










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkUniversitas Psychologica
versão impressa ISSN 1657-9267
Univ. Psychol. v.5 n.3 Bogotá out./dez. 2006
MÓNICA NOVOA Y BLANCA PATRICIA BALLESTEROS DE VALDERRAMA*
PONTIFICIA UNIVERSIDAD JAVERIANA, BOGOTÁ
Correos electrónicos: mmnovoa@javeriana.edu.co / blanca.ballesteros@javeriana.edu.co.
ABSTRACT
The research presented in this article was aimed to specify in detail psychologist’s role in the context of an Intensive Care Unit, from the work at the Health Service Humanization Project, carried out by the Pontificia Universidad Javeriana from 1994 to 2000. This research is framed as a documental one, with a non-experimental design of an evaluative type aimed to evaluate the results of the activities carried out in function of the proposed objectives. Results were analysed at two levels: a qualitative level though Logical Frames Methodology and a quantitative level, with descriptive and correlation statistics. Results allowed to define psychologist’s role in three fundamental areas: attention to patients at the ICU, attention to family members or caregivers, and work with health personnel. These three areas are related to the objective of improving this people quality of life.
Keywords: Psychologist role, critical patient, Health Psychology, Intensive Care Unit
RESUMEN
El objetivo de la investigación presentada en este artículo fue especificar en detalle la labor del psicólogo en el contexto de una Unidad de Cuidado Intensivo a partir del trabajo en el proyecto Humanización de la Atención en Salud, desarrollado por la Pontificia Universidad Javeriana, durante el período comprendido entre 1994 y 2000. Esta investigación se enmarca dentro de la investigación documental, bajo un diseño de corte no experimental tipo evaluativo valorando los resultados de las actividades desarrolladas en función de los objetivos propuestos. Los resultados fueron analizados en dos niveles, a nivel cualitativo, por medio de la metodología de marco lógico y a nivel cuantitativo, mediante estadística descriptiva y correlacional. Los resultados permiten definir la labor del psicólogo en tres aspectos fundamentales: Atención a pacientes que ingresan a UCI, atención a familiares y acompañantes del paciente y trabajo con personal de salud. Estos tres aspectos están relacionados con los objetivos de mejorar la calidad de vida de estas personas.
Palabras clave: Labor del psicólogo, Paciente crítico, Psicología de la salud, Unidad de cuidado intensivo.
The Intensive Care Unit (ICU) is the place where attention is given to patients with a vital crisis, that is, compromise of one or more vital organs and thus requiring continued intervention and permanent monitoring by health caregivers. It is undeniable that such circumstances become a source of stress for the ill person, his or her family, and for the health personnel. It is therefore a field where the psychologist has multiple functions and levels of intervention that deserve to be clearly defined. The importance of considering the role of the psychologist in an ICU is supported by Scragg, Jones and Fauvel (2001), who confirm that treatment in an ICU can generate psychological problems in patients that interfere with quality of life, specially anxiety and depression (47% of patients) and posttraumatic stress indicators (38% of patients). The Health Psychologist, specially in the ICU, needs to have personal and professional skills that enable him to interact with people in special conditions, different to those commonly found in other professional fields. Likewise, he must integrate knowledge that transcend those of his own discipline into his professional skills, in order to complement his explanations with knowledge coming from biomedical sciences and other social sciences.
In this direction, the role of the psychologist in the ICU is compatible with that of the health psychologist in Colombia (Flórez, 1995, 2002). Nevertheless, it must be made clear that this description of roles doesn’t include the specifics of required actions for working in the different contexts, which is why it is necessary to clearly establish the role in a particular context such as the ICU, within the general frame of a hospital, considering that the intervention for a patient with asthma cannot be considered equivalent as one for a patient in critical state.
In view of its characteristics, the ICU is one of the hospital places that has a deeper impact on patients and family members, specially because of the use of high technology devices such as monitors displaying cardiac activity, blood pressure and other important data that reveal the patient’s condition; automatic sphygmomanometer, mechanic ventilation, intravenous lines, nasogastric tubes, vesical tube and infusion pumps, among others. The aforementioned means physical conditions that include noises emitted by the monitoring devices and permanent artificial illumination, which favours the loss of day-night cycles; constant presence of healthcare professionals, frequently watching the patients and performing procedures on them. Besides, the use of devices establish conditions such as dependence of them, immobility and nakedness in order to ease performing of the procedures and cleaning and care. Likewise, both having an endotracheal tube and the effect of certain medications cause difficulties for communication (Caro, Grimaldos, Novoa & Serrano, 1995; Paredes, Parra, Urueña & Serrano, 1997; Bermúdez, Sanz, Novoa & Serrano, 1999; Aldana, Morales, Novoa & Rodríguez, 2000). A review of studies performed by Cook, Meade and Perry (2001) summarises the psychological impact of being in the ICU and Fontaine (1994) describes in detail the most common conditions of discomfort and distress for patients in an ICU, i.e., thirst, insomnia, pain, restraint, inability to speak, immobility, noise, trouble breathing, confusion, inability to determine current time and day, hopelessness, loneliness, seeing other patients and have doctors and nurses saying more than what the patient can understand.
Generally speaking, different studies agree in considering the physical conditions of the ICU as generators of psychological distress (Aldana, Morales, Novoa & Rodríguez, 2000; Bell, Fisher & Loomis, 1978; Davis, 1978; Durbin, 1995; Fontaine, 1994; Hayden, 1994; Samples, 1998; Simini, 1999; Wilson, 1987; Wunderlich, Perry, Lavin & Katz, 1999). Fowler & Smyth (1997) have pointed out that the conditions of stress that critical patients are exposed to often have a detrimental effect on their responses to disease, because they favour an increase in cardiovascular effort and oxygen consumption, which is reflected in a longer stay in the ICU and a progressive decrease of their biological and psychological stability.
This situation of stress is shown in several ways, as described by Blanco (1986): at the somato-physiological level there is an increase of neurological reticular activity, catecholamine secretion and steroid production, which has effects on bodily functions, specially on the endocrine system. Secondly, at the motor level there often is some direct action performed by the patient in order to change the aversive conditions (aggression, removal of tubes, resisting procedures, etc.) and finally emotional responses appear, such as anxiety, rage, sadness, depression and delusions.
On the other hand, within the context of critical disease there are many degrees of severity of the patient admitted to the ICU. A measure that has shown to be effective to determine the severity of the patient and the probability of death is the APACHE II (Knaus, Draper, Wagner & Zimmerman, 1985) and APACHE III (Pappachan, Millar, Bennett & Smith, 1999). Both scales have been used in the ICU and its records have supported the psychological role, as they allow for prediction of the prognosis and adjustment of actions accordingly.
The scientific literature also reveals the necessity of taking into account the diverse psychological profiles, in order to be able to respond to patient demands in the ICU, since they determine the response of the patient to the situation of being hospitalised and being in the ICU.
Even patients with well structured psychological profiles may present with very childlike behaviours during their long stay in the ICU (Horta, Plazas & Serrano, 1998). In the same way, it is possible to find, in ICU patients, psychological disturbances such as anxiety (Epstein & Breslow, 1999; Hansen-Flaschen, 1994; McCartney & Bolan, 1994; Tesar & Stern, 1995) and depression (Paredes, Parra, Urueña & Serrano, 1997) and the term ICU psychosis or ICU Syndrome has been specifically coined to refer to affective, behavioural and cognitive abnormalities in ICU patients, related to sleep deprivation, exposure to sensory overload, environmental restriction and medication (Durbin, 1995; Fontaine, 1994; Sivark, Higgins & Seiver, 1995). Besides, the different experiences in the ICU (intubation or extubation, feelings of loss of control, among others), together with vulnerability factors can trigger the development of a Posttraumatic Stress Disorder (PTSD) in some patients (Horta, Plazas & Serrano, 1998).
It is also important to pay attention to the collateral effects of medications frequently used in the ICUs (Tekeres, 2000; Tung & Rosenthal, 1995) and conditions of immune suppression associated with the conditions of the ICU patient (DeKeyser, 2003; Krueger, Thoth, Floyd & cols., 1994; Schrader, 1996).
Regarding interventions, some studies have shown that behavioural and environmental interventions are beneficial, combined with pharmacologic treatment (Blacher 1987; Chlan, 1998; Fontaine, 1994; Granber, Engberg & Lundberg, 1999; McGuire, Baste, Ryan & Gallagher, 2000; Posen; 1995; Sivak, Higgins & Seiver, 1995). Music as a valid alternative has been suggested and applied by several authors, with different goals, including the control of the noisy environment that inhibits sleeping and promotes anxious reactions, helping promote relaxation and handling pain (Biley, 2000; Fontaine, 1994; Horta, Jaimes, Rodríguez & Serrano, 2000; Magill, 1993), easing medical procedures and decreasing use of medication (Bonebreak, 1996).
Another mode of intervention related to environmental design includes that described by Costello (2000) as a model of intervention for preoperative Augmentative Alternative Communication (AAC), for patients programmed to stay in the ICU after surgery. Even though reported data are anecdotic in nature, they show beneficial effects of the intervention, as described by patients, family and healthcare professionals.
In regard to the problem of delirium in the ICU, Roberts (2001) states that it continues to be a problem and its clinical handling focuses on procedures designed to save the life; nevertheless, healthcare professionals require skills to prevent it, which means to be able to identify it on time and have a thorough understanding of how the brain, the most important organ in these cases, works, as well as being aware of the features of the physical environment in order to be able to help patients cope with those conditions, specially when they cannot be modified or eliminated (for instance, immobility and devices). This author suggest the reduction of noise, specially at night, using music and familiar voices, speaking in a calm tone, looking at the patient, without using medical jargon that may disturb even more or induce irrational ideas; reorientation to time and space is also a factor to take into account in these cases, in order to alleviate the sensory deprivation; thereby the importance of the presence of close people, such as family members, that support or directly help with actions of communication and sensory stimulation in order to relieve the anxiety caused by the foreign environment of the ICU. In opinion of this author, it is imperative to provide an appropriate handling of pain, because of its relationship with irritability and its sleepdisrupting effect, both associated with the presentation of delusional syndrome. In cases of delusion, it is necessary to calm family members and warn them about the syndrome; it is important to offer support to both the patient and them by explaining the nature of the syndrome, the visual course followed by the disease and the possible treatments.
With regard to that, DeKeyser (2003) states that both psychologists and nurses are able to carry out several actions that allow patients to increase their feelings of security and comfort. In the study by Laitinen (1996), patients emphasised the importance of having a closer relationship with the professionals in charge, because they believe that perceived calmness and feelings of security and acceptance will depend on the quality of this presence.
Also related to the aforementioned, it is worth to mention the contributions of environmental psychology in hospital environments and specifically in the ICUs (Trites, Galbraith, Sturdavant & Leckwart, 1970; Bell, Fisher & Loomis, 1978; Carlopio, 1996).
Finally, it is necessary to consider the technological advances in the field of security. For example, Morris (2002) refers to security in the clinical environment based on structures that reduce the probability of danger, in evidence of actions that increase favourable results in explicit directions tending towards decisions to implement said actions, taking into account that a 1% error rate threatens the life of the patient; computerbased support tools are a great help for standardizing clinical decisions and guiding therapeutic measures, including algorithms for generation of relevant information and protocols that include more complex rules in order to reduce the margin of error. This author states that such protocols are specific for each patient, so that the individualised treatment is preserved, while clinical decisions are standardized, which is a crucial aspect in order to ensure the safety of the patient.
Considering what was just presented about bidirectional implications of psychological processes and the conditions of the patient in the ICU, this research had the main objective of specifying the role of the psychologist in an ICU in detail, so as to contribute in the process of answering the questions of the Psychology and Health Research Group. The specific objectives were to critically analyse the interventions of the psychologists in the ICUs in order to delimit their functions with basis on the information available in the archives of the Humanization of Health Services project between 1994 and 2000, to design and create an electronic data base and bibliography cards on the thematic axes proposed by the Psychology and Health Research Line and to contribute to its strengthening by enhancing the existing knowledge and by making new questions on the grounds of the collected information.
Method
Design
This research is framed as a documental one, with a methodology of analysis and systematization of existing information in a series of reports and observations, interviews and questionnaire record forms belonging to the Health Service Humanization Project developed by the PUJ, specifically in the ICU in during the aforementioned period. A non-experimental evaluative design was used in order to evaluate the results of the programmes and, through that evaluation, to determine the role of the psychologist in the ICU. This type of research is characterised by valuing the results of the programmes in terms of the proposed objectives; it is carried out taking social research methods into account due to its scientific foundations (Tamayo & Tamayo, 1999).
Units of Analysis
1. Semestral reports from the Health Services Humanization Project developed by the PUJ in the Intensive Care Unit of the San Rafael University Hospital. There is a total of 7 reports, written between 1995 and 2000.
2. Undergraduate (Psychology) theses under the direction of Ps. Carmen Serrano, head of the Health Services Humanization Project. 4 undergraduate theses were produced between 1995 and 2000. Those studies were derived from the project practicum.
3. Available evaluation forms of patients and family members. These instruments were:
• Patient Personal Data Survey: a form for collection of relevant information for the process of recovery and the emotional well-being of the patient during his stay at the ICU (Ballestas, Duarte, Otero & Serrano, 1996). It contains identification data and information such as length of stay at the ICU, causal of admission and if he was prepared or not; has open-ended questions about biopsychosocial characteristics of the patient. First 11 items were answered by the family and the other 6 by the patient.
• Evaluation of information: administered to the patient’s family members in order to identify their needs and expectations, as well as the failures detected by them with regard to the evaluation, in order to be able to intervene on these aspects together with the rest of the team. It contains identification data for both the patient and his family; it includes 9 questions dealing with the information they had received on the patient’s health status. Questions were: dichotomous, multiple selection and Likert scale, and the second part of each item had an open-ended question regarding the explanation or justification of the answer given to the first part.
• Post-ICU patient interview: Administered to patients upon discharge from the ICU; its objective was to evaluate the service during the stay at the unit and thus improving the service according to the suggestions. It allowed for identification of the needs of the patient at the ICU, the strengths and weaknesses of the service and it became a qualitative record on the conditions that patients experienced during their stay. It contains identification and information data such as length of stay in days, cause of admission and if the patient was prepared or not. It includes 17 questions about the information they had on the ICU before being admitted, the process of entering the ICU, the stay (relationship with the healthcare professionals at the ICU, visits, type of communication, worries, discomforts, information received on their health status and evaluation of the attention they received) and suggestions for improving the attention given in the ICU. The questions were dichotomous, multiple selection, open-ended and Likert scale; some of them had a second part where people wrote the explanation or justification of the answer given to the first part.
Materials
For the first part of the research two double-entry collection matrices were used as direct instruments. The first one consisted of 55 variables that collected information about the projects’ objectives, concise actions, results, among others. The second one comprised 74 variables that requested sociodemographic information of the patients attended at the ICU, characteristics of the admission, general considerations of the condition and responses to post-ICU interviews; it also contained information provided by the family. The relevant information about each report and each dissertation was collected in each matrix.
With interpretative and theoretical construction goals, the Logical Frame Scheme was used for the second part (Inter-American Development Bank – IDB, 1997), which is a tool to ease the process of conception, design, execution and evaluation of projects. The purpose is to provide a structure for the processes of planning, communication and information related to the project. Nevertheless, it can be also used as an ex post-facto evaluation. It can be modified several times during the preparation and execution of the project. According to the IDB (1997), the logical frame not only provides precise elements that decrease the ambiguity when writing projects, but also provides information for executing, monitoring and evaluating the project. The indicators are clearly verifiable since the elements for evaluating the project are established.
Procedure
Main focuses of work were established from the objectives of the investigation. Initially, reports and theses pertaining to the investigation were located, for a total of 11 documents. The following categories of analysis were stated for each document:
• Type and strategies of psychological intervention.
• Target population (patient, family, ICU personnel, institutional, others).
• Effectiveness of the intervention.
• Mechanisms of evaluation used.
These categorical proposals were adjusted according to the information recorded, taking into account: • Source of the information (patient, health personnel, family).
• Cause of intensive care (type of vital crisis).
Data dictionaries and corresponding data bases were built for collection of data related to the documents themselves and to the patients admitted to the ICU during the period analysed. Basically, the discriminated information of each report was considered.
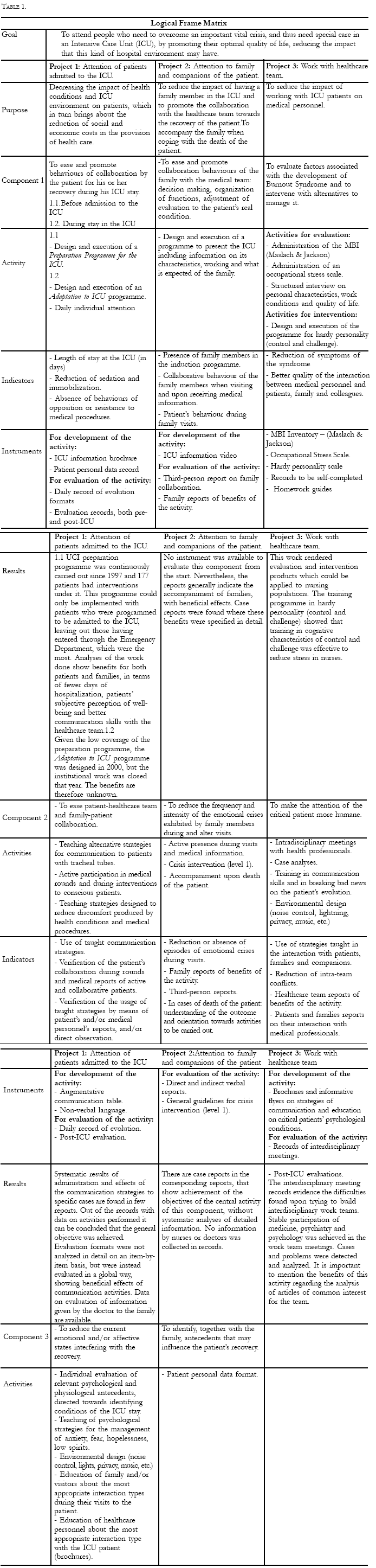
Information was then typed into a data base and the evaluation strategy was determined. Logical Frame Methodology was deemed appropriate for this process. The information on the reports was analysed, which produced an analysis matrix with three basic components (in relation to the patient, to the family and to the health personnel). This matrix can be seen in the Results section.
The information related to the users was evaluated by means of descriptive and correlational strategies. Finally, data bases were cleaned up and the analysis of results was performed.
Results
In order to analyse the results two aspects were considered; one qualitative in nature by using the methodology of Logical Frames (BID, 1997) and content analysis. The other one was quantitative in nature, mainly by means of descriptive statistics, with the use of central tendency measurements (mean, median, mode) and dispersion measurements (ranges, standard deviation) in the information related to the users. Correlational methods were also used (Pearson and Spearman correlations, Kendall and contingency coefficients) in order to establish relationships among relevant variables in the subject data.
Descriptives of the sample
For this study, information was found on 1.235 male and female patients. With regard to the most relevant sociodemographic data, we found that the 61-71 age group was the most represented (10.60%) of the 91.66% of patients with age data. The less represented group was that of ages between 0 and 10, with 0.40%, of which, upon discriminated analysis, corresponds to subjects under 3 years old, which is in agreement with the expected values according to demographic incidence.
There was a smaller number of people with ages over 81, which is coherent with the country’s life expectancy. 44.7% were male, and 55.3% were female.
More patients were female, specially in the age groups 21-30, 31-40 and 61-70, but a larger number of male patients was found in the age groups 41-50, 71-80 and 91 or more.
Only 328 people reported their marital status. 192 (58.7%) were married, 48 (14.7%) were widowers and 40 (12.2%) were single.
The sample ranged between illiteracy and high levels of education. Of the 306 people that reported their education level, 45.42% had elementary education, 9.80% were illiterate, 7.52% were professionals (had college-level education) and 1% had some level of postgraduate education. Education levels higher than undergraduate were reported only in patients older than 41 years. Nevertheless, lower levels of education and the highest levels of illiteracy were also reported in that very sample.
As for remissions, we were able to establish that General Surgery (28.40%) and Neurosurgery (24.20%) were the services that remitted the most patients, followed by Orthopaedic Surgery, Internal Medicine and Obstetrics-Gynecology; Rheumatology and Emergency Medicine only remitted 0.2% of the total.
Medical conditions were evaluated according to variables such as sedation, intubation, immobility and sepsis. 254 patients had information on sedation, and 109 (42.9%) were sedated; 134 (61.5%) of 218 with information on intubation were intubated; 76 patients (30.9%) of the 246 with information on mobility were immobile.
Psychological work was done with 236 ICU patients. Companionship activities only were carried out with 30.10% of them, and both companionship and preparation programme were performed with the rest of them. Out of 1209 patients with information, 177 (14.6%) were included in the Psychological ICU Preparation Programme, contrasting with 1032 (85.4%) that were not included.
71 cases had reports on psychological conditions, either reported by family members or recorded by Psychologists. 12 (16.9%) identified psychological problems derived from their stay at the ICU (mainly depression and anxiety). It is important to note here the evaluation that patients made of the psychological work and the sufficiency of the time devoted to attention.
In the evaluations administered to patients after discharge from the ICU, it is important to point out some aspects related to the information and previous knowledge they had before admission to the ICU, who gave them that information, the evaluation they made of their stay and the attention received. Concerning the topic of information they had before admission, out of 126 reported cases, 70 (55.6%) identified the ICU as the place where very ill people are attended; 9 (7.1%) as the place where people recovers after surgery and 8 (6.3%) as the place in the hospital where more specialized equipment and devices are used. This information, according to the patients, was obtained, in most cases (15.7%), by direct previous knowledge (they had been admitted before or had visited someone), 14.2% was informed by psychologists and 12.6% by doctors.
Relationships among variables
After the descriptive analysis, a correlational one was performed that intended to determine the possible relationships among the relevant variables for this research. These variables were specifically related to preparation, communication and psychosocial aspects of the patients, the families and elements of the service given by the ICU. As for the nominal variables related to interval-level variables, the Eta coefficient, which indicates the direction of the measurements, was employed.
The correlation between what people imagined of the ICU and the information they had was significant (r = 0.230, p < 0.01). Likewise, the form of communication was related to the quantity of time at the unit (Eta = 0.481). The patient’s concerns were not significantly related neither with the length of stay nor with the preparation received. A relationship was found between consideration of visit time and suggestions, meaning that visit time determines the suggestions made (Eta = 0.561).
Significant relationships were found between the evaluation of medical attention and the perception of being treated in a humane way (r = 0.288, p < 0.01), the evaluation of the time devoted by the healthcare team to attention of the patient (r = 0.295, p < 0.01), and the evaluation of the service of the ICU (r = 0.253, p < 0.01). Significant relationships were also found between the perception of being taking care of in a humane way and the evaluation of time devoted to attention by the healthcare team (r = 0.407, p < 0.01) and the evaluation of the service of the ICU (r = 0.280, p < 0.01). Relationships were also found between the evaluation of the information received, the perception of being taken care of in a humane way (r = 0.471, p < 0.01) and the consideration of visit times (r = - 0.271, p < 0.05), that is, the better the perception of the information, the less disagreement with the allotted visit time.
With regard to the evaluation of psychological work, significant relationships were found with the sufficiency of the time of attention by the Psychologist (r = - 0.338, p < 0.01) and dedication of time for attention by the healthcare team (r = 0.164, p < 0.05); significant relationships were also found between evaluation of visit times and evaluation of ICU service ((r = 0.279, p < 0.01), that is, the better valuing of time, the better evaluation; finally, between evaluation of time devoted to attention by the healthcare team and the evaluation of ICU service (r = 0.279, p < 0.01).
In statistical analysis, and in agreement with the objectives of the programmes, prepared patients tended to stay at the ICU for shorter periods (r = 0.070, p < 0.05), which fulfilled the purpose of reducing the impact of health conditions and environment of the ICU on patients.
Finally, Table 1 presents the results of the analysis performed with the Logical Frame Methodology, which systematizes, in the Projects cell, the Psychologist’s work nuclei at the ICU, as a function of the type of population and of the objectives of the analysis.
Discussion
Discussion of the results is made in light of the review of the specialized literature available and of the results from the analysis of reports and archives of the Humanization of Health Services project.
Generally speaking, this documental research allowed us to establish the role of the psychologist in an ICU, which consists of individual attention to patients, attention to family members and companions, work with the medical and paramedic personnel and environmental design. These conclusions are in accordance with those reported by Ramos and Pereira (2003) about the factors of intervention of the Psychologist in the ICU, factors referred to family, the individual and the hospital.
From the methodological viewpoint, it is important to bring to notice that this research evidences the need to clearly separate the effects of biomedical conditions from those of the pharmacological treatment and the particular conditions of the ICU on the patients’ psychological state during their stay at the ICU. In this line, Fontaine (1994) includes conditions derived from the pharmacological treatment into the category of biomedical conditions, which have important side effects such as cognitive and behavioural alterations – changes in state of consciousness, orientation, memory, attention, sensoperception and thought among them, some in the category of ICU psychiatric abnormalities. In pragmatic terms, controlling these alterations as good as possible becomes necessary, because, as this author points out and as evidenced by this research, they may imply potential damages to the patients themselves or to the healthcare team in charge of them. When possible, the intervention should pose as little restrictions as possible and should appeal in minimum amounts to sedatives. As found by this research, knowledge of the patients’ characteristics provided information to guide the medical intervention in the noted direction.
Results are also consistent with what was described by authors such as Epstein and Breslow (1999) regarding anxiety in ICU patients and their families, so that it becomes important to pay attention to indications, both verbal and physiological, susceptible of being monitored by people that have contact with the patient. Interventions directed towards managing anxiety showed significant effects, but the important thing is to bear in mind that such interventions must be continued, because the conditions of an ICU, already described, may be thought of as favouring or feeding anxiety, as found in 17% of the 71 cases evaluated during and after their stay at the ICU, who showed problems such as anxiety and depression related to their ICU stay.
Taking into account the importance of psychological variables in the quality of life of ICU patients, this research allowed for a reaffirmation of the need to know those variables as soon as possible, in order to be able to determine whether they are previous conditions or they are brought about by the stay at the ICU and the medical conditions. For example, the work at the HUCSR with patients described as being in «low spirits» or conflictive families allowed us to give direction to the interventions performed on them during visits and during the periods of communication with the healthcare personnel.
Coincidences were found among what was stated by DeKeyser (2003), Granberg, Engberg and Lundberg (1999), Krueger et al. (1994), Simini (1999) and Thomas (2003) regarding factors that were more worrying and distressing for patients during their ICU stay, such as noise levels, permanent illumination, conversations by unknown people, mobility restriction and social loneliness. As said, the patients’ experience of stress is not only related to sepsis and trauma, but is also heavily affected by environmental conditions; hence the importance of work based on environmental design. From the set of complaints and reports of distresses it can be concluded that the most frequent psychological stressors were pain, sleep deprivation, fear or anxiety and nudity.
It is important to observe how opportunity and effectiveness of psychological interventions may allow to break feedback cycle existing between environmental conditions and psychological conditions and the physiological conditions inherent to the morbid state, which can, together, make a naturally aversive stay worse, as described previously. This aspect is related to psychoneuroimmunology, a specialty that has allowed for a gradually increasing understanding of that feedback cycle. In this way, work at the HUCSR ICU with the goal of evaluating the Psychological Preparation Programme based on measurements of anxiolytic medication showed important benefits, given the reduction in medication use by the patients and the length of hospitalization and immobilization requirements, which is in accordance with better biological recovery indices for patients (see Ballestas, Duarte, Otero & Serrano, 1997). These results are even more relevant when considering the high psychological, social and economic costs associated with ICU services.
The project developed at the HUCSR did not examine any interventions for pain, which has been associated with effects on the neuro-endocrine and immune systems, and the psychological science has created intervention strategies for pain which use medication in minimum amounts and have shown benefits in diverse pathologies.
As for the environmental intervention, and taking into account that the environmental design is not under the Psychologist’s control in most ICUs, it is very important to understand that intervention in low cost aspects (for example music therapy, regulation of illumination according to sleep cycles) can turn a potentially damaging factor into an ally of the recovery process.
With regard to the interventions performed, the results support the relevance of psychological support both for the patients and for their families, specially for those conditions perceived as aversive, reported by several authors (Durbin, 1995; Fontaine, 1994; Hayden, 1994; Wunderlich, Perry, Lavin & Katz, 1999), including those related to essential aspects such as nudity, immobilization and presence of other patients. All these conditions imply restriction of movement and loss of privacy, and have repercussions on loss of perceived control, psychological reactivity and lack of feelings of protection, as pointed out by Aldana, Morales, Novoa and Rodríguez (2000).
Relevance of psychological support provided to the patient was evidenced in the post-ICU measurements. A suggestion to the Psychology and Health Research Group would be to conduct follow-up evaluations of the interventions in a longer term, considering reports by Horta, Plazas and Serrano (1998) regarding the possibility of developing Posttraumatic Stress Disorder and other psychological abnormalities.
Concerning evaluation made about psychology work, in some cases by patients and in others by families, it is worth noting that most of them evaluated it as good, and claimed for more time of this service. This aspect ought to be explored more carefully in relation not only to the psychologist’s clinical skills, but to the risk of reducing the psychologist-patient work time when privileging environmental interventions and interventions with family and healthcare teams. It should be pointed out that psychologists were not full-time at the ICU, since the whole work was framed in a project-based practicum, with the already mentioned implication that few patients were prepared; this evidences the need for hospitals to have staff psychologists as ICU personnel.
The results of intervention with family and companions of the patient are also consistent with the literature reviewed, as it is regarded that family has a double function, the first one as supporters of the patient and the second as agents that ease the work of the healthcare personnel. The role of psychological intervention with the family in handling information and reducing the negative impact of ICU on the family was evident in this research, by enhancing communication with the patient and the healthcare team. A general conclusion worth noting of this is the change in beliefs held by family and companions about the psychological conditions of their hospitalized family members, going from considering them as completely biological entities, incapable of contact and influence by the environment, to understanding that despite their physiological condition they continue to be psychologically active beings.
It was evidenced that family members want to be informed about the medical evolution of their patient and about the way that they can help with the patient’s recovery. In this way, the Psychological Preparation for ICU programme and the presence of the Psychologist during the visits were activities that should be highlighted.
This research evidenced, with regard to the work of the professional team in the ICU, the need of building interdisciplinary groups in order to have a real impact on the quality of attention of the patient and the quality of life of the professionals. The difficulty reported in the documents on joint work leads to the conclusion that one of the jobs of the psychologists in the ICU is to be a part of said team, showing clear skills in their discipline and in the relationships between their discipline and the relevant biomedical disciplines. One of the roles would then be to give orientation to the healthcare personnel as to improving the relationship with the patients and their families, which is in the way suggested by authors such as Laitinen (1996), based on the importance, claimed by patients, of having a closer relationship with the professionals in charge; it is indicated that perceived tranquility and safety and acceptance feelings depend mostly on the quality of this presence. Krueger et al. (1994) also state that one of the jobs of the psychologists in the ICU is educating the healthcare personnel on the importance of handling environmental conditions in favour of patients’ comfort. Despite not being documented in the reviewed reports, it is relevant to point out the encounter of the roles of each discipline with a presence in the ICU, especially between Nursing and Psychology. As mentioned previously, most publications about attention to critical patients come from Medicine and Nursing, the latter being mainly concerned with the effects of human interactions, so that the inclusion of psychologists in the ICU could have been perceived as invasive, with the subsequent implication of a role conflict of the nursing personnel. Consequently, one suggestion is to clearly define the roles of each profession and comment them with the members of the team, in order to promote cooperative behaviours that ease, instead of interfering with, the quality of the service in the ICU, as well as the quality of the work environment.
Another work front with the healthcare personnel was related to the design of interventions tending to reduce the impact of working at this kind of units and thus improving their quality of life. Noteworthy of that work is the effectiveness of the intervention in the hardy personality pattern (control and challenge) as a strategy for stress management and the improvement of interpersonal relationship conditions among ICU professionals.
There are numerous suggestions for future research. On the one side, research on psychoneuroimmunology should continue, with the incorporation of an objective instrument of measurement such as the APACHE III (Pappachan, Millar, Bennett & Smith, 1999), which will provide for a more accurate estimation of the biomedical changes in different moments of the patient’s stay at the ICU, together with the supplemental measurements of psychological conditions. On the other hand, more research is needed on the improvement of the measures, including other sources of information different from patients and family members, that allow for validation of the work.
As suggested by Morris (2002), it is important to consider the technological advances in the field of security and involve the psychologist’s work into them, in order to accurately establish the intervention protocols that include more complex work rules and measure their effectiveness. Finally, it is worth considering the need of continued implementation of the proposals made in the reviewed reports, such as the ICU adaptation programme, as well as ensuring the continuity of the programmes when started. The latter is important when taking into account the results of the preparation programme on psychological variables like discomfort, which was reported by a significantly lesser number of prepared patients in comparison to those who weren’t prepared; as for the contents of discomfort, nonprepared ones included more psychological aspects, while prepared ones referred more to physical disturbances due to their health condition, including pain, having to be laying down and the length of stay.
The time variable is worth taking into account for further research, in the different dimensions included, length of stay in the ICU, visit length and time in contact with the healthcare team. Most reports of discomfort were made by patients that stayed between 1 and 7 days, in comparison to those with longer stays, which can be related to the process of adaptation; it would be hypothesized that, after a week, the patients would have recognized the conditions of the ICU, including environmental and relational ones, and would have got used to them, not implying any liking or satisfaction about their status of ICU patients. Worth noting is the result on the evaluation of sufficiency of time devoted by the healthcare team, since while most regarded the time as sufficient, also considered the psychological intervention time and the visit time to be insufficient. Also related to the length of stay at the ICU, it is good to be important to discuss the results in light of the type of information required by family members. It seems that the longer the stay at the ICU, the more the needs of information deal with getting ready for a worse outcome, including the death of the patient. As a consequence, the role of the psychologist also includes situations of mourning.
Finally, the Humanization of Health Services Project made an important contribution to the topic of quality of life upon considering it to be susceptible of being studied in critical patients. To date, quality of life had been a topic of interest in patients with chronic and terminal diseases, but not in ICU patients, probably because of the conditions inherent to their state.
References
Aldana, C., Morales, C., Novoa, M. & Rodríguez, B. L. (2000). Programa de la Unidad de Cuidados Intensivos. Informe I Semestre. Faculty of Psychology, PUJ. Unpublished document. [ Links ]
Ballestas, M., Duarte, A. M., Otero, A. & Serrano, C. (1996). Impacto de un programa de preparación basado en información sensorial y estrategias de comunicación en pacientes de la Unidad de Cuidado Intensivo. Dissertation. Faculty of Psychology, Pontificia Universidad Javeriana de Bogotá. Unpublished document. [ Links ]
Bell, P., Fisher, J. & Loomis, R. (1978). Environmental Psychology. Philadelphia: W.B. Saunders. [ Links ]
Bermúdez, A. M., Sanz, C., Novoa M. & Serrano, C. (1999). Informe final del trabajo realizado por el equipo de psicología en la Unidad de Cuidados Intensivos de la Clínica San Rafael. Proyecto de humanización de la atención en salud. Faculty of Psychology, PUJ. Unpublished document. [ Links ]
Biley, F. C. (2000). The effects on patient well-being of music listening as a nursing intervention: a review of the literature. Journal of Clinical Nursing, 9(5), 668-677. [ Links ]
Blacher, R. S. (Ed.) (1987). The psychological experience of surgery. New York: John Wiley and sons. [ Links ]
Blanco, A. (1986). El estrés ambiental. En F. Jiménez y J. I. Aragonés (Eds). Introducción a la psicología ambiental. Madrid: Alianza. [ Links ]
Bonebreak, K. (1996). A sound way to induce relaxation and natural sleep: a safe alternative to sedation. American Journal Electroneurodiagnostic Technology, 36(4), 264-268. [ Links ]
Carlopio, J. R. (1996). Construct validity of a Physical Work Environment Satisfaction Questionnaire. Journal of Occupational Health Psychology, 1, 330-344. [ Links ]
Caro, S. L., Grimaldos, D., Novoa, M. & Serrano, C. (1995) Humanización de la calidad de la atención en salud. Unidad de Cuidados Intensivos. Informe, proyecto de Humanización de la Atención en salud. Faculty of Psychology PUJ, unpublished document. [ Links ]
Chlan, L. (1998). Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance. Heart and Lung, 27(3), 169-76 [ Links ]
Cook, D. J., Meade, M. O. & Perry, A. G. (2001). Qualitative studies on the patient’s experience of weaning from mechanical ventilation. Chest, 120(6) (Supplement): 469S-473S. [ Links ]
Costello, J. M. (2000). AAC intervention in the intensive care unit: The Children’s Hospital Boston model. AAC: Augmentative-and-Alternative-Communication, 16(3), 137-153. [ Links ]
Davis, B. K. (1978). The expanded measurement of patients’ psychological stress responses to being in the coronary care unit. Milit Med. 143, 203-225. [ Links ]
DeKeyser, F. (2003) Psychoneuroinmunology in Critical Ill Patients. AACN Clinical Issues, 14(1), 25-32 [ Links ]
Durbin, Ch. (1995). Sedation of the Agitated, Critically ill patient without an artificial Airway. Critical Care Clinics, 11(4), 913-934 [ Links ]
Epstein, J. & Breslow, M. (1999). The stress response of critical illness. Critical Care Clinics, 15, 17-32. [ Links ]
Flórez, L. E. (1995). El rol del psicólogo de la salud en Colombia. Presented at the XXV Interamerican Congress of Psychology. San Juan de Puerto Rico, junio. [ Links ]
Flórez, L. E. (2002). Psicología de la salud en Colombia: Orígenes, evolución y estado actual. Ponencia en el Simposio Psicología de la Salud en Iberoamérica, III Congreso Iberoamericano de Psicología, Bogotá, julio. [ Links ]
Fontaine, D. (1994). Non-pharmacological management of patient distress during mechanical ventilation. Critical Care Clinics, 10, 651-657. [ Links ]
Fowler, J. & Smyth, K. (1997). Application of a transactional model of stress and coping with critically ill patients. Dimensions of critical care nursing, 16, 292-299. [ Links ]
Granberg, A., Engberg, I. B. & Lundberg, D. (1999). Acute confusion and unreal experiences in intensive care patients in relation to the ICU syndrome: part II. Intensive Critical Care Nurse, 15, 19-33. [ Links ]
Hayden, W. (1994). Life and near-death in the Intensive Care Unit. Critical Care Clinics, 10, 651-657. [ Links ]
Horta, D., Jaimes, C., Rodríguez, A. & Serrano, C. (2000). Influencia de música de naturaleza relajante en pacientes hospitalizados en una Unidad de Cuidado Intensivo bajo la condición de ventilación mecánica. Dissertation. Faculty of Psychology, Pontificia Universidad Javeriana de Bogotá. Unpublished document. [ Links ]
Horta, D., Plazas, C. & Serrano, C. (1998). Unidad de Cuidado Intensivo. Hospital Clínica San Rafael. Informe, proyecto de Humanización de la Atención en Salud. Faculty of Psychology PUJ. Unpublished document. [ Links ]
Inter-American Development Bank, IDB (1997). La matriz de marco lógico. Retrieved June, 2003, Available at: http://www.iadb.org/cont/evo/SPBook/lamatriz.htm. [ Links ]
Knaus, W., Draper, E., Wagner, D. & Zimmerman, J. (1985). Apache II: A severity of disease classification system. Critical Care Medicine, 13, 818-829. [ Links ]
Krueger, J. M., Thoth, L. A., Floyd R. & cols. (1994). Sleep, microbes and cytokines. Neuroimmunomodulation, 1, 100-109. [ Links ]
Laitinen, H. (1996) Patient’s experience of confusion in the intensive care unit following cardiac surgery. Intensive Critic Care Nurse 12, 79-83 [ Links ]
Magill, L. (1993). Music therapy in pain and symptom management. Journal of Palliative Care, 9(4), 42-48. [ Links ]
McCartney, J. & Boland, R. (1994). Anxiety and delirium in the Intensive Care Unit. Critical Care Clinics, 10(4), 673-680. [ Links ]
McGuire B.E., Baste, C. J, Ryan, C. J. & Gallagher, J. (2000) Intensive care unit syndrome: a dangerous misnomer. Archives of Internal Medicine, 160, 906- 909. [ Links ]
Morris, A. H (2002).Decision support and safety of clinical environments. Quality & Safety in Health Care, 11, 69 - 75. [ Links ]
Pappachan, J. V., Millar, B., Bennett, B. D. & Smith, G. B. (1999). Comparison of outcome from intensive care admission after adjustment for case mix by the APACHE III Prognostic System. Chest, 115, 802-810. [ Links ]
Paredes, O., Parra, A., Urueña, D. & Serrano, C. (1997). Programa de la Unidad de Cuidados Intensivos. Informe, proyecto de Humanización de la Atención en Salud. Faculty of Psychology, PUJ. Unpublished document. [ Links ]
Posen, D. (1995). Stress Management for the Patient and Physician. The Canadian Journal of Continuing Medical Education, 7(1), 65-82 [ Links ]
Ramos, R. & Pereira, F. (2003) Relación entre la frecuencia de la conducta de lavado de manos y la prevalencia de neumonía nosocomial en los pacientes de la unidad de cuidados intensivos de una clínica privada de Bogotá. En Memorias, II Congreso Latinoamericano de Psicología de la Salud, Cartagena, septiembre. [ Links ]
Roberts, B. (2001). Managing delirium in adult intensive care patients. Critical Care Nurse ,21(1), 48-56. [ Links ]
Samples, R. (1998). Family coping during critical illness. Dimensions of Critical Care Nursing, 17(2), 100-112. [ Links ]
Sánchez, L. (2002). Psicología y salud: la situación en Venezuela. Ponencia en el Simposio Psicología de la Salud en Iberoamérica, III Congreso Iberoamericano de Psicología, Bogotá, julio. [ Links ]
Schrader, K. A. (1996). Stress and immunity after traumatic injury: the mind-body link. AACN Critical Issues, 7, 351-368. [ Links ]
Scragg, P., Jones, A. & Fauvel, N. (2001). Psychological problems following ICU treatment. Anaesthesia, 56(1), 9-14. [ Links ]
Simini B. (1999). Patient’s perceptions of intensive care, Lancet, 354, 571-572 [ Links ]
Sivak, E., Higgins, T. & Seiver, A. (1995) The High Risk Patient: Management of the Critically ill. New York: Williams & Wilkins. [ Links ]
Tamayo & Tamayo, M. (1999). La investigación. En Aprender a investigar (3ra. Ed.). Bogotá: ICFES. [ Links ]
Tekeres, M. (2000). Pharmacology for anaesthesia and intensive care. European Journal of Anaesthesiology, 17, 531. [ Links ]
Tesar, G. & Stern, T. (1995). Neuropsychiatric Disturbance in the Critically Ill Patient. En E. Sivak, T. Higgins & A. Seiver (comp.), The High Risk Patient: Management of the Critically Ill (p.p. 29-40). New York: Williams & Wilkins. [ Links ]
Thomas, L. A. (2003) Clinical management of stressors perceived by patients on mechanical ventilation. AACN Clinical Issues, 14(1), 73-81. [ Links ]
Trites, D., Galbraith, F., Sturdavant, M. & Leckwart, J. (1970). Influence of nursing unit design on the activities and subjective feelings of nursing personnel. Environment & Behavior, 3, 303-334. [ Links ]
Tung, A. & Rosenthal, M. (1995). Patients requiring sedation. Critical Care Clinics, 11, 4, 791-657. [ Links ]
Wilson, V. S. (1987). Identification of stressors related to patients’ psychological responses to the surgical intensive care unit. Heart and Lung, 16(3), 267-273. [ Links ]


{kind=link}