











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Cancer has become the main public health problem worldwide and is responsible for a high morbidity and mortality rate 1. As a result, intensive care units (ICUs) have been one of the most important sectors responsible for providing therapeutic support to patients with severe conditions and complications stemming from the cancer illness process 2.
ICUs are part of the Urgent and Emergency Care Network of the Unified Health System and include facilities fitted with high-quality technological resources for the treatment of critically ill patients who require uninterrupted multidisciplinary care 3,4.
The management of care in ICUs is undergoing recent changes, with the current model being replaced by one that aims to reduce mortality and improve the quality of life of survivors 5. It should be noted, however, that a balance needs to be reached between these perspectives and nursing care, based on basic human needs (BHNs), which can enable nurses and patients to become closer, including ICUs, where critically ill patients are present 6.
The reduction of mortality in ICUs is not an isolated factor, since critically ill patients require physical and mental health that results in rehabilitation and quality of life 7. In this setting, nursing professionals who work in ICUs develop competencies, skills, and approaches that enable them to provide adequate, empathetic, and effective care for their biopsychosocial needs 8. In addition, the creation of new technologies enables the development of advanced nursing practices, service organization, and safety in healthcare procedures, while keeping the team updated 9.
To mediate nursing practices, technologies which are defined as a set of material and non-material instruments that assist in providing healthcare are used 10. One such technology is “management technology” (MT), which is a modality used in nursing to systematize and bring theory and practice closer in terms of planning, executing, and evaluating the health process to improve it 11.
Patient data collection, especially at the time of admission, can help screen patients to identify their needs, facilitating the collection of relevant information that will assist the nursing team in planning and systematizing care to carry out individualized interventions in ICUs 12.
This study is innovative in the sense that it proposes an assistive technology designed to improve the quality of nursing care for patients admitted to oncology ICUs, given that the use of MTs is vital in nursing, as they enable a link between the healthcare team, the allocation of resources, professional preparation, and the supervision and evaluation of practices to improve care 13.
In this sense, this study aims to develop and validate the content of a nursing admission form for oncology ICU patients.
Materials and Methods
This is a methodological study 14,15, conducted from March 2021 to November 2022, to develop and validate a nursing admission form for oncology ICU patients. The study was operationalized in three stages 16: Identification of studies to compose the form’s content, content validation by specialist judges, and presentation of the form’s final version. For the preparation of this article, the guidelines of the Revised Standards for Quality Improvement Reporting Excellence (Squire 2.0), available on the Equator network website, were followed.
The first stage of the study consisted of carrying out an integrative review (IR [17]) and occurred from March to August 2021 to search for suitable studies to compose the research form’s content. Initially, the identification of the topic and the development of the research question were carried out based on the PICo strategy, which is used to adequately formulate the research question and literature search 18: What evidence is available on the admission of cancer patients to ICUs?
The literature search was performed by two authors, through the Brazilian Journal Website of the Coordination for the Improvement of Higher Education Personnel (abbreviated as Capes), which facilitated access to databases and electronic websites considered important in the healthcare setting: Virtual Health Library (BVS), adding databases such as the Latin American and Caribbean Health Sciences Literature (Lilacs), Medical Literature Analysis and Retrieval System Online (Medline) via PubMed Central® (PMC), and the Scientific Electronic Library Online (SciELO) repository of scientific works. It was decided that the search strategy would be based on the following descriptors in health sciences (DeCS) in Portuguese, English, and Spanish: “unidade de terapia intensiva” OR “unidades de cuidados intensivos” AND “coleta de dados” OR “recolección de datos” AND “oncologia” OR “oncología médica”, in combination with the following Medical Subject Headings (MeSH) in English: “intensive care units” AND “medical oncology” AND “data collection”. The association between DeCS and MeSH was applied to model the search strategies, using the Boolean operators AND, to find more results to support the IR.
As inclusion criteria, only complete articles were selected for reading, as well as books and editorials in Portuguese, English, and Spanish, with a time frame spanning from 2017 to 2022. Duplicate studies, review articles, reflections, letters to the editor, experience reports, case reports, formative opinions, research protocols, comments, and short communications were excluded.
Study selection was checked by two other researchers with expertise in reviews, one of them holds a master’s degree and the other a PhD. They were responsible for the two-stage selection, with masking to ensure a double-blind review and methodological rigor. After the first selection, title and abstract reading, and the relevant selections, a full reading was done. It should be noted that in cases where there was disagreement between the reasons for exclusion and inclusion, a third researcher (PhD) was consulted to define the selection. A total of 4,482 records were identified and, after applying the inclusion filters, reading the titles and abstracts, and reading the full text, 20 articles were included as the corpus for the qualitative analysis.
The second stage of the study: content validation, was performed from April to August 2022, with the participation of 15 specialists (nurses) and consisted of an intentional sample based on expertise criteria. The specialists had to meet at least two of the following criteria: be a specialist or master in the ICU field, be a healthcare professional with at least three years experience in ICU care, or be a professor of ICU or critical patient care. A sample size of 6 to 20 specialists was used as a parameter 19.
The entire process of validation by agreement, following the model proposed by Pasquali 20, was done online using the Google Forms platform. Each professional was sent an invitation letter via email (personal or corporate), which included the study objectives and the researchers’ identification. Those who accepted were sent two copies of the informed consent form and, upon returning it, were sent a copy of the first version of the form in PDF format and a questionnaire, divided into three sections: professional characterization, instructions for filling in the form, and sections with the instrument’s judgment questions, following a Likert scale 21, where 1 point stands for inadequate (I), 2 points for partially adequate (PA), 3 points for adequate (A), and 4 points for totally adequate (TA). Regarding the relevance, clarity, and applicability of the practice, the specialists rated: - 2 points for totally disagree, - 1 point for disagree, + 1 point for agree, and + 2 points for totally agree.
After organizing the data, the Chi-squared probability ratio test was used for independent samples 22; a significance level of p-value < 0.05 was adopted for the test. The ratio or percentage of experts who agreed on aspects of the instrument was calculated based on the content validity index (CVI), which was considered adequate when it was equal to or above 0.78 23. Items with a CVI lower than 0.78 were revised and adapted. Descriptive and inferential statistics were then applied. Computer resources were used, via processing in Microsoft Excel, using the Statistic Package for the Social Sciences (SPSS) version 24.0, all running in a Windows 7 environment.
The third stage, which was the presentation of the final version of the form, considered all the suggestions made by the specialists. The study is an excerpt from the residency conclusion work, entitled “Admission of Patients to an Oncology ICU: The Development and Validation of a Nursing Survey Form”, presented to the Uniprofessional Residency Program in Cancer Care in the Intensive Care Unit of the State University of Pará, Brazil, that was approved by the Research Ethics Committee, following the regulations of Resolution 466/2012, of the National Health Council, with opinion number 5.339.264 and certificate of presentation of ethical appraisal number 56210722.8.0000.5550.
Results
In the IR, a total of 4,482 publications were found; of these, when the exclusion filters were applied, 188 publications remained for analysis. From this, 168 publications were excluded —14 for being duplicates, 60 for not being available in full for reading, and 94 for not meeting the study’s objectives— totaling 20 articles which, after being read in full, were used in the study. The synthesis of the studies included in the IR led to three thematic categories: “incidence of ICU admission of cancer patients,” “the profile of cancer patients admitted to the ICU,” and “predictors of ICU admission for cancer patients.” Therefore, the thematic synthesis allowed content to be identified for inclusion in the nursing admission form for oncology ICU patients, which led to the structuring of the first version of the form with the following sections: identification (3 items), brief history (1 item), admission conditions (8 items), and physical examination (3 items), with a total of 15 items.
Fifteen experts participated in the content validation. Regarding age groups, 7 (46.7 %) were aged from 36 to 45, 4 (26.7 %) were aged from 26 to 35, 3 (20 %) were aged from 46 to 55, and 1 (6.7 %) was aged from 56 to 65. Regarding gender, there were 14 women (93.3 %) and one man (6.7 %). As for their training, 8 (53.3 %) had between 5 and 14 years of training, 6 (40 %) had between 15 and 24 years, and 1 (6.7 %) had between 25 and 34 years. Regarding time working in the ICU field, 8 (53.3 %) had been working between 1 and 10 years, 6 (40 %) between 11 and 20 years, and 1 (6.7 %) between 21 and 30 years. In terms of qualifications, 9 (60 %) were specialists, 4 (26.7 %) were doctors, and 2 (13.3 %) had master’s degrees. Of the 15 specialist judges, only 10 (66.7 %) stated they had completed at least one study related to ICU.
Regarding the mean and standard deviation, item 3.1. was the best-rated item with a mean score of 3.800 ± 0.414. Regarding Cronbach’s alpha, it can be verified that all the items were well evaluated, with a research reliability index higher than > 0.90 (excellent); regarding the CVI, it can be verified that only item 4.2 scored lower than the proposed value (CVI > 0.75), as shown in Table 1.
Table 1 Mean and Standard Deviation of the Specialist Judges’ Evaluation Questionnaire. Belém, Pará, Brazil, 2023
| Item | n | Mean | Standard deviation | Cronbach’s alpha | CVI |
|---|---|---|---|---|---|
| 2.1 | 15 | 3.600 | 0.632 | 0.957 | 0.933 |
| 2.2 | 15 | 3.467 | 0.640 | 0.957 | 0.933 |
| 2.4 | 15 | 3.333 | 0.724 | 0.959 | 0.867 |
| 2.3 | 15 | 3.400 | 0.632 | 0.958 | 0.933 |
| 2.5 | 15 | 3.400 | 0.828 | 0.957 | 0.800ns |
| 3.1 | 15 | 3.800 | 0.414 | 0.959 | 1.000 |
| 3.2 | 15 | 3.667 | 0.488 | 0.958 | 1.000 |
| 3.3 | 15 | 3.600 | 0.632 | 0.961 | 0.933 |
| 3.4 | 15 | 3.533 | 0.516 | 0.956 | 1.000 |
| 3.5 | 15 | 3.333 | 0.617 | 0.959 | 0.933 |
| 3.6 | 15 | 3.400 | 0.507 | 0.959 | 1.000 |
| 4.1 | 15 | 3.333 | 0.724 | 0.956 | 0.867 |
| 4.2 | 15 | 3.200 | 0.862 | 0.956 | 0.733ns |
| 4.3 | 15 | 3.133 | 0.834 | 0.958 | 0.867 |
| 4.4 | 15 | 3.400 | 0.632 | 0.957 | 0.933 |
| 5.1 | 15 | 3.600 | 0.632 | 0.959 | 0.933 |
| 5.2 | 15 | 3.400 | 0.507 | 0.960 | 1.000 |
| 5.3 | 15 | 3.333 | 0.816 | 0.954 | 0.800ns |
| 5.4 | 15 | 3.533 | 0.516 | 0.956 | 1.000 |
| Total | 15 | 65.467 | 9.441 | 0.960 | - |
Source: Prepared by the authors.
Regarding the sections and items of the instrument according to relevance, clarity, and applicability, it should be noted that all the items scored an adequate CVI (≥ 0.85), as shown in Table 2.
Table 2 Sections and Items of the Instrument according to Relevance, Clarity, and Applicability. Belém, Pará, Brazil, 2022
| Sections and items | Score 3 | Score 4 | CVI |
|---|---|---|---|
| 1. Identification | |||
| 1.1. Relevance | 2 | 13 | 1.000 |
| 1.1. Clarity | 3 | 12 | 1.000 |
| 1.1. Applicability | 2 | 13 | 1.000 |
| 1.2. Relevance | 3 | 12 | 1.000 |
| 1.2. Clarity | 3 | 12 | 1.000 |
| 1.2. Applicability | 2 | 13 | 1.000 |
| 1.3. Relevance | 2 | 13 | 1.000 |
| 1.3. Clarity | 3 | 12 | 1.000 |
| 1.3. Applicability | 3 | 12 | 1.000 |
| 1.4. Relevance | 4 | 11 | 1.000 |
| 1.4. Clarity | 4 | 10 | 0.933 |
| 1.4. Applicability | 4 | 11 | 1.000 |
| 1.5. Relevance | 4 | 11 | 1.000 |
| 1.5. Clarity | 4 | 11 | 1.000 |
| 1.5. Applicability | 4 | 11 | 1.000 |
| 1.6. Relevance | 2 | 13 | 1.000 |
| 1.6. Clarity | 3 | 12 | 1.000 |
| 1.6. Applicability | 3 | 12 | 1.000 |
| 2. Brief History | |||
| 2.1. Relevance | 2 | 13 | 1.000 |
| 2.1. Clarity | 2 | 13 | 1.000 |
| 2.1. Applicability | 1 | 13 | 0.933 |
| 3. Admission Conditions | |||
| 3.1. Relevance | 4 | 11 | 1.000 |
| 3.1. Clarity | 4 | 11 | 1.000 |
| 3.1. Applicability | 4 | 11 | 1.000 |
| 3.2. Relevance | 3 | 12 | 1.000 |
| 3.2. Clarity | 3 | 10 | 0.867* |
| 3.2. Applicability | 4 | 11 | 1.000 |
| 3.3. Relevance | 4 | 11 | 1.000 |
| 3.3. Clarity | 3 | 11 | 0.933 |
| 3.3. Applicability | 5 | 10 | 1.000 |
| 3.4. Relevance | 3 | 12 | 1.000 |
| 3.4. Clarity | 3 | 12 | 1.000 |
| 3.4. Applicability | 3 | 11 | 0.933 |
| 3.5. Relevance | 2 | 12 | 0.933 |
| 3.5. Clarity | 2 | 11 | 0.867* |
| 3.5. Applicability | 2 | 12 | 0.933 |
| 3.6. Relevance | 4 | 11 | 1.000 |
| 3.6. Clarity | 3 | 12 | 1.000 |
| 3.6. Applicability | 4 | 11 | 1.000 |
| 3.7. Relevance | 3 | 12 | 1.000 |
| 3.7. Clarity | 3 | 11 | 0.933 |
| 3.7. Applicability | 3 | 12 | 1.000 |
| 3.8. Relevance | 3 | 12 | 1.000 |
| 3.8. Clarity | 3 | 11 | 0.933 |
| 3.8. Applicability | 2 | 12 | 0.933 |
| 4. Physical Examination | |||
| 4.1. Relevance | 3 | 12 | 1.000 |
| 4.1. Clarity | 3 | 12 | 1.000 |
| 4.1. Applicability | 3 | 12 | 1.000 |
| 4.2. Relevance | 3 | 12 | 1.000 |
| 4.2. Clarity | 3 | 12 | 1.000 |
| 4.2. Applicability | 2 | 12 | 0.933 |
| 4.3. Relevance | 3 | 12 | 1.000 |
| 4.3. Clarity | 3 | 12 | 1.000 |
| 4.3. Applicability | 4 | 11 | 1.000 |
| 4.3. Relevance | 4 | 11 | 1.000 |
| 4.3. Clarity | 2 | 11 | 0.867* |
| 4.3. Applicability | 3 | 11 | 0.933 |
| 4.3. Relevance | 3 | 12 | 1.000 |
| 4.3. Clarity | 3 | 11 | 0.933 |
| 4.3. Applicability | 3 | 12 | 1.000 |
Source: Prepared by the authors.
The specialists recorded suggestions for the sections and items on the form in the instruments, which worked as a guide for restructuring the first version (Table 3).
Table 3 Suggestions from the specialists for the sections and items on the form. Belém, PA, Brazil, 2023
| Sections and Items | Suggestion |
|---|---|
| 1. Identification | |
| 1.2. Date of birth/age | I suggest adding “mother’s name.” |
| 1.4. Origin | I suggest complementing it with: “another city” or “another institution.” |
| 1.6. Reason for ICU admission* | I suggest adding “surgery” and “current framework history.” |
| 2. Brief History | |
| 2.1. PMH** | I suggest adding “surgical history.” I suggest adding “use of drugs/medications.” I suggest complementing it with “medication, food, or other allergies.” I suggest complementing it with “contrast allergy.” I suggest including whether the patient has “metastasis.” |
| 3. Admission Conditions | |
| 3.1. Vital signs | I suggest adding “glycemia.” |
| 3.2. Level of consciousness | I suggest either removing “RASS”*** or “level of sedation,” as both have the same meaning. I suggest specifying the meaning of “RASS”*** and “GCS”****. |
| 3.3. Respiratory assessment | I suggest adding “ventilation mode” to the mechanical ventilation item. I suggest adding “macronebulization.” |
| 3.4. Venous access | I suggest adding “PICC*****, Portocath, Shilley.” I suggest adding “insertion date.” |
| 3.5. Dressings | I suggest adding “skin assessment.” I suggest changing the terms “present” and “absent.” |
| 3.6. Drain | I suggest changing the terms “present” and “absent.” |
| 3.7. Nutrition | I suggest adding “GTT”******. I suggest complementing it with: if oral nutrition, “which preference and which refusal.” I suggest complementing it with: if NGT******* is open, “output characteristic.” |
| 3.8. Eliminations | I suggest specifying the meaning of “Bricker.” I suggest complementing it with “elimination properties.” |
| Physical Examination | |
| 4.2 Thorax | I suggest adding “other types of heart sounds.” |
| 4.3 Abdomen | I suggest changing the expression “positive/negative hydroaerial noises” to “hydroaerial noises present/absent.” |
| 4.4 Sacral region | I suggest changing the term “sacral region” to “skin assessment.” I suggest changing the term “sacral region” to “skin integrity” and adding the term “location.” |
| 4.5 ULs/LLs******** | I suggest separating the evaluation of ULs******** and LLs********. |
| Others | I suggest adding an item for “pain assessment.” |
| I suggest adding an item for “genitalia assessment.” |
Source: Prepared by the authors.
Key: *ICU — intensive care unit; **PMH — personal morbidity history; ***RASS — Richmond agitation-sedation scale; ****GCS — Glasgow Coma Scale; *****PICC — peripherally inserted central catheter; ******GTT — gastrostomy; *******NGT — nasogastric tube; ********ULs/LLs — upper limbs/lower limbs.
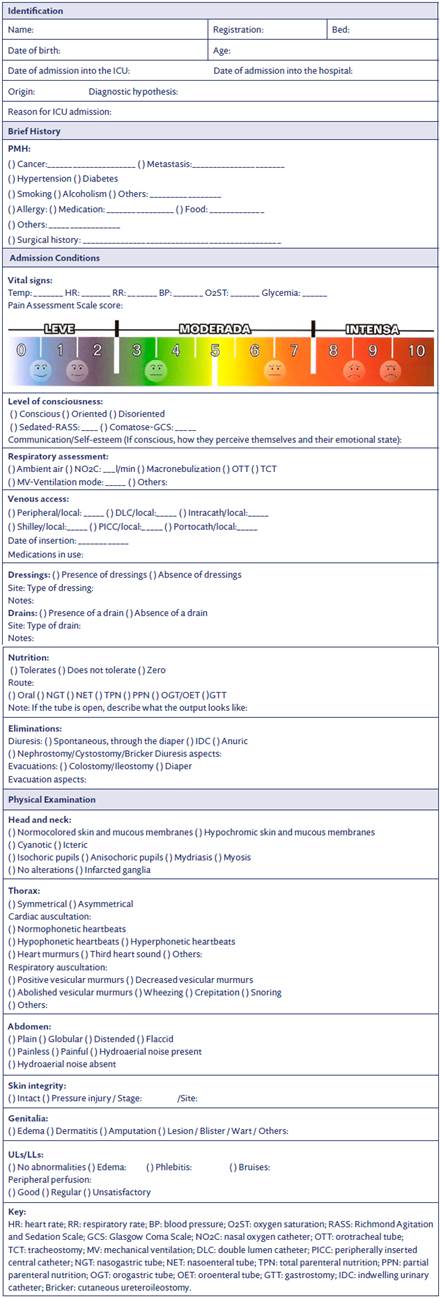
Based on the suggestions, the admission form was organized into item sections: Identification, brief history, admission conditions, and physical examination, with a total of four items (Figure 1).
Discussion
Over the last two decades, the number of cancer patients requiring intensive care has increased 2. In a prospective cohort study conducted with adult cancer patients undergoing systemic antineoplastic treatment, infection was the main reason for unscheduled hospitalization and, of these patients, 17.2 % presented with febrile neutropenia and 12.3 % with sepsis or septic shock 24.
It is noteworthy that among cancer patients, the elderly when admitted unexpectedly to ICUs, including after surgery, could benefit from patient-centered interventions such as rehabilitation, more frequent medical evaluations, and palliative care consultations if a well-defined investigation form were available 25. However, there are still certain difficulties related to the adequate management of cancer patients, mainly due to the stigmatization of the disease, which perpetuates doubts, especially regarding the signs and symptoms of hemodynamic deterioration that they may present, in which case it is strongly advised to admit them to ICU 26.
Correct assessment and early admission to the ICU offer increased chances of avoiding and managing complications stemming from cancer 27. The challenges of admitting oncology patients to ICUs are still an issue, but the literature on the adequate management of these patients, even in the face of an unexpected admission, is essential to adequately care and act for this population 28.
The survival rate of cancer patients admitted to the ICU is still higher than that of patients without the disease, but when compared to other diseases, such as chronic heart failure, intensive care stands out in terms of reducing mortality rates in this sector 29. In addition, cancer patients undergoing potentially curative therapy and even those with an advanced form of the disease, but with a chance of long-term survival, can benefit from ICU admission 30.
Some studies have found that the reasons why cancer patients are admitted to the ICU are age (elderly), operating time, bleeding, intestinal resection, hospital readmissions and low survival rates, hemodynamic instability, and fluid management 31, advanced-stage cancer, emergencies, sepsis/septic shock, respiratory failure 32, being male, of mixed race, married, post-surgical, hypertensive, diabetic, and with pulmonary comorbidities 33.
Diseases with a poor prognosis and high lethality, such as cancer, can cause distress, highlighting the need for more efficient and humanized care 34. It is noteworthy that ICU hospitalization is an uncomfortable process, involving isolation, a loss of privacy and a loss of autonomy for patients, who become highly dependent on the sector’s healthcare team, which highlights the importance of providing care that respects the principle of integrality and reaches every human dimension 35.
A study that aimed to develop a data collection tool for ICU patients based on the BHNs showed the tool could contribute to the proximity, interrelationship, and communication between nurses, patients, and family members, with attention focused on the patient’s individuality, favoring clinical reasoning and critical thinking regarding nursing interventions 36.
Furthermore, the results of an IR on the BHNs affected in cancer patients showed that the aspects of vascular regulation, nutrition, elimination, physical integrity, oxygenation, perception of sensory organs, lifestyle habits, neurological regulation, therapy, hydration, and thermal regulation were some of the empirical findings of the review that represent signs and symptoms that indicate alterations and that are included in the instrument presented in this study 37.
The present study found that the specialist judges’ sociodemographic characteristics were a prevalence of ages from 36 to 45 of females corroborates another validation study 38, which found that 89.7 % 26 of the judges were female, with ages ranging from 29 to 77, and 82.8 % 24 were aged over 40.
The judgment of the instrument contained in the health specialists’ evaluation questionnaire scored a CVI of 1.00 for the most part. This result was similar to a validation study performed with 17 judges, where the instrument evaluated scored a total CVI of 0.88 and was considered validated 39.
Item 2.5. of the specialist evaluation questionnaire, which addresses the theory of human needs proposed by Wanda Horta, infers the admission form includes most of the items contained in the BHNs subgroup that are pertinent to the admission of cancer patients to the ICU. In addition, to better cover the aspects of BHNs, “communication/self-esteem” was also included in the admission form. Regarding items 4.2 and 5.3, adjustments and additions were made, as proposed by the judges.
Regarding the instrument evaluated by the specialists, all the items scored CVI > 0.85 in terms of relevance, clarity, and applicability, resulting in only a few suggestions described by the specialists. Thus, the instrument is suitable for use by ICU nurses. A similar result was found in a study that also assessed its instrument for clarity and relevance, and scored a CVI above 0.8 for most items, showing a satisfactory level of agreement between the judges 40.
There was no need to do a second round of evaluation of the protocol by the judges since all the items met the minimum value set for the CVI. For the same reason, no items were excluded. It should be noted that after validation by the specialist judges, 8 items were modified, 31 items were included, and there were no items excluded, totaling 125 items in the final version of the instrument. Of the suggestions, 9 were not accepted. The “mother’s name” suggestion was not included because only two identifiers can be used.
It is usually recommended that patients should be identified using a wristband with two identifiers that allow professionals to confirm the data on the wristband with that contained in the medical record, such as the patient’s full name and/or date of birth and/or health service registration number and/or mother’s full name 41.
It is believed that the nursing survey form represents a milestone for nursing in the oncology ICU setting, since it is the first stage of the nursing process, and the information collected and the needs identified in this phase, are essential for the adequate management and implementation of the other stages.
Conclusions
It can be concluded that this assistive instrument is considered valid, since it exceeded the proposed cut-off point of > or = 0.80 (80 %), both for the individual evaluation of the questionnaire items and for the total index of the instrument for the three criteria. It is therefore of paramount importance for use in the ICU setting, improving the quality of the nursing care provided.
The construction and validation process of the survey form enabled the instrument to be evaluated, based on the judgment of specialist judges in the healthcare field, in which its content and structure were refined with the aim of better treating critically ill patients admitted to an oncology ICU. Furthermore, the methodology used proved to be suitable for the development and validation process, which could support the development of other technologies, on this and on other subjects that directly involve ICU care and cancer patients.
The nursing survey form for patients admitted to oncology ICUs is relevant as it is a technology that can mediate nursing care practices to render them more operational and systematized, thus providing comprehensive, resolutive, and quality care to patients.
As limitations of this study, it is worth noting that only content validation was carried out, but that the selection criteria and the number of specialist judges met all the requirements of this validation item; it is also worth noting that, given the demands for continuity projects, future validations, such as visual (by design professionals) and semantic (by the target audience) will be carried out, in addition to the usability verification.

