










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkUniversitas Psychologica
versión impresa ISSN 1657-9267
Univ. Psychol. vol.13 no.4 Bogotá oct./dic. 2014
https://doi.org/10.11144/Javeriana.UPSY13-4.igcd
Is there a Grammatical Comprehension Deficit in Multidomain Mild Cognitive Impairment?*
¿Hay un déficit de comprensión gramatical en el Deterioro Cognitivo Leve multidominio?
Ramón López-Higes**
José María Prados***
Universidad Complutense de Madrid, España
Pedro Montejo****
Mercedes Montenegro*****
Montserrat Lozano******
Centro de Prevención del Deterioro Cognitivo, Madrid, España
*Este estudio ha sido posible gracias al proyecto de investigación PSI2012-38375-C03-03, financiado por el Ministerio de Economía y Competitividad del Gobierno de España.
**Departamento de Psicología Básica II (Procesos cognitivos). Facultad de Psicología. Director del Departamento de Psicología Básica II. E-mail: rlopezsa@psi.ucm.es
***Departamento de Psicología Basica II. Profesor de la Sección departamental de Psicología Básica II en la Facultad de Trabajo Social de la UCM. Email: jprados2@hotmail.com
**** Director del Centro de Prevención del Deterioro Cognitivo (CPDC). Madrid Salud. Ayuntamiento de Madrid. Madrid Salud. Ayuntamiento de Madrid. E-mail: montejop@munimadrid.es
*****Psicóloga del CPDC. Profesora asociada del Departamento de Psicología Básica I en la UCM. E-mail: montenegropmm@munimadrid.es
******Auxiliar Técnico Sanitario del CPDC. E-mail: mlozano@munimadrid.es
Recibido: junio 6 de 2013 | Revisado: abril 18 de 2014 | Aceptado: abril 18 de 2014
Para citar este artículo
López-Higes, R., Prados, J. M., Montejo, P., Montenegro, M., & Lozano, M. (2014). Is there a grammatical comprehension deficit in Multidomain Mild Cognitive Impairment? Universitas Psychologica, 13(4), 1569-1579. http://dx.doi.org/10.11144/Javeriana.UPSY13-4.igcd
Abstract
Multidomain mild Cognitive Impairment (mMCI) patients have similar difficulties than those observed in the initial stages of Alzheimer disease. Many studies have explored language abilities in MCI, but few have focused in grammatical comprehension. This study explores the differences between mMCI patients and controls using a complete neuropsychological battery, it tries to find out if vocabulary and grammatical comprehension in both groups are predicted by naming and verbal fluency, and seeks the best subset of sentence structures to classify the subjects. There were significative differences between groups in verbs and in grammatical comprehension. Linear regression revealed that verb and sentence comprehension are independent of naming and verbal fluency performance in mMCI patients. In the control group verb comprehension is predicted by intrusions in verbal fluency, and the comprehension of sentences containing two propositions seems to be related to control processes and recognition errors. Two sentence structures, that do not fit to syntactic canonical order in Spanish, are especially useful for subjects' classification. mMCI patients have a specific deficit affecting grammatical comprehension that doesn't seem to depend on their low performance at lexical-semantic level. In healthy elders, verb and grammatical comprehension are related to control processes.
Keywords :Mild cognitive impairment; healthy elders; grammatical comprehension; vocabulary; naming; verbal fluency
Resumen
Pacientes con Deterioro Cognitivo Leve Multidominio (DCLm) tienen dificultades similares a las observadas en las etapas iniciales de la enfermedad de Alzheimer. Algunos estudios han explorado las habilidades lingüísticas en pacientes con DCLm, pero pocos se han centrado en la comprensión gramatical. Este estudio explora las diferencias entre pacientes con DCLm y controles. Utilizando una batería neuropsicológica completa, tratamos de determinar si la denominación y la fluidez verbal predicen los resultados en vocabulario y comprensión gramatical en ambos grupos, y buscamos el mejor subconjunto de estructuras oracionales para clasificar a los sujetos. Se encontraron diferencias significativas entre los grupos en la comprensión de verbos y de oraciones. La regresión lineal reveló que la comprensión de verbos y de oraciones son independientes del rendimiento en denominación y en fluidez verbal en pacientes con DCLm. En el grupo control, la comprensión de verbos fue pronosticada por el número de intrusiones en la tarea de fluidez verbal, mientras que la comprensión de oraciones con dos proposiciones parece estar relacionada con procesos de control y errores de reconocimiento. Dos tipos de oraciones no ajustadas al orden sintáctico canónico del español resultaron especialmente útiles para la clasificación de los sujetos. Los pacientes con DCLm presentan un déficit específico que afecta la comprensión gramatical que no parece depender de su bajo rendimiento en el nivel léxico-semántico. En los ancianos sanos, tanto la comprensión de verbos como la de oraciones se relacionan con los procesos de control.
Palabras clave :deterioro cognitivo leve; ancianos sanos; comprensión gramatical; vocabulario; nombrar; fluidez verbal
Mild Cognitive Impairment (MCI) is actually defined as a sustained decrease of cognitive functions that is insufficiently severe to warrant a diagnosis of dementia (Montenegro, Montejo, Llanero, & Reinoso, 2012; Petersen, 2011; Petersen et al., 2009). Three subtypes of MCI have been recognised, each with a different evolution (Mulet et al., 2005): amnestic MCI (aMCI), multiple-domain MCI (mMCI), and single MCI.
Initially the definition of MCI focused exclusively on memory and its model was the Alzheimer Disease ([AD]; Petersen et al., 1999). Thus, studies of memory in MCI have dominated the research in this area for decades. In the decade of 90s there appeared definitions of MCI focused not only in memory but also referring to the decline of other domains, such as language and executive functions (Petersen et al., 2001).
MCI is a syndrome susceptible of evolution so it is possible to argue that cognitive impairment associated with it can vary over time, thus affecting not only memory, but gradually also attention, executive functions, or language (Sperling et al., 2011). From this perspective mMCI would be a subtype of cognitive impairment closer to dementia than other subtypes, in fact some authors cast doubts upon the usefulness of the concept of multiple-domain aMCI as distinct from early stage of AD (Ahmed, Mitchell, Arnold, Nestor, & Hodges, 2008). Thus, mMCI patients with memory and language impairments would have similar difficulties than those observed in the initial stages of AD (Alexopoulos, Grimmer, Perneczky, Domes, & Kurz, 2006; Taler & Phillips, 2008).
Language deterioration in AD is well documented (see Taler & Phillips, 2008). Initial symptoms in typical AD are loss of episodic memory (difficulty in learning and retaining new information), alterations in naming (anomia) and in semantic memory. In early stages of AD the difficulties in naming are associated with degradation in lexical-semantic networks caused by atrophy of the left temporal cortex (Grossman et al., 2004). In mild to moderate stages patients can be read aloud without understanding what they read (using the link between the orthographic lexicon and the phonological lexicon). As the disease progresses the destruction of temporo-parietal areas of the left hemisphere produces aphasic disorders: problems of syntactic and discourse comprehension, semantic paraphasias and paragrammatism in production. In the later stages of the disease an almost complete absence of language and communication (global aphasia) is observed, and patients completely lose the ability to read.
Language skills that have been studied most often in MCI patients are: verbal memory, verbal fluency and naming (Juncos, Pereiro, Facal, & Rodrígez, 2010). However, studies of grammatical comprehension in MCI are relatively scarce. For example, Lambon, Patterson, Graham, Dawson, and Hodges (2003) found differences between MCI patients and control subjects only in the Token Test, but not in the Test of Reception of Grammar. Ribeiro, Mendoza, and Guerreiro (2006) also found significant differences between subjects with MCI and controls in the Token Test. Other studies have found no differences between subjects with MCI and controls in these tests (Hodges, Erzinclioglu, & Patterson, 2006), so that the possible existence of a deficit in comprehension at the syntactic level in patients with MCI is still an open question.
A brief subtest, adapted to the elderly population, which explores the grammatical comprehension of a wide variety of sentences with different syntactic structures can be found in ECCO_Senior (Exploración Cognitiva de la Comprensión de Oraciones; López-Higes, Rubio, Martín, Del Río, & Mejuto, 2012). Additionally, to rule out or to confirm wheter the difficulties in sentence comprehension stem from lexical problems, the test includes a vocabulary task.
The present study has the following specific objectives:
(1) To explore the differences between healthy elders and mMCI patients (with objetive memory and language impairments) in a battery of neu-rospychological tests and also in vocabulary and sentence comprehension.
(2) To analyze if the results obtained by each group on vocabulary and grammatical comprehension are predicted by the level of performance shown in a standard naming and in verbal fluency tasks.
(3) A final goal of the study is to determine which is the best subset of sentences in the grammatical comprehension subtest in order to classify subjects in the two groups previously mentioned.
Method
Participants
A total of 46 older adults were asigned to one of two groups according to their clinical profile: (1) control elders, nl = 27, mean age 73.59 years (SD = 3.18), 70.4% females; and (2) mMCI patients, n2 = 19, mean age 75.21 years (SD = 3.54), 58% females. There were no statistically significant differences between groups in age (Mann-Whitney U = 182, p = 0.095). All subjects had an elementary school level (beetween 1 and 8 years of formal education) and normal or corrected hearing and vision. All of them came to the Center for Prevention of Cognitive Impairment (CPCI) of Madrid. An experienced psychiatrist or psychologist interviewed all participants.
Inclusion criteria used for selection of seniors in the control group were: (a) Global Deterioration Scale (GDS) ≤ 2 (Reisberg, Ferris, de Leon, & Crook, 1982); (b) Mini-Mental State Exam (MMSE) > 26 (Folstein, Folstein, & McHugh, 1975); (c) Normal score (equal or greater than percentile 50) in WMS III Word List delayed recall (spanish adaptation: Weschler, 1997/2004); (d) Normal score in the Boston Naming Test ([BNT]; Kaplan, Goodglass, & Weintraub, 1978; Goodglas & Kaplan, 1996): equal or greater than 41, according to the normative study of Rami et al. (2008) for age and school level matched healthy elders. They did not meet the criteria for MCI and had no history of psychiatric or neurological disorders.
The diagnosis of mMCI was established following these criteria: (a) Memory complaints corroborated by an informant and the center's professional judgment; (b) Activities of daily living sufficiently preserved: Functional Assessment Scale (FAQ) < 6 (spanish version: Olazarán, Mouronte, & Bermejo, 2005); (c) Not fulfilling criteria for dementia; (d) Number of words recalled at or below percentile 30 in WMS-III Word List delayed recall: equal or below 2 words for subjects between 66 and 73 years old, or equal to 1 or 0 for elders having 74 or more years; (f) BNT scores 1.5 SD units below the mean corresponding to age and school level matched controls (equal or below 40, according to Rami et al., 2008).
Materials
To explore the cognitive status of all participants a complete neuropsychological assessment battery was administered. This included the MMSE, the 7-Minutes Screen Test (7-M in advance; Del Ser et al., 2004), various subtests of the WMS-III, including Word List, Orientation and Digits, the BNT, and two verbal fluency tasks, phonological (FAS test) and semantic (fruits and animals). An additional fluency task, with personal first names as evocation criteria, was also used, since such of names seem to be free of socio-educational influences (Saez-Zea, Carnero, & Gurpegui, 2008).
Regarding to the BNT three measures were obtained: the overall score and the score with semantic and phonological key, respectively. In the verbal fluency tasks the following measures were collected: the number of words evoked, the number of intrusions, and the number of perseverations.
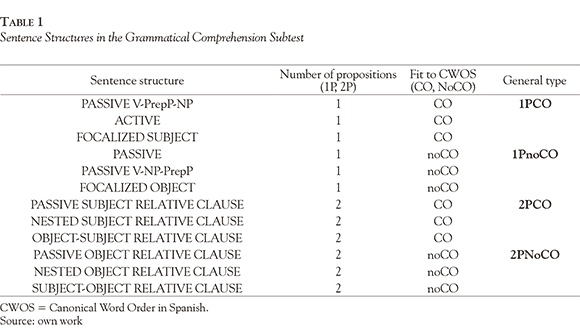
To assess the grammatical comprehension of all participants we used the sentence comprehension subtests of the ECCO_Senior Test. This is a simple verification task with 36 sentence-picture pairs that can be grouped into 12 types of sentence structures (see Table 1).
As a primary measure, in sentence comprehension subtest, the number of correct responses to each of the 12 types of sentences was obtained.
The vocabulary subtest is a written word-picture matching task containing 15 nouns, eight noun + adjective combinations and 16 verbs. With respect to the vocabulary subtest. The analyses include three indexes: total number of correct responses for nouns, for adjective + noun combinations and for verbs.
Procedure
Trained and specialized staff members from the CPCI conducted the assessment in two sessions. The entire neuropsychological battery was administered in two sessions. Neuropsychological tests were administered to the subjects following the standard instructions provided in the users' manuals.
The application of the sentence comprehension subtest began with five examples where adecuate feedback was provided to the subject. In a trial, each pair sentence-picture appeared on the screen until the subject responded "True" or "False", then a new item appeared on the screen. This procedure was repeated until the end of the test. During application no feedback was provided.
In the vocabulary subtest subjects' task was to point out the correct picture corresponding to the word (noun, noun + adjective or verb). The application of the subtest began with five examples in which adequate feedback was provided to participants.
Statistical analysis
Results obtained in the 12 sentence structure types in the comprehension subtest were transformed into four general categories that orthogonally combined two factors, as shown in Table 1. The number of correct responses in these four categories was as measures of grammatical comprehension.
All the statistical analysis was performed using SPSS 15.0. Regarding the first goal of the study descriptive analyses and non-parametrical mean comparisons between groups (Mann-Whitney U) were performed for all the neuropsychological test and ECCO_Senior subtests.
Pearson correlations for the entire sample, and then by groups, were calculated trying to discover the pattern of relationships between a working memory index (inverse order digit span) and sentence comprehension measures.
Linear regression analyses following the Enter method were performed to explore if BNT and verbal fluency predicted the results obtained by each group on grammatical comprehension and vocabulary, which was the second main objetive of the study.
Finally, to satisfy the third goal, a logistic regression analysis (following Wald forward step method) was performed in order to find out what sentence structures had a greater weight, and classify allow inter-group discrimination.
Results
Descriptive Analyses and Comparisons between Groups
Table 2 shows the descriptives of the two groups in all neuropsychological tests used in the study, as well as the U statistic for between-group comparisons and its significance.
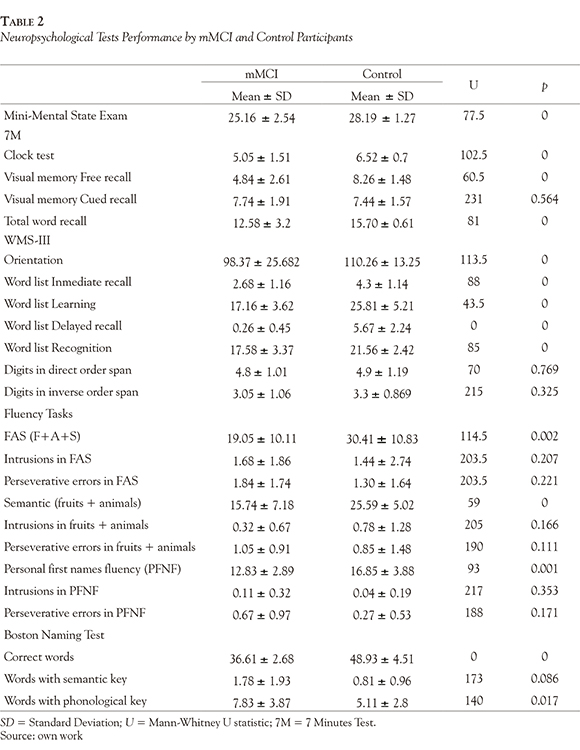
mMCI patients showed a significative lower performance than control elders in all the WMS-III Word List subtests, in all verbal fluency tasks, in spontaneous responses and responses with phonological key to BNT; as well as in MMSE, Orientation, Clock Test, Visual Memory Free Recall, and in the total word recall in 7-M.
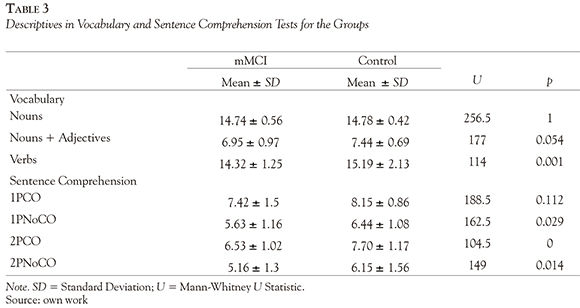
Table 3 shows the corresponding descriptives for vocabulary and sentence comprehension in both groups, together with the result of mean comparisons and its significance. The mMCI group had a significative lower performance in verb comprehension and in the following sentence types: 1PNoCO, 2PCO and 2PnoCO .
We also attempted to find out if there was a relationship between a measure related to working memory (digits in inverse order span) and the level reached on the four general types of sentences. Correlations between these variables were calculated for the entire sample, as well as for the two groups, independently. Only in the analysis of the entire sample a positive correlation between the working memory span measure and 1PnoCO reached significance (r = 0.308, p < 0.04). Correlations between variables were higher in the mMCI group than in the control group, all above 0.240. In mMCI group 73.7% of cases had a span between 2 and 3, while in the control group this percentage decreased to 59.3%.
Prediction of Vocabulary and Sentence Comprehension by Naming and Verbal Fluency Performance
Variables chosen for the regression analyses were those in which significant differences were found between groups (verbs, 1PNoCO, 2PCO, and 2Pno-CO). The following predictor variables were included: global score on FAS, total of intrusions in FAS, total of FAS perseverative errors, overall score in semantic verbal fluency (SVF), intrusions in SVF, perseverative errors in SVF, semantic fluency for personal first names (SFPFN), intrusions in SFPFN, perseverative errors in SFPFN, BNT overall score, BNT score with semantic key, and BNT score with phonological key.
First we performed linear regression analyses by selecting only patients within the mMCI group. None of the aforementioned predictor variables entered into the regression equations performed for each of the four dependent variables selected.
The analyses performed for the control group showed that intrusions in FAS and in the semantic fluency task explained 56.3% of the variance of the subject's total score in verb comprehension. Both the global score on FAS, and the number of responses with semantic key on BNT explained 51% of the variance of the subject's total score on 2PCO type of sentences. Additionally, the analyses revealed that intrusions in the semantic fluency task explained only 8.6% of the variance of the subject's total score on 1PNoCO sentences, and also that overall score on FAS and intrusions both on semantic and on personal first names fluency tasks explained 32.1% of the variance 2PnoCO sentences.
What is the Best Subset of Sentence Structures in Order to Classify the Subjects?
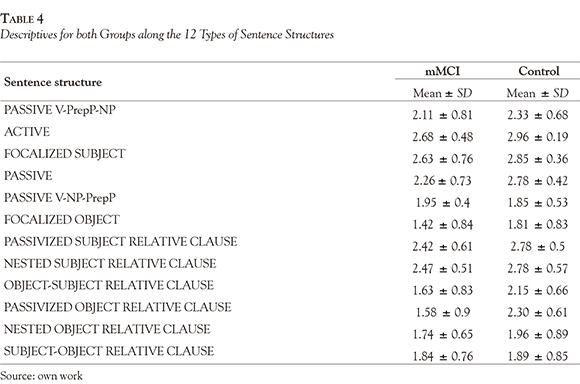
Logistic regression analysis was performed to check what sentence structures have a greater weight, in order to classify subjects in one of the two groups previously mentioned. Table 4 showed the descriptives for each sentence structure in the comprehension test for both groups.
The two sentence structures included in the final equation and the corresponding statistics (weights, statistical significance, odds ratio and confidence interval) are shown in Table 5. Passive sentences had the highest weight as discriminant variable in the equation, and also had the higher odds ratio (Exp_(B)); it means that a person having a bad performance in this type of sentences will have 3.5 times more probability to have MCI than normal than their control peers. An analog interpretation should be derived for Passivized Object Relative Clause structures.
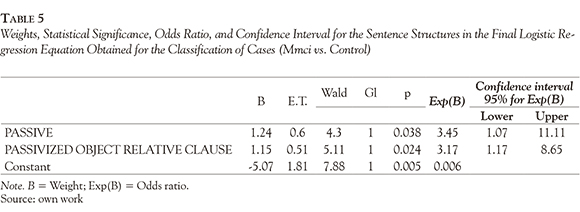
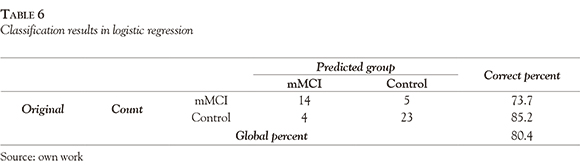
The final logistic equation classified 80.4% of the cases (see Table 6).
Discussion
Beyond the differences found between both groups in neuropsychological tests, and regarding the first objective of this study, the analyses have shown that mMCI patients had worse performance on verbs than controls and also presented less variability.
The lowest results in grammatical comprehension test corresponded always to the sentences not fitted to CWOS, whatever the group considered. It seems that grammatical comprehension is more negatively affected by syntactic order of constituents than it is by the number of propositions. This result would be in line with other similar studies (Wingfield, McCoy, Peelle, Tun, & Cox, 2006).
On the other hand, the worst performance in all sentence types was observed in the mMCI group, which also showed a comprehension mean near to chance level in one sentence that do not fit to CWOS (2PnoCO). Only in one of the sentence types (the less complex, 1PCO) the difference with the control group did not reach statistical significance.
Because of its close relationship with sentence comprehension (Christianson, Williams, Zacks, & Ferreira, 2006; Just & Varma, 2002) we explored whether there was a relationship between a measure of working memory (WM) span and the subjects' performance with the four general sentence types. Correlation analysis in each group revealed that in this case there appears not to be a significant relationship between the subjects' WM and their sentence comprehension skills. In mMCI patients the correlations between variables were higher than in the control group. Only in the overall analysis a positive correlation between the WM span and 1PnoCO reached significance. One possible explanation for this pattern of results is that there was little variability between subjects in each group in the WM span measure. Another issue that must be taken into account is that the simple verification task used to assess grammatical comprehension demands few memory resources.
Regarding the second aim of the study, analyses revealed that the observed verb and grammatical comprehension difficulties (especially in sentences not fitted to CWOS) in mMCI patients are independent to their naming and verbal fluency abilities. This conclusion might be in tune with other similar studies (Lambon et al., 2003; Ribeiro et al., 2006), which had pointed out the possible existence of a specific deficit in grammatical comprehension in MCI and initial AD patients.
By contrast, in the control group the regression analyses allow to conclude that there is a direct relationship between verb and 2PnoCO sentence type comprehension and the existence of problems of inhibition and/or mental flexibility. That is why intrusions in a verbal fluency task (phonological or semantic) indicate failures in inhibitory control and/or lack of mental flexibility (Traykov et al., 2007). In this group the results on FAS and the responses with semantic key on BNT also explained a significative percentage of the variance (51%) associated to 2PCO comprehension. It is well known that performance in phonological verbal fluency tasks depend both on the integrity of phonological representation, as well as on links between them and the corresponding lexical representations. In this task processes of control that would include update and inhibition intervene, as well as strategies of search and recovery (Lanting, Haugrud, & Crossley, 2009). On the hand, when an examiner offers a semantic key in BNT application he/she is trying to verify if the subject has committed a mistake in picture recognition. Thus, problems in control processes or perceptual difficulties are plausible factors affecting subjects' performance in 2PCO sentence type comprehension.
Logistic regression results showed that Passive and Passivized Object Relative Clause sentence structures served to correctly classify 80.4% of the cases. Classification results were better for the control group, but reached an acceptable percentage in mMCI group. Both are sentence structures not fitted to CWOS, and it is expected that they are more resource demanding for all subjects (Wing-field et al., 2006).
It is therefore necessary to conduct further studies with larger samples of patients and control subjects in order to confirm if there is a specific deficit in grammatical comprehension in mMCI patients.
References
Ahmed, S., Mitchell, J., Arnold, R., Nestor, P. J., & Hodges, J. R. (2008). Predicting rapid clinical progression in amnestic Mild Cognitive Impairment. Dementia and Geriatric Cognitive Disorders, 25(2), 170-177. [ Links ]
Alexopoulos, P., Grimmer, T., Perneczky, R., Domes, G., & Kurz, A. (2006). Progression to dementia in clinical subtypes of mild cognitive impairment. Dementia and Geriatric Cognitive Disorders, 22(1), 27-34. [ Links ]
Christianson, K., Williams, C. C., Zacks, R. T., & Ferreira, F. (2006). Younger and older adults' "good-enough" interpretations of garden-path sentences. Discourse Processes, 42(2), 205-238. [ Links ]
Del Ser, T., Sánchez, F., García de Yébenes, M. J., Otero, A., Zunzunegui, M. V., & Muñoz, D. G. (2004). Versión española del Test de los Siete Minutos. Datos normativos de una muestra poblacional de ancianos de más de 70 años. Neurología, 19(7),344-358. [ Links ]
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research,, 12(3), 189-198. [ Links ]
Grossman, M., McMillan, C., Moore, P., Ding, L.,Glosser, G., Work, M., & Gee, J. (2004). What's in a name: Voxel-based morphometric analyses of MRI and naming difficulty in alzheimer's disease, frontotemporal dementia and corticobasal degeneration. Brain: A Journal of Neurology, 127(3), 628-649. [ Links ]
Hodges, J. R., Erzinclioglu, S., & Patterson, K. (2006). Evolution of cognitive deficits and conversion to dementia in patients with mild cognitive impairment: A very long-term follow-up study. Dementia and Geriatric Cognitive Disorders, 21 (5-6), 380-391. [ Links ]
Juncos-Rabadán, O., Pereiro, A. X., Facal, D., & Rodríguez, N. (2010). Una revisión de la investigación sobre lenguaje en el deterioro cognitivo leve. Revista de Logopedia, Foniatría y Audiología, 30(2), 73-83. [ Links ]
Just, M. A., & Varma, S. (2002). A hybrid architecture for working memory: Reply to MacDonald and Christiansen (2002). Psychological Review, 109(1), 55-65. [ Links ]
Kaplan, E. F., Goodglass, H., & Weintraub, S. (1978). The Boston Naming Test. Philadelphia: Lea & Febiger. [ Links ]
Lambon, M. A., Patterson, K., Graham, N., Dawson, K., & Hodges, J. R. (2003). Homogeneity and heterogeneity in mild cognitive impairment and Alzheimer's disease: A cross-sectional and longitudinal study of 55 cases. Brain, 126(11), 2350-2362. [ Links ]
Lanting, S., Haugrud, N., & Crossley, M. (2009). The effects of age and sex on clustering and switching during speeded verbal fluency tasks. Journal of the International Neuropsychological Society, 15(2), 196-204. [ Links ]
López-Higes, R., Rubio, S., Martín-Aragoneses, M. T., Del Río, D., & Mejuto, G. (2012). Evaluación de la comprensión gramatical en el envejecimiento normal y patológico: Un resumen de los resultados obtenidos con las baterías ECCO y ECCO_Senior. International Journal of Psychological Research, 5(1), 96-108. [ Links ]
Montenegro, M., Montejo, P., Llanero, M., & Reinoso, A. I. (2012). Evaluación y diagnóstico del deterioro cognitivo leve. Revista de Logopedia, Foniatría y Audiología, 32(2), 47-56. [ Links ]
Mulet, B., Sánchez-Casas, R., Arrufat, M. T., Figuera, L., Labad, A., & Rosich, M. (2005). Deterioro cognitivo ligero anterior a la enfermedad de Alzheimer: tipologías y evolución. Psicothema, 17(2), 250-256. [ Links ]
Olazarán, J., Mouronte, P., & Bermejo, F. (2005). Validez clínica de dos escalas instrumentales en la enfermedad de Alzheimer. Neurología, 20(8), 395-401. [ Links ]
Petersen, R. C. (2011). Mild cognitive impairment. The New England Journal of Medicine, 364(23), 2227-2234. [ Links ]
Petersen, R. C., Doody, R., Kurz, A., Mohs, R. C., Morris, J. C., Rabins, P. V., . . . Winblad, B. (2001). Current concepts in mild cognitive impairment. Archives of Neurology, 58(12), 1985-1992. [ Links ]
Petersen, R. C., Roberts, R. O., Knopman, D. S., Bo-eve, B. F., Geda, Y. E., Ivnik, R. J., . . .Jack, C. R. (2009). Mild cognitive impairment: Ten years later. Archives of Neurology, 66(12), 1447-1455. [ Links ]
Petersen, R. C., Smith, G. E., Waring, C., Ivnik, R. J., Tangalos, E. G., & Kokmen, E. (1999). Mild cognitive impairment. Clinical characterization and outcome. Archives of Neurology, 56(3), 303-308. [ Links ]
Rami, L., Serradell, M., Bosch, B., Caprile, C., Sekler, A., Villar, A., . . . Molinuevo, J. L. (2008). Normative data for the Boston Naming Test and the Pyramids and Palm Trees Test in the elderly Spanish population. Journal of Clinical and Experimental Neuropsychology, 30(1), 1-6. [ Links ]
Reisberg, B., Ferris, S. H., de Leon, M. J., & Crook, T. (1982). The global deterioration scale for assessment of primary degenerative dementia. American Journal of Psychiatry, 139(9), 1136-1139. [ Links ]
Ribeiro, F., de Mendoza, A., & Guerreiro, M. (2006). Mild cognitive impairment: Deficits in cognitive domains other than memory. Dementia and Geriatric Cognitive Disorders, 21 (5-6), 284-290. [ Links ]
Saez-Zea, C., Carnero-Pardo, C., & Gurpegui, M. (2008). Nombres de personas: una prueba de fluidez verbal sin influencias socioeducativas. Neurología, 23(6), 356-360. [ Links ]
Sperling, R. A., Aisen, P. S., Beckett, L. A., Bennett, D. A., Craft, S., Fagan, A. M., ... Creighton, H. P. (2011). Toward defining the preclinical stages of Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & Dementia, 7(3), 280-292. [ Links ]
Taler, V., & Phillips, N. A. (2008). Language performance in Alzheimer's disease and mild cognitive impairment: A comparative review. Journal of Clinical and Experimental Neuropsychology, 30(5), 501-556. [ Links ]
Thornton, R., & Light, L. L. (2006). Language comprehension and production in normal aging. In J. E. Birren & K. W. Schaie (Eds.), Handbook of the psychology of aging (6th ed., pp. 261-287). San Diego, CA: Elsevier. [ Links ]
Traykov, L., Raoux, N., Latour, F., Gallo, L., Hanon, O., Baudic, S., . . . Rigaud, A. (2007). Executive functions deficit in mild cognitive impairment. Cognitive and Behavioral Neurology, 20(4), 219-224. [ Links ]
Wechsler, D. (2004). WMS-III. Escala de memoria de Wechsler-III: manual de aplicación y puntuación. Madrid: TEA Ediciones. (Original publicado en 1997) [ Links ]
Wingfield, A., McCoy, S. L., Peelle, J. E., Tun, P. A., & Cox, L. C. (2006). Effects of adult aging and hearing loss on comprehension of rapid speech varying in syntactic complexity. Journal of the American Academy of Audiology, 17(7), 487-497. [ Links ]
Yesavage, J. A. (1982). Development and validation of a geriatric depression screening scale: A preliminary report. Journal of Psychiatric Research, 17(1), 37-49. [ Links ]
