Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkUniversitas Psychologica
Print version ISSN 1657-9267
Univ. Psychol. vol.13 no.1 Bogotá Jan./Mar. 2014
Clinical Case Formulation in a Context of Health*
Formulación de caso en un contexto de Salud
Diana Paola Pulido-Castelblanco**
Monica María Novoa Gómez***
Pontificia Universidad Javeriana, Bogotá, Colombia
*Colciencias and Pontificia Universidad Javeriana (PPTA ID 00004156)
**Pontificia Universidad Javeriana, Bogotá, Colombia. E-mail: diana.pulido@javeriana.edu.co
***Pontificia Universidad Javeriana, Bogotá, Colombia. E-mail: mmnovoa@javeriana.edu.co, Re-searchID: E-1869-2011
Recibido: junio 20 de 2012 | Revisado: junio 25 de 2013 | Aceptado: agosto 17 de 2013
Para citar este artículo
Pulido-Castelblanco, D., & Novoa Gómez, M. (2014). Clinical case formulation in a context of health. Universitas Psychologica, 13(1), 187-205. doi:10.11144/Javeriana.UPSY13-1.ccfh
Abstract
The objective of this research was to determine the usefulness of a clinical formulation model (Muñoz & Novoa-Gómez, 2010), in two health-related issues: obesity and oncology. Seven cases were formulated using an A-B-S design. Results show similarities about the internal validity, in comparison with was reported in previous studies like Caycedo, Ballesteros and Novoa-Gómez (2008), Pachón and Novoa-Gómez (2009) and Muñoz and Novoa-Gómez (2010), showing the usefulness of this model and its application in a health context. Therefore, it is important to continue the replication of the model and extend the generalizability of the data in order to get the external validation of it.
Keywords authors: case formulation; functional analysis; behavioral assessment; behavioral model
Keywords plus: clinical psychology; psychotherapy; validity
Resumen
El objetivo de la presente investigación fue determinar la utilidad de un modelo de formulación clínica (Muñoz & Novoa-Gómez, 2010), en dos problemáticas relacionadas con la salud: Obesidad y Oncología. Siete casos fueron formulados usando un diseño A-B-S. Los resultados indican que en los casos estudiados en esta investigación, se mantienen los resultados respecto de la validez interna, reportados por las anteriores investigaciones realizadas por Caycedo, Ballesteros y Novoa-Gómez (2008), Pachón y Novoa-Gómez (2009) y Muñoz y Novoa-Gómez (2010), mostrando a su vez la utilidad del modelo al ser aplicado en un contexto de salud. Es importante continuar la replicación del modelo, para ampliar la generalización de los datos y poder llegar a contar con la validación externa del mismo.
Palabras clave autores: formulación de caso; análisis funcional; evaluación conductual; modelo comportamental
Palabras clave descriptores: psicología clínica; psicoterapia; validez
Clinical Case Formulation in a Context of Health
The clinical psychologist has the social responsibility to generate strategies and respond to several problems of people who consulted him. One of the ways in which a commitment to good practice is fulfilled, is through the use of case-formulation models for understanding the particular case, and many factors relevant to it.
That is why researchers at the Research Group on Psychology and Health at Pontificia Universidad Javeriana (PUJ), have designed a guide model for case formulation, as a tool that serves the clinical psychologist to plan timely and efficiently interventions for each case; favoring people to adjust to different contexts in which they interact (Muñoz & Novoa-Gómez, 2010a). This, in turn, will improve training strategies for qualified clinical psychologists. For this aim, several studies in the research of psychological wellbeing and quality of life, and psychological assessment and intervention (Cay-cedo, Ballesteros, & Novoa-Gómez, 2008; Pachon & Novoa-Gómez, 2009; Muñoz & Novoa-Gómez, 2010a), have sought the model validity and reliability from an idiographic perspective, consistent with the principles of behavior analysis (Muñoz & Novoa-Gómez, 2010a).
Case Formulation
The case formulation can be understood as an idiographic research methodology aimed at understanding the behavioral problems of the consultants, and identifying the factors from which they are a function, so that it can provide work alternatives that can generate positive changes in them; and thus, make it possible to meet their needs (Hayes & Haas, 1988). This methodology is useful, not only to organize the information obtained from the evaluation, but also to facilitate the generation of hypotheses that account for predisposing factors, acquisition and maintenance, which are related to the problems of the consultants (Castro & Angel 1998; Bergner, 1998; Eells, Kendjelic, & Lucas, 1998; Haynes, Leisen, & Blaine, 1997; Haynes,
Mumma, & Pinson, 2009; Haynes & Williams, 2003; Sturmey, 2008). It develops and implements an intervention that improves the efficiency of the process ahead; understanding effectiveness in the field of clinical psychology as the ability of an intervention to produce changes according to defined objectives (Ferro & Vives, 2004).
Eells (2001), Kahneman and Klein (2009) have noted that case formulation improves the clinical judgment, to such extent that decisions are not based on the therapist's intuition, but on the relations identified for the particular case, which have been explored from a careful assessment of the motive for consultation and problems of the client. This consequently leads to decrease the likelihood of standardized, inefficient or ambiguous interventions will done.
Formulation model from behavioral analysis
However, the formulation model — developed from studies of the Research Group on Health Psychology from the PUJ — has sought to be consistent with the principles of behavior analysis (Caycedo, Ballesteros, & Novoa-Gómez, 2008; Pachon & Novoa -Gómez, 2009; Muñoz & Novoa-Gómez, 2010), meaning that it had to be built in order to analyze the relationships between the environment and people's responses (Catania, 2007). From the analysis of behavior it is well known that this relationship involves three terms, namely: antecedent context that precedes or occurs before the response, which gives occasion for the behavior; the response, and the consequence, which refers to the effect that has the response on the environment. This consequence may be reinforcing or punishing, and the aim is to study the systematic covariation between these three terms, which have been called functional relationship (Michael, 2004).
From the perspective of behavioral case formulation, the model is useful for identifying functional relationships between behavior and context, using functional analysis as a methodology characteristic of the model (Caycedo, Ballesteros, & Novoa-Gó-mez, 2008; Iwata & Worsdell, 2005; Muñoz & Novoa-Gómez, 2010), understood as a strategy to identify the sources of reinforcement that maintain the behavior. Also, formulation integrates relevant information in decision-making processes about the case, such as the relationship between the context and behavior variables of a client, its effects and gives possible options to change the problem (Iwata & Worsdell, 2005; Haynes et al., 1997). According to Haynes et al. (2009) and Sturmey (2008), interventions will be more effective if they arise from a functional analysis rather than a diagnosis, or a purely descriptive analysis, since they will realize that relationships are features within the behavioral repertoire of each particular client. That leads to planning interventions that modify these relationships in a specific manner, and increases the likelihood of lasting changes (Haynes & Williams, 2003; Ribes, 1990).
Although several formulation models have been developed (Butler, 1998; Haynes & Williams, 2003; Horowitz, Rosenberg, Urena, Kalehzan, & Hallo-ran, 1989; Nezu, Nezu, & Lombardo, 2004; Perry, Cooper, & Michels, 1987; Persons, 1991; Tarrier, 2006). Mumma and Smith (2001) noted that there are few empirical studies related to reliability and validity in the use of these models. Authors such as Carrascosa and Valdivia (2007), Mumma and Smith (2001) have pointed out that validation is indispensable so that the hypotheses arising from such formulations provide effective treatment planning, in order to decrease the frequency of relapses, desertions and extensive processes, and consequently improving the quality of people's lives.
The clinical formulation model developed by the PUJ research group in Psychology and Health has followed several investigations that have contributed to the internal, content, predictive, clinical and judges validity criteria, whose findings show the importance of replicating the model in a different population that has been intervened with the model in previous studies, so we tried to identify its usefulness in people with various problems related to health contexts.
This is consistent with the statements made by Barlow and Hersen (1988), as well as Sidman (1960), who pointed out that the most suitable behavioral analysis methodology is the systematic replication of the previous study. In this case, means the application of the formulation in different populations, environments and conditions. Systematic replication will facilitate the identification of variability sources between contexts and individuals, which will lead to take control of a greater number of factors; reducing the variability, and will allow to good results achieving in a greater number of clients. This increases the likelihood that data are reproducible in new cases, leading to a possible generalization of data (Johnston & Pennypacker, 1980; Hayes, Barlow, & Nelson-Gray, 1999; Mumma & Smith, 2001). As noted by Tukey (1969), as well as by Cumming and Maillardet (2006), replication allows us to confirm data, and this is the basis of the reliability and significance, being it central to the scientific method.
Thus, the present investigation was aimed to replicate the use of the model in case-related with health problems. In order to meet this objective, it is necessary to (a) functionally analyze related problematic behaviors in population with health problems, (b) formulate each case using the formulation model to organize and analyze case information, (c) design and implement an idiographic intervention in each one, and (d) compare the effects obtained from the participants.
Method
Design
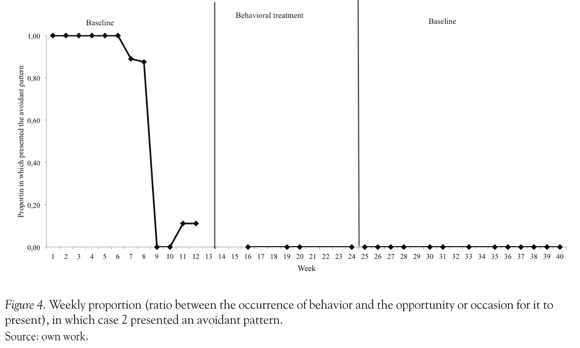
This research followed a clinical case design. Seven cases were formulated using an A-B-S design, in which the A phase is the establishment of the baseline, which provides information about the parameters in which the behavior occurs. Stage B refers to the application of treatment. Finally the S phase refers to the tracking after the withdrawal of the treatment variable (Kazdin, 2001).
Participants
Participants from obesity group. People with a diagnosis of morbid obesity resulting from an interdisciplinary assessment team, which met the criteria for classification of body mass index (BMI) > 30, who were also candidates for bariatric surgery, and who were referred by the Obesity Group of Hospital Cardiovascular del Niño de Cundinamarca (HCC) to start psychotherapeutic support. They were treated at the HCC.
Case 1 (AC). A 49 year-old female, with incomplete primary education, she works independent as the owner of a miscellany. She is a single mother of two women and a man; she has two daughters 28 and 30 years old, and her son is 23 years old. She is from a middle socioeconomic status (3 out of 6), and lives with her youngest son. When she started the program she had a BMI of 51.14.
Case 2 (CC). A 47 year-old female, housewife, with complete primary schooling. She lived in middle socioeconomic status (3 out of 6). She lives with her husband and her youngest son. She has 2 children, by that moment her oldest daughter was 27 years old and her son was 23. When she started the program she had a BMI of 46.78.
Case 3 (MC). A 37 year-old female, with high school education, full secretarial and technical studies; she works as a community mother in a preschool of the Colombian Institute of Family Welfare (Instituto Colombiano del Bienestar Familiar - ICBF). She lived in middle-low socioeconomic status (2nd out of 6) with her husband and three daughters (10, 7 and 2 years old). When she started the program she had a BMI of 38.10.
Case 4 (SR). A 35 year-old female, with complete high school education and culinary studies. She occasionally worked in different household maintenance activities in a brother's middle class home. She lived with her husband and two of his four children (19, 18, 13 and 9 years old). When she started the program she had a BMI of 41.91.
Participants from oncology service. People diagnosed with cancer and caregivers of people diagnosed with cancer, derivate from the psychological service of oncology at the Hospital San Ignacio, who were adults and volunteered to participate in the research. They were treated at San Ignacio Hospital Oncology Center.
Case 5 (AD). A 52 year-old man, with full high school education, married, a restaurant owner. He lived with his wife in the middle socioeconomic status (3rd out of 6), and had three children 33, 32 and 28 years old. He was diagnosed with colon CA a year before starting therapy.
Case 6 (EC). A 51 year-old female, with incomplete secondary education, wife, who lived with her husband and three children aged 33, 32 and 28 in the middle socioeconomic status (3rd out of 6). She is the Primary caregiver of her husband, who at 52 was diagnosed with colon CA, a year before starting therapy. She presented hemorrhoids, gastritis, occasional chest pains, headache, constant muscle pain insomnia and loss of appetite.
Case 7 (VS). A 54 year-old female, with incomplete university studies, married, dedicated to home, from middle-high socioeconomic status (4th out of 6), living with her husband, her youngest son and her two young daughters. Their children are aged 17, 23, 27, 30 years old. Her eldest daughter lives with her partner. She had been the primary caregiver of her husband, who was diagnosed with cancer in the right eye when he was 60 years old, six months before starting the process of psychotherapy. She also suffered from controlled hypothy-roidism, showing symptoms such as debility, fatigue and drowsiness.
Instruments
Each of the cases was formulated with the case formulation model to validate, in which the following information is recorded: (a) demographic data, (b) the genogram, (c) the transcript of the motive of consultation expressed by the client, (d) descriptive analysis of the case, (e) biological conditions of the client (f) description and behaviors found in the contexts of operation, (g) competences of the consultant, (h) a description of the competences of self-knowledge and appreciation of the therapist in this regard: (i) facilitating resources of the therapeutic process; (j) consultants' degree of affectation of the problem, (k) formulation of hypotheses, (l) explanatory hypothesis, and (m) intervention plan.
Data collection was done by direct and indirect measures. Indirect measures included data reported in the medical record and in structured and open interviews; and direct measures involved a process of asking each participant to carry out a self-register, mostly anecdotal, which included their actions, thoughts and feelings, situations in which they arise and the people involved. These tools allowed to collect additional information from the reports made by the consultants and their families, and, thus, allowed validation of the data by information convergence, because it is important to assess the same event by different methods, determining the coincidence of the information provided (Iwata, & Dosi, 2008).
Procedure
In the seven cases analyzed in this study the same evaluation procedure was replicated, although the treatment phase of the procedure was carried out according to the formulation of the problems of each particular case, following the principles of behavior analysis and idiographic study. It is important to note that the objective of this research is not the clinical case study itself, only relevant clinical information of specific issues that were useful of the model are presented. This paper don't show specific qualities of the psychotherapeutic process.
Weekly sessions of one hour were carried out in the seven cases; each one depended on the availability of participants. When they could not attend, the meeting was rescheduled, and they were asked to continue the written self-record steadily. An initial baseline was conducted in all cases, in which the evaluation and data collection was made to make the functional analysis of target behaviors. Consultants and family members were both interviewed during this phase. Constant data was taken from the self-reports and behavior was observed during the session.
The following procedure took place during the evaluation sessions: (a) First, the conditions for research were explained and participants signed informed consent, (b) Data was collected and their medical history was explored (c) motive of consultation and expectations of the therapeutic process were asked for, (d) the problem behaviors were operationalized, (e) information that allows the covariation between behavior and contextual variables was investigated to perform functional analysis, (f) the effect of problem behaviors in different contexts regarding the operation and interaction with other elements of these contexts was explored, (g) questions were asked regarding the history of the participants that could be relevant for understanding the behavior problem, (h) and finally, when results an self-reports were collected and analyzed, the clients received feedback of the case formulation.
Following the above procedure, the intervention phase began, which involved the application of treatment. During this phase, the recollection of data regarding target behaviors was systematic and continuous, and thus worked on each case according to its particular objectives, as the idiographic approach is favored in behavior analysis. In the final phase, the therapeutic variable was removed, follow-up sessions were carried out and records were kept. Results and their maintenance were evaluated.
Results
Seven cases were formulated, four of which correspond to consultants with problems related to morbid obesity, and three with problems related to cancer diseases. Following the aim of the investigation, the results shown are relevant to the specific issue of replication of the formulation model, without developing the specific qualities of the psychotherapeutic intra-subject process.
It was considered appropriate in each case to present data by functional classes and not by topography, based on the principle that the change in functional class involves a change in the responses that constitute it. For data analysis, a time-series methodology was used, which allows to observe the changes in the level, trend and variability of the measurement unit, in relation with an independent variable (Hayes et al., 1999; Kazdin, 2001). The weekly rate was used as the unit of measurement, which corresponds to the relationship between behavior and appearance of the opportunity or occasion for it to be present.
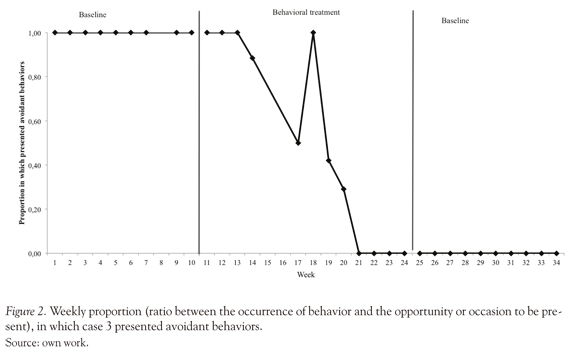
In case 1, the monitoring was 31 weeks long, in case 2, it was 10 weeks long, and in case 3 the monitoring was not possible because the client and her husband moved to another city. In cases 1, 2 and 3, following the introduction of the intervention that was designed based on the assumptions from data organized in model formulation, favorable changes were observed; since not only the rate at which functional classes presented problems decreased, but also this change was maintained during the follow-up weeks (see Figures 1, 2 and 3).
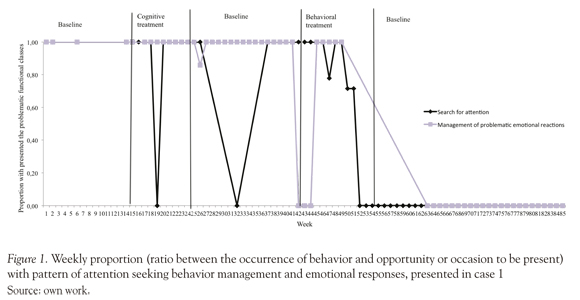
It is important to note that case 1 was initially formulated from a cognitive viewpoint. However, as shown in Figure 1, we observed that there were no significant changes in cognitive intervention, and in the withdrawal phase of the therapeutic variable, changes did not persist. That led to the reformulation of the case from a behavioral-analytical perspective, making this case in A-B-A-C-A design. Both the initial formulation, from a cognitive perspective, and the reformulation of the case from an analytic-behavioral perspective, were performed using the given formulation model. It was observed that the structure of the model allows to constantly update event information and to restructure it, to raise new explanatory hypotheses, and thus adjust the interventions to the particular conditions of the case in that moment.
In case 4, as shown in Figure 4, from the 7th week , the proportion of featured weekly avoidance or escape behaviors began to decrease. The case formulation allowed the generation of explanatory hypotheses, which accounted for the evolution of the functional relationship between the context and the behaviors of the consultant. This allows not only to understand the changes shown in Figure 4, but to predict the outcome when changes in context are observed.
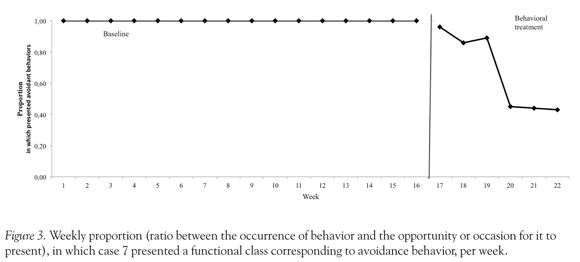
However, in cases 5, 6 and 7 the therapeutic goals were not achieved, because there was desertion. However, these results were predictable, as the explanatory hypothesis that resulted from the case formulation allowed to put into detail the behavioral characteristics of the consultants, and thus accounted for the implications of a behavioral change. In case 5, behavioral change meant losing access to positive reinforces, resulting in an increased cost of responding to his behavior. In case 6 the behavior change involved contact with aver-sive situations in the short term, but with appetitive long term effects; besides, he should have presented a longer behavioral chain, which implied a higher response cost in order to receive the same standard positive reinforcer. Finally, in case 7 the explanatory hypothesis, product of formulation, argued that in situations that would create an aggressive interaction with her husband, she would submit an avoidant behavior; so that when the husband gave the order of not to returning to therapy, she obeyed, thus avoiding aggression behavior from him.
It is noteworthy that the different categories in the formulation model (see Appendix A) allow a broader view of the cases, so that, for example, it was possible to understand the relationship of the disease and the motive for clinical consultation. In the condition of morbid obesity and cancer disease, the model's categories played an establishing operation role, by making it more likely to present challenging behaviors, and in turn decreasing the likelihood of present alternative and healthier behaviors.
Discussion
This research was performed aim to replicate the model of clinical formulation developed by the Psychology and Health Research Group of the Pontificia Universidad Javeriana, in health context, in order to determine their usefulness in different clinical problems in other clinical populations that haven't already been studied in previous research.
It followed a methodology in accordance with idiographic research, in which it is specified that, from a behavioral-analytic perspective, the ideal methodology correspond to the systematic replication of the previous studies (Barlow & Hersen, 1988; Sidman, 1960). In this case, this means to systematically replicate the use of the formulation model, which increases the likelihood of the data being reproducible in new cases, leading to a possible generalization of data (Goodwin, 2010; Hayes, Barlow, & Nelson-Gray, 1999; Johnston & Penny-packer, 1980; Kazdin, 2001; Leon & Montero, 2003; Mumma & Smith, 2001).
To demonstrate that the model is useful, based on idiographic perspective and in accordance with the principles of behavior analysis, it would expect to replicate the model used in new cases, with different characteristics from the cases of previous studies (Muñoz & Novoa-Gómez, 2010), the model retains its predictive and clinical validity. The internal, content and judges validity remains because the format of the model was not modified and was applied according to its instructions and specifications (See Appendix A).
To accomplish this task, we chose seven people whose reasons for consultation were related to health issues, and the clients were seen in the context of hospital outpatient care that referred them for psychological attention.
Now, as Santibanez, Roman, Chenevard, Espinoza, Irribarra, and Muller (2008) noted, there are nonspecific variables that are involved in psycho-therapeutic processes, and therefore, are beyond the researcher's or therapist's control. The cases studied in this investigation showed that there were nonspecific variables that were related to changes observed in consultants. However, it is important to note that different categories in the formulation model (see Appendix B) allow a larger view of the cases. So it was possible to integrate non-specific variables that had arisen, by adjusting the same information, and predicting the potential impact of these variables on the consultants' behavior.
Within these variables are the health-related processes, which could be elements that encourage changes in behavior of the consultants. For example, in cases with clinical condition of morbid obesity, a progressive increase of physical limitations was reported, as well as pain, motor and respiratory difficulties. In cases where the reasons for consultation were associated with a diagnosis of cancer, it was reported that they had to take the side effects of chemotherapy such as nausea, insomnia, etc.
These items increased the likelihood that the consultants presented problem behaviors such as isolation, aggression, constant complaints, avoidant behavior, attention seeking, among others; while diminishing the probability of healthy behaviors and access to other sources of reinforcement. Therefore it is conceivable that these secondary consequences of obesity, of disease, or of treatments for the disease, were aversive enough to generate a change across participants' behavioral repertoire, or to comply a function of establishment or abolition, which is consistent with the approach of Ribes (1990), Hackberg and Dougher (2000), as well as Michael (1993).
In addition to this, the consultants were under the constant attention of an interdisciplinary group, and in order to improve their health, they should have followed multiple directions and recommendations that each of the specialists gave. In addition to having to attend multiple visits and tests, and make changes in their daily lives in order to meet the various treatments indicated, all this meant a change in response instances belonging to the problematic functional classes.
So, from what is stated so far, it is clear that several nonspecific variables were related to changes observed in the consultants, which were beyond the control of the therapist. However, from the functional analysis and case formulation, it was possible to find functional relations governing the behavior of the consultants. To that extent, it was possible to propose effective interventions (cases 1, 2 and 3), to understand the changes generated by the variables involved in all cases, as well as to predict
desertion in cases 5, 6 and 7. This fact implies that the model is useful for predicting the behavior of the consultants, and therefore allows foreseeing the changes that arise in the conduct of consultants as a result of changes in context, or in the presence of non-specific variables. This supports the usefulness of the model.
In cases 1, 2 and 3, results show significant changes after the introduction of the medical treatment derived from the clinical formulation, which remained after the end of the intervention. It evidences that the formulation allowed planning an effective intervention, adjusted to each consultant, and results were maintained at follow-up.
On the other hand, the results show that the therapeutic efficacy or dropouts can be predicted from the principles of behavior analysis, through functional analysis and the case formulation. Three explanatory hypotheses, result of case formulation, allowed detailing the behavioral characteristics of the consultants, and, likewise, it accounted for what implied a change in behavior. Also, the different categories of the model allowed to accounting of the contextual elements that may hinder the psy-chotherapeutic process, leading to the prediction of dropout cases.
Besides the above, case 1 could demonstrate the flexibility of the model, since it was made from two different theoretical positions. This confirms the statement by Muñoz and Novoa-Gómez (2010), which states that the formulation model can be used by different cognitive-behavioral approaches, since it is not affiliated with any specific theoretical position. Therapists may include, within the formulation, items related to mediational and non-mediational positions, and may also adjust the assumptions and interventions to new information, the observed changes and the particularities of each case.
So, along the seven cases the predictive validity of the formulation model was maintained, both in successful cases and in those in which there were dropouts. This indicates that results are kept in regard to internal, clinical and predictive validity, as reported by previous research conducted by Cayce-do, Ballesteros and Novoa-Gómez (2008), Pachón and Novoa-Gómez (2009), as well as by Muñoz and Novoa-Gómez (2010). It is found that the model is useful within the health context.
During this study, both strengths and weaknesses were found, that lead to recognize the scope and limitations of this research. Among the strengths, one can conclude that results achieved have clinical significance, to the extent that coherent hypotheses were formulated; consistent with the principles of behavior analysis regarding the functional relations that characterized the problem behaviors of each participant. Likewise accomplish intervention objectives consistent with these hypotheses. Added to this, it is considered that the objective of the investigation was fulfilled, to the extent that there was a first approach of the application of the model in a population with health-related issues, maintaining consistency with the principles of idiographic research. It was found that the model was not only useful and applicable, but maintained its internal, clinical and predictive validity.
New questions arose about the relationship between dropout and treatment success with the use of a formulation model, since it would be safe to assume that the use of a formulation model would increase the likelihood of treatment success, and thus decrease the likelihood of attrition (Eells, Kendjelic, & Lucas, 1998; Haynes, Leisen, & Blaine, 1997; Hayes & Hass, 1988; Muñoz & Novoa-Gómez, 2010). It is considered important to conduct similar studies with changes at the sample size, population, conditions and environments, and to increase the follow-up after completion of the intervention; as well as specific studies to increase knowledge about the relationship between dropout and treatment success with the use of a formulation model. Such results will expand the generalizability of the findings.
Finally, it is important to note that this research has allowed to continue with the studies conducted by Caycedo, Ballesteros and Novoa (2008), Pachón and Novoa-Gómez (2009), as well as by Muñoz and Novoa-Gómez (2010), in the research work related with psychological well-being, showing the Psychology and Health Research Group's commitment to improve the quality of life of the consultants.
References
Ballesteros, B., Caycedo, C., & Novoa-Gómez, M. (in press) El bienestar psicológico en el marco del análisis del comportamiento. [ Links ]
Barlow, D., & Hersen, M. (1988). Diseños experimentales de caso único. Barcelona: Martínez Roca. (Original 1984) [ Links ]
Bergner, R. (1998). Characteristics of optimal clinical case formulations. American Journal of Psychotherapy, 52, 287-301. [ Links ]
Butler, G. (1998). Clinical Formulation. En A. S. Bel-lack., & M. Hersen (Eds.), Comprehensive Clinical Psychology (pp. 1-24). New York: Pergammon Press. [ Links ]
Carrascoso, F., & Valdivia, S. (2007). Towards alternative criteria for the validation of psychological treatments. International Journal of Psychology and Psychological Therapy, 7, 347-363. [ Links ]
Castro, L., & Angel, E. (1998). Formulación clínica con-ductual. En V. E. Caballo (Comp.), Manual para el tratamiento cognitivo-conductual de los trastornos psicológicos (Vol. 2; pp. 3-69). Madrid: Siglo XXI. [ Links ]
Catania, C. (2007). Learning. Interim (4a. Ed.) USA: Sloan Publishing [ Links ]
Caycedo, C., Ballesteros, B., & Novoa-Gómez, M. (2008). Análisis de un protocolo de formulación de caso clínico desde las categorías de bienestar psicológico. Universitas Psicológica, 7(1). 231-250. [ Links ]
Charmaz, K. (2005). Grounded theory in the 21st Century. En N.K. Denzin., & Y.S. Lincoln, The Sage Handbook of Qualitative Research (pp. 507-535). Thousand Oaks: SAGE. [ Links ]
Cumming, G., & Maillardet, R. (2006) Confidence intervals and replication: where will the next mean fall?. Psychological methods. 11 (3). 216-227 [ Links ]
De la Torre, G., Di Carlo, E., Florido, A., Opazo, H., Ramirez, C., Rodríguez, P., Sánchez, A., & Tirado, J. (2005). Teoría Fundamentada o Grounded Theory. Obtenido en Enero 13, 2012, de http://www.uacj.mx/DINNOVA/Documents/SABERES_Verano2011/curso_ti/Teoria-Fundamentada_(trabajo).pdf [ Links ]
Dougher, M., & Hackberg, L. (2000). Establishing operations, cognitions, and emotions. The Behavior Analyst, 23, 11-24. [ Links ]
Eells, T. (2001). Update on psychotherapy case formulation research. The Journal of Psychotherapy Practice and Research. 10, 277-281. [ Links ]
Eells, T., Kendjelic, E., & Lucas, C. (1998). What's in a case formulation? Development and use of a content coding manual. The Journal of Psychotherapy Practice and Research. 7(2). 144-156. [ Links ]
Ferro, R., & Vives M.C. (2004) Un análisis de los conceptos de efectividad, eficacia y eficiencia en psicología. Tremédica, 5 (16). 97-99. Obtenido en Julio 25, 2011, de http://tremedica.org/panacea.html [ Links ]
Goodwin, C. (2010) Research in psychology. Methods and design (6a. Ed., pp. 186 - 191) Washington: Wiley. [ Links ]
Hayes, S. C., Barlow, D. H., & Nelson-Gray, R. O. (1999). The scientist practitioner: Research and accountability in the age of managed care (2nd Ed.). Boston: Allyn and Bacon. [ Links ]
Hayes, S., & Haas, J. (1988). A reevaluation of the concept of clinical significance: goals, methods, and methodology. Behavioral Assessment. 10, 189-196. [ Links ]
Haynes, S., Leisen, M., & Blaine, D. (1997). Design of individualized behavioral treatment programs using functional analytic clinical case models. Psychological Assessment. 9. 334-348. [ Links ]
Haynes, S., Mumma, GH., & Pinson, C. (2009) Idio-graphic assessment: conceptual and psychometric foundations of individualized behavioral assessment. Clinical Psychology Review, 29, 179-191 [ Links ]
Haynes, S., & Williams, A. (2003) Case formulation and design of behavioral treatment programs: Matching Treatment Mechanism to Causal Variables for Behavior Problems. European Journal of Psychological Assesment, 19 (3), 164-174 [ Links ]
Horowitz, L., Rosemberg, S., Ureño, G., Kalehzan, M., & O'Halloran, P. (1989). Psychodinamic Formulation, Consensual Response Method, and Interpersonal Problems. Journal of Consulting and Clinical Psychology, 57 (5), 599-606. [ Links ]
Iwata, B., & Dosier, C. (2008). Clinical application of functional analysis methodology. Behavior Analysis in Practice. 1, 3-9 [ Links ]
Iwata, B., & Worsdell, A. (2005). Implications of functional analysis methodology for the design of intervention programs. Exceptionality. 13. 25-35. [ Links ]
Jameson, P., Stadter, M., & Poulton, J. (2007). Sustained and sustaining continuing education for therapists. Psychotherapy: Theory, Research, Practice, Training. 44(1), 110-114. [ Links ]
Johnston, J., & Pennypacker, H. S. (1980) Strategies and tactics of human behavioral research. Erlbaum Associates, Hillsdale: N.J. [ Links ]
Kahneman, D., & Klein, G. (2009). Conditions for intuitive expertise a failure to disagree. American Psychologist, 64, 515-526. [ Links ]
Kanter, J., Tsai, M., & Kohlenberg, R. (2010).The Practice of Functional Analytic Psychotherapy. New York: Springer [ Links ]
Kazdin, A. (2001) Métodos de investigación en psicología clínica (3a. Ed., pp. 26 - 27) México: Prentice Hall. [ Links ]
León, O., & Montero, I. (2003) Métodos de investigación en psicología y educación (3â. Ed., pp. 26-27) Madrid: McGraw Hill. [ Links ]
Mañas, I. (2006). Nuevas terapias psicológicas: la tercera ola de terapias de conducta o terapias de tercera generación. Gaceta de psicología, 40, 26-34 [ Links ]
Michael, J. (1993). Establishing operations. The Behavior Analyst, 16, 191-206. [ Links ]
Michael, J (2004) Concepts and principles of behavior analysis.Kalamazoo, MI: SABA [ Links ]
Mumma, G., & Smith, J. (2001). Cognitive-Behavioral-Interpersonal scenarios: interformulator reliability and convergent validity. Journal of psychophatol-ogy and behavioral assessment. 23, 203-221. [ Links ]
Muñoz, A., & Novoa-Gómez, M. (2010). Confiabilidad y validación de un modelo de formulación clínica conductual. Universitas Psicológica, 10 (2). 501-519. [ Links ]
Muñoz, J. (2005) Análisis cualitativo de datos textuales con ATLAS.ti 5. Documento de libre distribución, obtenido en Junio 25, 2011, de http://unorte.edu.uy/ccss/mtubio/Atlas5.pdf. [ Links ]
Nezu, A., Nezu, C., & Lombardo, E. (2004). Cognitive case-formulation and treatment design. A problem solving approach. New York: Springer Publishing Company, Inc. [ Links ]
Pachón, G., & Novoa-Gómez, M. (2009). Validación de un protocolo de formulación de caso clínico desde la perspectiva del análisis del comportamiento. Tesis para acceder al título de psicólogo. Pontificia Universidad Javeriana. Documento inédito. [ Links ]
Perry, S., Cooper, A., & Michels, R. (1987). The Psychodinamyc Formulation: Its Purpose, Structure, and Clinical Application. American Journal of Psychiatry, 144, 543-550. [ Links ]
Persons, J. (1991). Cognitive Therapy in Practice: The Case Formulation Approach. New York: Norton. [ Links ]
Ribes, E. (1990) Psicología y salud. Un análisis conceptual. Mexico: Trillas. [ Links ]
Santibáñez, P., Román, M., Chenevard, C., Espinoza, A., Irribarra, D., & Müller, P. (2008) Variables inespecíficas en psicoterapia. Terapia psicológica. 26 (1), 89-98. [ Links ]
Sidman, M. (1960) Tactics of Scientific Research. New York: Basic Books, Inc. [ Links ]
Sturmey, P. (2008). Behavioral Assessment: Behavioral Case Formulation and Intervention. A Functional Analytic Approach (pp. 225-258). West Sussex: Wiley - Blackwell. [ Links ]
Tarrier, N. (2006). Case Formulation in Cognitive Behaviour Therapy: The Treatment of Challenging and Complex Cases. London: Routledge. [ Links ]
Tsai, M., Kohlenberg, R., Kanter, J., Kohlenberg, B., Follete, C., & Callaghan, G. (2009). A Guide to Functional Analytic Psychotherapy. Awareness, Courage, Love and Behaviorism. New York: Springer [ Links ]
Tukey, J. W. (1969). Analyzing data: Sanctification or detective work? American Psychologist, 24, 83-91. [ Links ]
Vallejo, M. (2007). El Mindfulness y la "tercera generación de terapias psicológicas". Consejo general de colegios oficiales de psicólogos - INFOCOP, 33, 16-18 [ Links ]
APPENDIX
B APPENDIX
CLINICAL BEHAVIORAL FORMULATION MODEL
SOCIODEMOGRAPHIC DATA
GENOGRAM
TRANSCRIPT OF THE MOTIVE OF CONSULTATION AS EXPRESSED BY THE CONSULTANT:
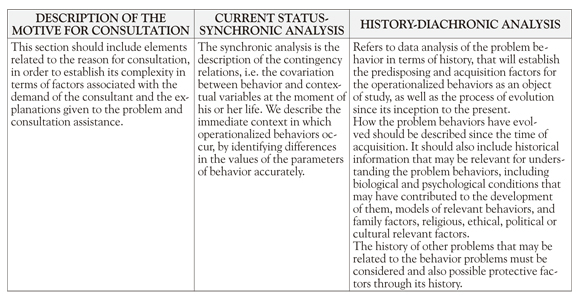
DESCRIPTIVE ANALYSIS OF CLINICAL CASE:
The first step includes a description of client problem, history and functional areas on which hypotheses will be formulated for acquisition, disposition and maintenance. These guide the process to develop clinical judgments that allow the identification of the unit of analysis.
BIOLOGICAL CONDITIONS OF / THE CONSULTANT: DESCRIBE THE TYPE OF RELATIONSHIP BETWEEN THE CONDITIONS AND THE BEHAVIOR
Describe biological condition of the person, historical and present, that relate in some way with the personal, social, academic, labor and sexual function and problems.
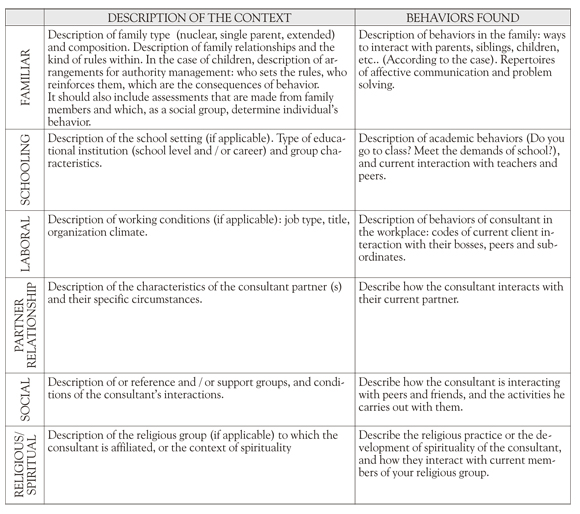
FUNCTIONING CONTEXTS
Functioning context is referred to the set of circumstances of time, place and people who demand specific behaviors of a person. Listed below are the most common contexts for most people. However, if the clinician identifies other contexts, they must be included.
SKILLS
A skill is a set of behaviors that are adjusted (are effective) in relation to established criteria. A competency usually includes behaviors of different morphologies that are effective when they personally or socially fit. This section is also important to identify when the behavior is not effective.
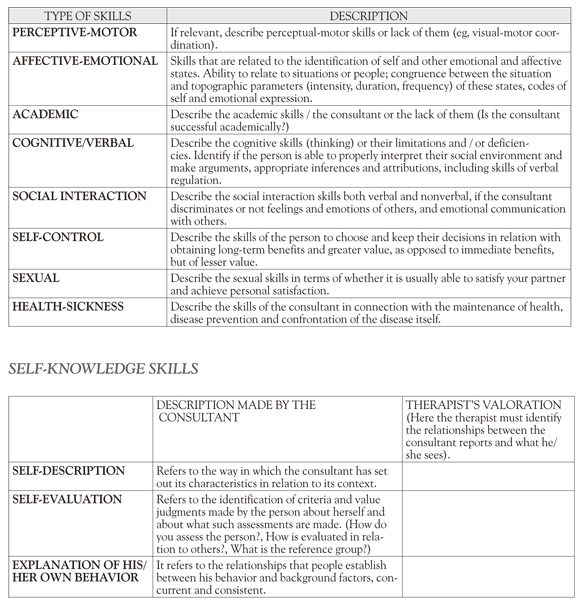
FACILITATING RESOURCES FOR THE THERAPEUTIC PROCESS
They refer to the contextual and consultant resources that can lessen the impact of the problems or modulate the therapeutic process. This section does not repeat the information described above, but is a summary of such contexts
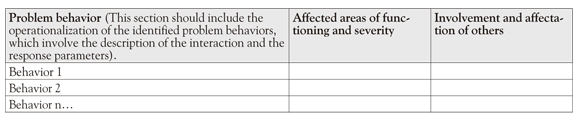
DEGREE OF INVOLVEMENT IN THE PROBLEM
This involves defining a clear, precise and specific severity of the consultant's problem, identifying how behaviors affect their performance in different areas of his/her life, and how those behaviors affect other people.
HYPOTHESES FORMULATION
Propose the hypotheses that have been developed so far, regarding relationships between issues considered, possible causes, the data that verifies or falsifies the hypotheses, scientific literature about the problem and other sources of hypotheses and / or verification of stock.
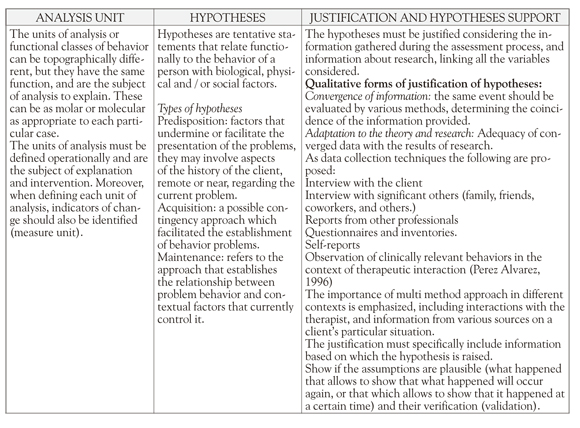
EXPLANATORY HYPOTHESES
This hypothesis summarizes and organizes all relevant information to understand the case and direct intervention. Integrates all hypotheses that have been validated and clarifies the role of behavioral and contextual variables. It is proposed to maintain internal consistency and logical relationship with the descriptive analysis, explaining the development or evolution of the problem, and specifically the factors and processes responsible for maintaining it at the moment in life of the person or group. Make sure there is enough empirical evidence for psychological processes and to sustain the explanatory variables that are formulated.
INTERVENTION PLAN
The plan should address the priorities identified and the issues raised in the explanatory hypothesis. Designing the plan, the characteristics of the client should be considered, in terms of his/her process, and factors and repertoires that may increase the likelihood of success or failure of the intervention, the environmental and social group that may be affected by this and information on intervention strategies that have proven most effective in similar situations, in order to conduct a cost-benefit analysis to ensure the best intervention for the client.