagnosis, in which the relationships between the concepts can be observed.
Construction of Propositions
Seven propositions were developed for the situation-specific theory for AD nursing diagnosis:
Adults with spinal cord injury with a nursing diagnosis of AD frequently present the following ineffective behaviors: paroxysmal hypertension, headache, and diaphoresis above the level of injury.
Anxiety as an ineffective behavior of AD is explained exclusively by the alteration of neurological function in the physiological model.
Ineffective behavior paroxysmal hypertension in the presence of any focal stimuli is sufficient to diagnose AD in adults with spinal cord injury.
Focal stimuli come from below the level of spinal cord injury. These precipitate the ineffective behaviors that characterize AD.
Focal stimuli bowel distention, digital stimulation, manual bowel evacuation, suppositories, constipation, fecal impaction, wound, pressure ulcer, muscle spasm, bladder distention, bladder spasm, sexual stimulation, sexual intercourse, range of motion of exercises, enemas, breastfeeding, constrictive clothing, transfer, positioning, and the contextual stimuli inadequate caregiver knowledge of the disease process and inadequate knowledge of disease process are likely to be modified by the nurse.
The contextual stimuli’ inadequate caregiver knowledge of the disease process and inadequate knowledge of the disease process by adults with spinal cord injury exacerbate the effect of focal stimuli.
The contextual stimuli of pregnant or experiencing labor predispose a woman with spinal cord injury to develop AD.
Establishment of Causality and Evidence Relations for Practice
AD is a life-threatening human response because the ineffective behavior of arterial hypertension can generate devastating complications 21. Since nurses are one of the health professionals most in contact with adults with spinal cord injury, they must be able to identify the focal stimuli that precipitate dysreflexia and the ineffective behaviors through which it manifests itself.
The primary precipitating focal AD stimulus is bladder distension 22,23, which may be secondary to urinary retention, mechanical catheter obstruction, or poor positioning. Another focal stimulus related to the urinary system is bladder spasms.
This can occur as a complication of a neurogenic bladder 24 due to involuntary contractions of the detrusor muscle 25 because the bladder is irritable due to a urinary infection or the presence of a long-term urinary catheter 24.
Focal stimuli, digital stimulation, manual bowel evacuation, suppositories, range of motion of exercises, enemas, positioning, and transfer are present in the daily life of adults with spinal cord injury. They are part of the care of this person. These are stimuli that the nurse can anticipate as precipitating AD. Due to neurogenic bowel dysfunction, most adults with spinal cord injury require digital stimulation, manual bowel evacuation, suppositories, or enemas to induce defecation 26. In addition, immobility and altered sensitivity generate a risk of pressure ulcers, for which position changes must be made frequently. In the case of transfer (for example, to or from the bed, the chair, the bathroom), this is carried out by the patient or by the caregiver for the development of the activities of daily living of the person with a spinal cord injury 27. Neurogenic bowel dysfunction also alters colorectal motility, transit time, and emptying, often leading to constipation. In other words, constipation results from suspended stool movement throughout the colon, causing hard stools from the reabsorption of water and electrolytes through the intestinal lumen by inhibiting secretomotor neurons in the enteric nervous system 26. Constipation that is not adequately treated can cause fecal impaction 28. Both entities are also part of the causes of abdominal distension. Focal stimulus muscle spasms can present signs and symptoms similar to AD and trigger AD due to the intense pain they cause 29. On the other hand, sexuality is a complex and sensitive topic, and people with spinal cord injuries may not feel comfortable discussing it with the health team 30. Therefore, it is necessary for the nurse to feel comfortable addressing inherent aspects of sexuality that precipitate the appearance of AD, as is the case of sexual intercourse and sexual self-stimulation.
In the context of the situation-specific theory for AD, inadequate caregiver knowledge of the disease process and inadequate knowledge of the disease process are contextual stimuli that exacerbate the effect of focal stimuli. This is explained by the fact that a caregiver or a person with a spinal cord injury who is unaware of everything related to AD will be unable to identify the harmful stimuli that precipitate it. They will not be able to intervene, thus perpetuating and aggravating their effect. These two contextual factors should be of particular interest to the nurse because they are the main ones responsible for executing training and educational interventions aimed at improving the knowledge and care skills of formal and informal caregivers, as well as the person in a situation of dependency, as is the case of adults with spinal cord injury. In the case of pregnancy or experiencing labor, contextual stimuli are predisposing factors for AD. Hypertensive disorders during pregnancy and childbirth are frequent 31,32; hence, health professionals involved in the care of pregnant women must recognize whether the cause of hypertension is due to AD and not to hypertensive disorders such as preeclampsia 33 or in the case of parturients to labor pain, analgesic agents or hemodynamic changes 34.
Regarding ineffective behaviors, paroxysmal hyperreflexia exists when an increase of more than 20-40 mmHg in systolic blood pressure is identified concerning the baseline measurement 10. Although up to 88% of patients with AD present headaches and profuse sweating above the lesion 10, it is possible that some people experience an elevation of blood pressure without any associated symptoms 35. In such cases, the nurse could lose valuable time identifying noxious stimuli and even suspect AD only until the person presents severe sequelae.
Bradycardia, nasal congestion, conjunctival congestion, diaphoresis, and flushing above the lesion are ineffective compensatory behaviors of the parasympathetic nervous system to reduce hypertension secondary to sympathetic activity 22 produced by focal stimuli.
The ineffective behaviors, tachycardia, palpitations, chills, piloerection, and pallor below the injury, are mediated by sympathetic nervous system activity 22. In contrast, the action of the parasympathetic nervous system mediates ineffective behaviors, blurred vision, double vision, and anisocoria 22. In the case of headache behavior, this is a consequence of hypertension generated by the sympathetic system 36 and the reflex vasodilatation caused by the parasympathetic system 22. Regarding the ineffective behavior of hypothermia, the mechanism by which it occurs is not precise. Still, it is associated with profuse diaphoresis and thermoregulatory dysfunction in adults with spinal cord injuries.
Conclusion
This study successfully developed a situation-specific theory for the nursing diagnosis of AD based on the adaptation model of Sor Callista Roy. The theoretical derivation was carried out from the concepts of focal stimuli, contextual stimuli, and adaptive behaviors. Through seven propositions, it delineated the relationships between these concepts, unveiling the intricate dynamics of AD. From the perspective of Roy’s adaptation model, the nursing diagnosis of AD is manifested by ineffective adaptive behaviors in the physiological mode resulting from the interaction of noxious environmental stimuli with a regulatory subsystem compromised by a neurological function.
The situation-specific theory provides valuable insights for nursing practitioners and researchers working with individuals who have spinal cord injuries. Overall, the situation-specific theory contributes to the advancement of nursing knowledge and has the potential to enhance patient care for individuals with spinal cord injuries.
Implication for Nursing Practice, Research, and Education
The situation-specific theory for AD nursing diagnosis promotes the advancement of the nursing discipline by:
Provide a theoretical explanation of a human response that, if not intervened promptly, can trigger fatal consequences in those who experience it.
Enable improving care for adults with spinal cord injury by helping the nurse better understand how to support the person when experiencing AD. This understanding can materialize in developing care protocols that address the triggering focal stimuli of AD sensitive to nursing intervention and that take special consideration for groups vulnerable to developing AD, such as pregnant women or those experiencing labor.
Provide a theoretical basis for future research to obtain evidence of the AD nursing diagnosis’s content validity and clinical validity.
Evidence of the importance of educating the patient and formal and informal caregivers about AD. Because of this, from the nursing and continuing education programs and support programs for family caregivers, courses should be offered to improve knowledge about AD in these groups of people. These courses should emphasize the focal stimuli that trigger AD, the ineffective behaviors they generate in the physiological mode, and effective nursing interventions for said human response.
Given that the situation-specific theory is derived from a literature review and of Roy’s adaptation model, testing and validation of this proposal in practice is essential as the next step, since it is unknown how these constructs could assist and guide nursing practice, which is a fundamental element of this knowledge development.

