










Services on Demand
Journal
Article
 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkUniversitas Psychologica
Print version ISSN 1657-9267
Univ. Psychol. vol.15 no.2 Bogotá Apr./June 2016
https://doi.org/10.11144/Javeriana.upsyl5-2.dppq
Development and Psychometric Properties of a New Questionnaire for Assessing Mental Health Literacy in Young People*
Desarrollo y propiedades psicométricas de un nuevo cuestionario de evaluación de alfabetización en salud mental en jóvenes
Luísa Campos**
Pedro Dias***
Filipa Palha****
Ana Duarte*****
Elisa Veiga******
Catholic University of Portugal, Portugal
Artículo de investigación. Financed by the Portuguese Science and Technology Foundation (PT-DC/PSI-PCL/112526/2009) . Acknowledgments: The authors would like to thank the support from Anthony Jorm (consultant of the research project), António Fonseca, Raquel Matos, Maria Xavier, Vânia Sousa Lima, Bárbara César Machado (expertsin Psychology), and the schools where data collection occurred, as well as their boards, teachers and students. The study was awarded a grant from the Portuguese Science and Technology Foundation (PTDC/PSI-PCL/112526/2009) and is part of the Finding Space to Mental Health project - Promoting mental health in adolescents (12-14 years old): development and evaluation of an intervention - developed by the Faculty of Education and Psychology of the Catholic University of Portugal, in partnership with ENCONTRAR+SE - Association for the promotion of mental health.
**Assistant Professor Faculty ofEducation and Psychology. Correo electrónico: mcampos@porto.ucp.pt
***Assistant Professor Faculty of Education and Psychology. Correo electrónico: pdias@porto.ucp.pt
****Lecturer Faculty of Education and Psychology.Correo electrónico: fpalha@porto.ucp.pt
*****Research assistant Faculty of Education and Psychology. Correo electrónico: psic_anaduarte@ gmail.com
******Assistant Professor Faculty of Education and Psychology. Correo electrónico: eveiga@porto.ucp.pt
Recibido: 09 de enero de 2015 Aceptado: 08 de marzo de 2016
Para citar este articulo:
Campos, L., Dias, P., Palha, F., Duarte, A., Veiga, E. (2016). Development and psychometric properties of a new questionnaire for assessing Mental Health Literacy in young people. Universitas Psychologica, 15(2), 61-72. http://dx.doi.org/10.11144/Javeriana.upsyl5-2.dppq
Abstract
Objectives: Several instruments assess constructs related to mental health lite -racy and to the stigma associated with mental health problems. However, most of them have conceptualisations that may limit the assessment of the mental health literacy concept in a more up-to-date and comprehensive perspective. Furthermore, some of the instruments' structure may limit their use in large scale samples, in a short period of time and with repeated measures. This article presents the development of the Mental Health Literacy questionnaire (MHLq) and the studies to assess its psychometric properties. Methods: After item-pool generation, content validity was assessed by experts and a think aloud procedure. The MHLq was tested in two samples of students (study 1 n=239; aged between 12 and 15 years old; study 2 n=737; aged between 11 and 17 years old) to determine its psychometric properties. Results: Factor analysis procedures favoured a three-factor solution (with 33 items) of the MHLq. The questionnaire showed good internal consistency (total score a=0.84; Factor 1 first aid skills and help seeking - a=0.79; Factor 2 knowledge/stereotypes - a=0.78; Factor 3 self-help strategies - a=0.72); and excellent test-retest reliability, the ICC for the total score of MHLq was 0.88 and for the three dimensions of MHLq was 0.80 (Factor 1), 0.90 (Factor 2) and 0.86 (Factor 3). Conclusions: The MHLq is a practical, valid and reliable tool for identifying gaps in knowledge, beliefs and behavioural intentions, in large samples, allowing the development and evaluation of interventions aimed at promoting mental health in young people.
Keywords : Questionnaire; psychometric properties; mental health literacy; young people
Resumen
Objetivos: Varios instrumentos evalúan constructos relacionados con conocimientos sobre la salud mental y al estigma asociado con problemas de salud mental. Sin embargo, la mayoría de ellos tienen conceptualizaciones que pueden limitar la apreciación del concepto de alfabetización de la salud mental de una manera más actual y exhaustiva. Por otra parte, la estructura de algunos de los instrumentos puede limitar su uso en muestras a gran escala, en un corto período de tiempo y con medidas repetidas. Este artículo presenta el desarrollo del cuestionario de alfabetización en salud mental (MHLq) y los estudios para evaluar sus propiedades psicométricas. Método: Después de la generación de ítems, la validez de contenido fue evaluada por expertos y por un procedimiento think aloud. El MHLq ha sido testado en dos muestras de estudiantes (estudio 1 n = 239; con edades comprendidas entre los 12 y 15 años de edad; estudio 2 n = 737; edades comprendidas entre los 11 y 17 años de edad) para determinar sus propiedades psicométricas. Resultados: los procedimientos de análisis factorial indicaron una solución de tres factores (con 33 elementos) del MHLq. El cuestionario mostró una buena consistencia interna (puntuación total a = 0,84; Factor 1 técnicas de primeros auxilios y la búsqueda de ayuda - a = 0.79; Factor 2 de conocimientos / estereotipos - a = 0.78; Factor 3 estrategias de autoayuda - a = 0,72); y una excelente fiabilidad test-retest, la CCI para la puntuación total de MHLq fue de 0,88 y para las tres dimensiones del MHLq fue de 0,80 (factor 1), 0,90 (factor 2) y 0,86 (factor 3). Conclusiones: El MHLq es una herramienta práctica, válida y fiable para la identificación de lagunas en los conocimientos, las creencias y las intenciones de comportamiento, en muestras grandes, lo que permite el desarrollo y la evaluación de las intervenciones destinadas a promover la salud mental en los jóvenes.
Palabras clave : Cuestionario; propiedades psicométricas; alfabetización en salud mental; jóvenes
Background
Mental health literacy has been identified as a prerequisite for early recognition and intervention in mental disorders, and for this reason, it has become a focus of research over the past few decades. The concept was introduced by Jorm and colleagues (1997), who defined mental health literacy as "knowledge and beliefs about mental disorders which aid their recognition, management or prevention" (p. 182). It includes: the ability to recognize and distinguish different mental disorders; knowledge and beliefs regarding risk factors and causes for those disorders; knowledge and beliefs concerning selfhelp and professional help that is available; attitudes that can promote adequate help seeking behavior; and knowledge regarding ways to obtain relevant information about mental health (Jorm, 2000). By assessing an individual's knowledge and beliefs, it is possible to identify the stigma that the individual associates with mental health problems, which is considered to be one of the main obstacles for early recognition and intervention (WHO, 2005). A recent update on this concept included the ability to provide support to someone presenting with a mental health problem, that is, first aid skills (Jorm, 2012). Accordingly, mental health literacy is not limited to having knowledge because knowledge is linked to beliefs that together determine attitudes (e.g., resistance to seek professional help). The concept of mental health literacy has evolved to a more articulated model, including the development of increasingly complex cognitive and social skills related to individual and collective empowerment toward mental health promotion (Bourget Management Consulting, 2007; Canadian Alliance on Mental Illness and Mental Health, 2007).
Assessing this construct is relevant for identifying knowledge gaps and erroneous beliefs concerning mental health issues, to inform the development of interventions aimed at promoting mental health literacy (Schulze, Richter-Werling, Matschinger, & Angermeyer, 2003; Scottish Executive & Healthy Living, 2003; Link, Yang, Phelan, & Collins, 2004), as well as the evaluation of these interventions.
There are several instruments designed to assess constructs related to mental health literacy and the stigma associated with mental health problems.
The interview used at the Australian national survey of youth and parents (Jorm, Wright, & Morgan, 2007) is composed of four vignettes related to young people (from both genders), people diagnosed with depression, people with depression and alcohol misuse, and people with social phobia and psychosis (schizophrenia). The vignettes include 15-year-olds (for the young aged 12 to 17) and 21-year-olds (for the young aged 18 to 25). To begin, an open-ended question is presented, i.e., "What, if anything, do you think is wrong with (John/ Jenny)?" and afterwards, questions concerning opinions on formal and informal types of help, types of possible treatments, beliefs regarding prognosis, risk causes and factors are presented.
The questionnaire used to evaluate the program to reduce stereotypes toward schizophrenia, which was developed in German schools, "Crazy? So what!" (Schulze et al., 2003), is a self-report instrument that includes 19 answer items in a 5-point Likert scale and was created to assess children's and youth's attitudes regarding mental disease, namely social distance (12 items) and stereotypes related to schizophrenia (7 items).
The instrument developed under the scope of the Mind Matters project (Wyn, Cahill, Holdswor-th, Rowling, & Carson, 2000) aims at assessing mental health literacy in high school pupils. It encompasses three parts and 18 items in a 4-point Likert scale: the first part is composed of an item that assesses contact with people suffering from mental health problems; the second includes a multiple choice item (selection of mental disorders from a list of 15 health problems) and 17 items regarding knowledge on mental health issues (selection of the right option from a fouroption list); and the third is focused on the evaluation of beliefs and stigmatizing perceptions related to mental disorders.
The Attribution Questionnaire (Corrigan, Green, Lundin, Kubiak, & Penn, 2001) evaluates the effects of familiarity and social distance toward people suffering from a severe mental disorder in university students. It is composed of 21 items that assess seven constructs (three items per construct): two attitudes (personal responsibility and dangerousness); three emotional reactions (anger, concern, and fear); and two behavioral responses (help and avoidance).
The Attitudes to Mental Illness Questionnaire (Luty, Fekadu, Umoh, & Gallagher, 2006) aims at assessing the attitudes of the general public toward people with mental disorders. From the presentation of a vignette (5 possible vignettes, 3 of which were developed to produce a distinctly negative or positive answer), the respondents make a decision in relation to 5 items in a 5-point Likert scale.
To our knowledge, no questionnaire has been developed that addresses all aspects of the mental health literacy construct, as proposed by Jorm. The interview used at the Australian national survey of youth and parents (Jorm et al., 2007) may be the most complete survey, but it focuses on particular mental health problems. Regarding other instruments, most of them have been developed to assess a particular aspect of mental health literacy: knowledge and beliefs about mental health problems (e.g., Wyn et al., 2000); and attitudes or stigma toward mental disorders/ people experiencing a mental health problem (e.g.,Corrigan et al., 2001; Schulze et al., 2003). They also differ in the type of method used (e.g., based on vignettes or multiple statements).
The development of a new questionnaire to assess mental health literacy, the Mental Health Literacy questionnaire (MHLq), emerged from the need to assess the efficacy of a program to promote the mental health literacy of young people, based on the following aspects a) the age of the program's target population; b) the existence of possible constraints in the use of vignettes with large scale samples, in a short period of time and with repeated measures; and c) the need to assess mental health literacy from a comprehensive perspective of the concept instead of focusing on a restricted number of mental disorders.
This paper presents the process of developing the MHLq and the study of its psychometric properties.
Methods
This study was approved by the Portuguese Data Protection Authority (ID 11098/2011) and by the Portuguese Ministry of Education (ID 0128800003).
Development of the Questionnaire
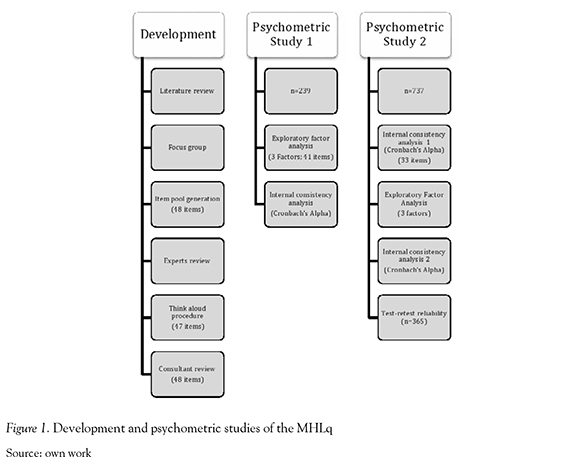
The development of the MHLq began by generating an item pool related to Jorm's definition of Mental Health Literacy described above (Jorm, 2012). This process was based on 1) a literature review on mental health literacy, mental health promotion and mental health problems with higher prevalence in young people; 2) content analysis of the discourse emerging from 4 focus group sessions held with 34 students (12- to 14-year-olds)1 and 3) a review of measures for assessing mental health literacy and related topics.
The first version of the questionnaire, resulting from the process presented above, included: 1) a socio-demographic form, comprised of questions related to the participants' gender, age, school grade, residence, parental occupation and professional status, proximity to people with mental health problems, including the nature of the relationship and the type of mental health problem; 2) 48 items2, organized in a 5-point Likert response scale (1=strongly disagree; 2=disagree; 3= neither agree nor disagree; 4=agree; 5 =strongly agree), concerning 4 sections-knowledge about mental health problems, stereotypes, behavioral intentions (first aid skills, help seeking behavior, and self-help strategies), and specific knowledge approximately 5 mental disorders (Major Depressive Disorder, Generalized Anxiety Disorder, Schizophrenia, Anorexia Nervosa, Substance Abuse); and 3) one multiple-choice item for the identification of mental health problems from a list of health problems.
Content validity was independently examined by five experts who had a PhD in Psychology and who were asked to rate the degree of specificity of the items in relation to the dimensions. From the 48 items examined by the experts, 83.7% achieved complete agreement. From the eight items where agreement was not met, six were assigned to the same dimension by three experts, and two were assigned to different dimensions by three experts. After examining the items that failed to meet agreement between the experts, disagreement was found between the dimensions related to general knowledge and risk factors about mental health problems and between knowledge and stereotypes, showing an overlap between these dimensions. We decided to keep all 48 items at this stage, postponing to the factor analysis further contributions to the decisionmaking process of eliminating or keeping the items.
The second stage of content validity analysis consisted of a think-aloud procedure with a group of 11 participants aged between 11 and 12 years old. All 48 items were presented individually to this group, and participants were asked to comment on the items based on item interpretation and suggested rephrasing for reducing ambiguity. All comments and suggestions made by the participants were registered by the research assistant. Based on this think-aloud procedure, 29 items were rephrased, and one item was removed from the scale because its content was redundant when compared to another item.
At this stage, the consultant of the research project, who was an expert on mental health literacy, reviewed this version of the instrument and suggested the distinction between formal and informal help seeking behavior, which led to the introduction of one item to the scale.
Psychometric properties - study 1
The experimental version of the questionnaire, with 48 items, was administered to a group of 239 students aged between 12 and 15 years old (M=13.12; SD=1.01). Of the students, 53.6% were male and in 7th to 9th grade (41.8% 7th grade; 21.8% 8th grade; 36.4% 9th grade).
Most students (N = 126; 54.3%) reported knowing someone who has a mental health problem, 62 students (26.7%) stated they did not know anyone with these problems, and 44 (19%) were not aware of anyone with these problems. The most common problems identified by students as mental health problems in people they knew included Down's Syndrome (n=45; 18.8%); Tourette's Syndrome (N=14; 5.9%); Alzheimer's (n=10; 4.1%); Mental Retardation (n=8; 3.3%); Depression (n=5; 2.1%); Autism (n=4; 1.7%); Schizophrenia (n=3; 1.3%); and Stroke (n=2; 0.8%). Twenty-three students (9.6%) were unable to identify the mental health problem.
Regarding the degree of proximity, 62 students (46.6%) mentioned the selected person to be a friend, 31 (23.3%) a family member, 36 (27.1%) another person, 2 (1.5%) referred him(her)self, and 2 (1.5%) several people.
Regarding parental professional status, most parents (97% of fathers and 92.6% of mothers) were employed.
Psychometric properties, i.e., construct validity and internal consistency, of the MHLq were evaluated using exploratory factor analysis (Principal components analysis, with Varimax rotation) and Cronbach's Alpha. Both analyses were used as complementary procedures for determining the final structure of the instrument (Janda, 1998). The criteria used for the factor analysis were: a) item loadings larger or equal to 0.20; and b) content of items loading in factors should be compatible with the underlying theoretical content.
Psychometric properties - study 2
The second psychometric study was conducted with a larger sample of 737 students3 aged between 11 and 17 years old (M=13.08; SD=1.06) who were in grades 7th to 9th (7th grade = 28.8%; 8th grade = 32.6%; and 9th grade = 38.7%) in eight schools. Regarding the gender of participants, 52.8% were male. Six hundred and twenty-three (84.5%) participants' parents were employed, 106 (14.4%) were unemployed, and eight (1.1%) participants did not respond to this question.
Almost half of the participants reported knowing someone with a mental health problem (n=324; 44.5%), 221 students (30.4%) stated they did not know anyone with these problems, and 183 (24.1%) were not aware. The mental health problems that students identified the most in people they knew included Depression (n=49; 16.4%); Down's Syndrome (n=42; 14.0%), Alzheimer's (n=36; 12.0%); Mental Retardation (n=27; 9.0%); Autism (n=19; 6.4%); and Schizophrenia (n=13; 4.3%). Forty-one participants (13.7%) were unable to identify the mental health problems. Regarding the degree of proximity, 133 (39.3%) mentioned the selected person to be a family member, 129 (38.2%) a friend, 66 (19.5%) another person, 8 (2.4%) referred him(her)self, and 2 (0.6%) reported several people.
Psychometric properties of the MHLq were evaluated following the same procedures in study 1. Additionally, the intraclass correlation coefficient (ICC) was used to study the test-retest reliability of the MHLq.
Results
Figure 1 presents both the stages followed during the development and psychometric studies of MHLq.
Psychometric study 1
After a first exploratory factor analysis retaining all factors with an eigenvalue higher than 1.0, the factorial solution failed to meet the conceptual organization of the instrument, and most items presented loading values higher than 0.20 in the first three factors. Therefore, a second exploratory factor analysis, using a fixed number of factors extraction procedure (3 factors) was conducted. The factor structure included: Factor 1) items related to first aid skills and help seeking behavior; Factor 2) items related to knowledge and stereotypes (with negative loadings); and Factor 3) items related to self-help strategies. This solution was responsible for 22.91% of the variance. Considering factor loadings, eleven items should be removed from the questionnaire. However, seven of those items were compatible with the underlying theoretical content, suggesting that they should be maintained, and only seven items were removed because they failed to load the corresponding factor to the conceptual dimension that they were assessing. Cronbach's Alpha values were satisfactory for the three sub-scales: first aid skills and help seeking a=0.78, knowledge/stereotypes a=0.71, and self-help strategies a=0.71.
The version of the MHLq that resulted from this study includes 41 items on a 5-point Likert scale and one multiple-choice item.
Psychometric study 2
The first stage of the psychometric study 2 consisted of examining the internal consistency of all of the 41 items of the MHLq as a mental health literacy total score. Thirty-three items presented an item-total correlation of 0.20 or above. The eight items presenting lower item-total correlations were removed from the following analyses. Cronbach's Alpha for the 33 items was a=0.84.
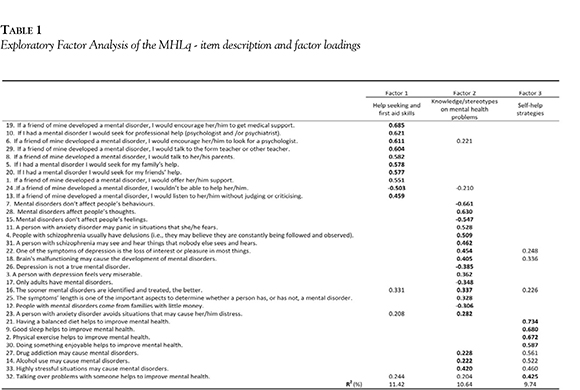
An exploratory factor analysis was conducted on the 33 items (three factors extraction), as suggested by psychometric study 1. This factorial solution, which was responsible for 31.8% of the total variance, included 10 items in Factor 1 (first aid skills and help seeking), 18 items in Factor 2 (knowledge/stereotypes), and five items in Factor 3 (self-help strategies). Table 1 presents the final factor structure of MHLq.
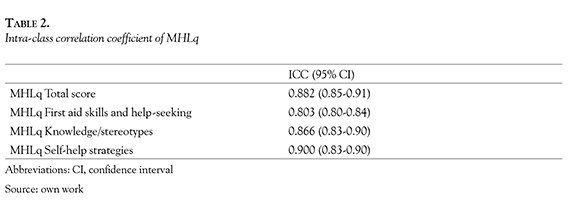
Internal consistency of the three factors (Cronbach's Alpha) was as follows: Factor 1, a=0.79; Factor 2, a=0.78; and Factor 3, a=0.72. Temporal stability of the MHLq was assessed through the re-administration of the questionnaire to a subset of n=365 participants two weeks after the first assessment. The demographic characteristics of these participants were similar to the entire sample (Mage=13.16; SD=1; 52% males; 23% attended the 7th grade, 37.5% the 8th grade and 39.5% the 9 th grade). The ICC for the total score of MHLq was 0.88 and for the three dimensions was 0.80 (first-aid skills and help seeking), 0.90 (knowledge/stereotypes), and 0.86 (self-help strategies) (see table 2).
The total score for the 33 items of the MHLq ranged between 62 and 158 (M=131.43; SD=11.35). First aid skills and help seeking factor scores ranged between 14 and 50 (M=41.65; SD =5.06). Knowledge/stereotypes factor scores ranged between 43 and 90 (M=69.99; SD=7.13). Self-help strategies factor scores ranged between 5 and 25 (M=19.48; SD=3.18).
Regarding the results for the multiple-choice item, 74.1% (n=546) of the students identified schizophrenia as a mental health problems, 74.1% (n=546) indicated depression, 50.9% (n=375) cerebral palsy, 48.4% (n=357) anxiety, 40.4% (n=297) trisomy 21, 35.5% (n=262) stroke and 35.5% (n=262) referred Parkinson's disease.
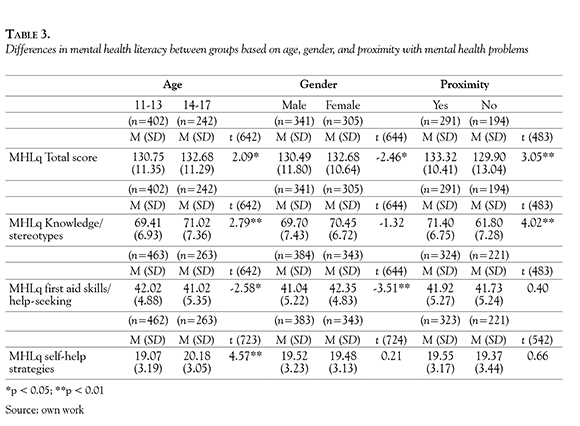
Socio-demographic variables (age, gender, and proximity with people presenting with mental disorders) are related to differences in MHLq scores (see table 3). Students aged between 14 and 17 years old presented higher scores on the MHLq total score, knowledge/stereotypes, and self-help strategies compared to younger participants. However, younger participants (11-13 years old) presented higher scores than older participants in first-aid skills and help-seeking behavior. Regarding gender differences, girls showed higher scores on the MHLq total score, first-aid skills and help-seeking behavior than boys. Finally, students who indicated knowing someone with a mental health problem showed higher scores on the MHLq total score and knowledge/stereotypes compared to students who do not know anyone presenting with mental health problems.
Discussion
In recent years, concern about the number of children and youth who are experiencing mental health problems has been growing, and from a preventive perspective, the need to intervene as early as possible to promote children's positive mental health and well-being has become urgent.
Having mental health literacy enables the prevention, identification, and adequate and early management of psychopathological symptoms (Jorm, 2000, 2012; Li, 2012; Wei, Hayden, Kut-cher, Zygmunt, & McGrath, 2013), in addition to the provision of help for people suffering from these problems (Gulliver Griffiths, & Christensen, 2010; Jorm, 2012; Kelly, Jorm & Wright, 2007). The probability of early recognition of mental health problems and the appropriate help-seeking behaviors is increased if people are appropriately "literate" in this field (Kitchener & Jorm, 2004).
Assessing mental health literacy in young people allows the identification of knowledge, beliefs and attitudes on mental health issues that can contribute to the definition of education and health policies related to mental health promotion, a priority defined by the World Health Organization (2005), allowing the design and evaluation of intervention programs in different contexts (e.g., schools, general community) and with diverse aims (e.g., fighting stigma; promoting mental health behavior).
The purpose of this study was to develop and examine the psychometric characteristics of a brief self-report instrument that assesses young people's mental health literacy, taking into account a comprehensive perspective of the construct (Jorm, 2012), and overcomes possible constraints in the use of vignettes (e.g., time-consumption, focus on a restricted number of mental disorders (Jorm, Wright & Morgan, 2007; Loureiro, 2012) and enables data collection with large samples in a short period of time and with repeated measures.
The results from both psychometric studies indicate that the construct related to mental health literacy has a threedimensional structure (first aid skills and help-seeking behavior, knowledge/stereo-types, and self-help strategies) and has adequate levels of internal consistency and test-retest reliability.
Throughout the development of the questionnaire, all of the procedures recommended for this purpose were followed (Freire & Almeida, 2001; Hinkin, 1998; Netemeyer, Bearden, & Sharma, 2003). To begin, a pool of items was generated and processes with a deductive nature were used as a starting point. A literature review on the construct related to mental health literacy and on instruments to assess it and data emerging from an inductive approach was also completed because focus groups were developed with participants from the target population in the first stage of the Finding Space to Mental Health Project (Hinkin, 1998).
The items were submitted to an assessment of content validity with the help of experts and a think-aloud procedure (Van Someren, Barnard, & Sandberg, 1994) carried out with a sample with similar characteristics to the ones describing the target population.
These procedures were of utmost importance so that the questionnaire would be better tailored to the target-group, enabling the creation of an experimental version of the instrument, incorporating items more suitable to the level of understanding of the target population, compatible with the multidimensional perspective of the construct related to mental health literacy and representative of that exact same construct. We consider this stage crucial for the MHLq development, in particular the transformation through the rephrasing of a significant number of items as a result of the think-aloud procedure. This applies not only to items that raised ambiguity regarding their content but also to items that, even though they were easily understood by the participants, elicit reformulation proposals to achieve greater clarity.
First, the organization of both psychometric studies made it possible to reduce the number of items, withdrawing the ones that contributed to weaken the instrument's factorial structure and internal consistency. Second, having the opportunity to test the instrument with a second sample that was larger and more heterogeneous enabled the refinement of the instrument's structure and the confirmation of its internal consistency. Regarding the factorial structure of the MHLq, it is noticeable the choice for the integration, in one single factor, of the items initially included in the knowledge section and in the stereotypes section. This option was based first on the results achieved with the factorial analyses, which pointed to the saturation of these items in one single factor, and second, on the conceptual closeness between these two constructs. In other words, stigmatizing beliefs have their origin in misconceptions about this theme, just as indicated by the stigma model proposed by Corrigan (2000), when the stereotypes are defined as knowledge cognitive structures. An example of a misconception included in the stereotypes dimension of the MHLq is item 12, "People with mental disorders come from families with little money". Concerning the internal consistency of the MHLq, the achieved alpha values are higher than the values considered acceptable (Kline, 2000).
The use of the MHLq in two moments, with a subsample from study 2, made it possible to assess the test-retest reliability. The choice for a two-week break is generally believed to be a reasonable compromise between recollection bias and unwanted change (Marx, Menezes, Horovitz, Jones, & Russel, 2003). The ICC values obtained in all dimensions of the questionnaire were > 0.80, indicating excellent reliability (Rosner, 1995).
This study explored the impact of sociodemographic variables on the levels of mental health literacy. Differences were found regarding age, gender and closeness to someone with a mental health problem. Girls showed higher scores on the MHLq total score, first-aid skills and help-seeking behavior than boys. The research on this topic sustains some of the differences encountered, as far as gender is concerned, as females are more sensitive to mental health issues, both in terms of knowledge and willingness to take action when facing a problem of this nature (Burns & Rapee, 2006; Cotton, Wright, Harris, Jorm, & McGorry, 2006; Williams & Pow, 2007). This finding is particularly important to consider when designing interventions to promote mental health literacy in young people, as boys are particularly at risk for some disorders and should be better prepared to respond appropriately.
Regarding closeness to someone with a mental health problem, students who indicated knowing someone with a mental health problem showed higher scores on the MHLq total score and knowl-edge/stereotypes compared to students who do not know anyone presenting with mental health problems. Similar results were found in several studies (Lauber, Nordt, Falcato, & Rossler, 2001; Angermeyer et al., 2004).
Concerning participants' age, the results are inconsistent. Older students (14-17) presented higher scores than younger participants on the MHLq total score, knowledge/stereotypes, and selfhelp strategies, but younger students (11-13) presented higher scores in first-aid skills and help-seeking behavior compared to older participants. Age differences in mental health literacy were previously explored in an Australian national survey (Farrer, Leach, Griffiths, Christensen, & Jorm, 2008) concerning the recognition of depression and schizophrenia and associated risk factors, treatments and sources of help. The results indicated that younger people have more accurate knowledge than the elderly regarding the recognition and treatment of depression, but not concerning schizophrenia. Younger people also tended to identify informal treatment sources as helpful, while the elderly rated fewer sources as helpful overall. Although this study compared adult participants from a wide age range (18 - 70 years old), it suggests that age plays a role in mental health literacy. Further studies with young people should examine these differences. The MHLq comprises one multiple-choice item aimed at the identification of 3 mental health problems from a list of 7 health conditions. The descriptive results presented in study 2 suggest some difficulties among the participants in differentiating mental health problems from other health conditions. This item allows a specific assessment of knowledge related to mental health problems and is useful for the design and assessment of interventions to promote mental health.
Future research should examine the sensitivity of the MHLq in the evaluation of intervention programs, as well as its convergent and discriminant validity. The development of a version of the MHLq for adults is in progress, given the universality of the contents assessed and the potential benefits arising from their application (both conceptual and methodological).
Conclusion
The MHLq is a valid and reliable self-report instrument for assessing mental health literacy in young people from a more up-to-date and comprehensive perspective of the construct, hence avoiding the focus on specific mental disorders, unlike other instruments. The use of the MHLq, which is a brief instrument, is specifically designed for its target-population and allows for a practical way of evaluating interventions aimed at promoting mental health literacy in young people. Future developments of this measure include its adaptation for other age groups.
Pie de página
1Focus groups were developed in the first stage of the Finding Space to Mental Health Project - an intervention study for mental health promotion- and contributed to the development of a mental health promotion intervention and the MHLq questionnaire. From the topics discussed during the focus groups, those related to the development of the questionnaire were: 1) definition, prevalence, risk factors, impact, and prognosis of mental disorders; behavioral intentions towards mental health problems; 2) definition and relevance of mental health; variables related to the promotion of mental health and prevention of mental disorders.
234 items positively formulated (high scores corresponding to superior levels of mental health literacy) and 14 items formulated in reverse (higher answer scores correspond to inferior levels of mental health literacy).
3This sample is part of the second stage of the Finding Space to Mental Health project.
References
Angermeyer, M., Matschinger, H., & Corrigan, P. (2004). Familiarity with mental illness and social distance from people with schizophrenia and major depression: testing a model using data from a representative population survey. Schizophrenia Research, 69, 175- 182. [ Links ]
Bourget Management Consulting for the Canadian Alliance on Mental Illness and Mental Health. (2007). Mental Health Literacy: A Review of the Literature. Retrieved from www.camimh.ca/files/literacy/LIT_REVIEW_MAY_6_07.pdf [ Links ]
Burns, J., & Rapee, R. (2006). Adolescent mental health literacy: Young people's knowledge of depression and help seeking. Journal of Adolescence, 29, 225- 239. [ Links ]
Canadian Alliance on Mental Illness and Mental Health. (2007). Mental Health Literacy in Canada: Phase One Project Mental Health Literacy Project. Retrieved from http://www.camimh.ca/files/lit-eracy/MHL_REPORT_Phase_One.pdf [ Links ]
Corrigan, P. (2000). Mental health stigma as social attribution: implications for research methods and attitude change. Clinical Psychology Science and Practice, 7(1), 48-67. [ Links ]
Corrigan, P., Green, A., Lundin, R., Kubiak, M., & Penn, D. (2001). Familiarity with and social distance from people who have serious mental illness. Psychiatric Services, 52, 953-958. [ Links ]
Cotton, S., Wright, A., Harris, M., Jorm, A., & McGorry, P. (2006). Influence of gender on mental health literacy in young Australians. Australian and New Zealand Journal of Psychiatry, 40, 790-796. [ Links ]
Farrer, L., Leach, L., Griffiths, K., Christensen, H., & Jorm, A. (2008). Age differences in Mental Health Literacy. BMC Public Health, 8(125), 1-8. [ Links ]
Freire, T. & Almeida, L. (2001). Escalas de Avaliação: Construção e validação. In: Fernandes E and Almeida L (eds) Métodos e Técnicas de Avaliação: contributos para a prática e investigação psicológicas (pp.109-128). Braga: Universidade do Minho, Centro de Estudos em Educação e Psicologia. [ Links ]
Gulliver, A., Griffiths, K., & Christensen, H. (2010). Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry, 10(113) 1-9. [ Links ]
Hinkin, T. (1998). A Brief Tutorial on the Development of Measures for Use in Survey Questionnaires. Organizational Research Methods, 1(1), 104-121. [ Links ]
Janda, L.H. (1998). Psychological testing: theory and applications. Massachusetts: Ally & Bacon. [ Links ]
Jorm, A. (2000). Mental health literacy: public knowledge and beliefs about mental disorders. British Journal of Psychiatry, 177, 396-401. [ Links ]
Jorm. A. (2012). Mental health literacy: empowering the community to take action for action for better mental health. American Psychologist, 67(3), 231-243. [ Links ]
Jorm, A., Korten, A., Jacomb, P., Christensen, H., Rodgers, B., & Pollit, P. (1997). Mental health literacy": a survey of the public's ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Medical Journal of Australia, 166(4), 182-186. [ Links ]
Jorm, A., Wright, A., & Morgan, A. (2007). Beliefs about appropriate first aid for young people with mental disorders: findings from an Australian national survey of youth and parents. Early Intervention in Psychiatry, 1, 61-70. [ Links ]
Kelly, C., Jorm, A., & Wright, A. (2007). Improving mental health literacy as a strategy to facilitate early intervention for mental disorders. Medical Journal of Australia, 187(7), S26-S30. [ Links ]
Kitchener, B., & Jorm, A. (2004). Mental health first aid training in a workplace setting: A randomized controlled trial. BMC Psychiatry, 4(23 ) 1-8. [ Links ]
Kline, P. (2000). The handbook of psychological testing (2nd ed.). London: Routledge. [ Links ]
Lauber, C., Nordt, C., Falcato, L., & Rossler, W. (2001). Lay recommendations on how to treat mental disorders. Social Psychiatry and Psychiatric Epidemiology, 36, 553-556. [ Links ]
Li, H. (2012). Mental health literacy, stigma, and early intervention. Asian Journal of Psychiatry, 5, 209-210. [ Links ]
Link, B., Yang, L., Phelan, J., & Collins, P. (2004). Measuring mental illness stigma. Schizophrenia Bulletin, 30(3), 511-541. [ Links ]
Loureiro, L. (2012). Questionário de Avaliação da Literacia em Saúde Mental - QuALiSMental: estudo das propriedades psicométricas. Revista de Enfermagem Referência, 4(4), 79-88. [ Links ]
Luty, J., Fekadu, D., Umoh, O., & Gallagher, J. (2006). Validation of a short instrument to measure stigmatized attitudes towards mental illness. Psychiatric Bulletin, 30, 257-260. [ Links ]
Marx, R.G., Menezes, A., Horovitz, L., Jones, E., & Russel, W. (2003). A comparison of two time intervals for test-retest reliability of health status instruments. Journal of Clinical Epidemiology, 56, 730-735. [ Links ]
Netemeyer, R.G., Bearden, W.O., & Sharma, S. (2003). Scaling procedures: issues and applications. Thousand Oaks: Sage Publications. [ Links ]
Rosner, B. (1995). Fundamentals of biostatistics. Toronto: Duxbury Press. [ Links ]
Schulze, B., Richter-Werling, M., Matschinger, H. & Angermeyer, M.C. (2003). Crazy? So what! Effects of a school project on students' attitudes towards people with schizophrenia. Acta Psychiatrica Scandinavica, 107, 142-150. [ Links ]
Scottish Executive & Healthy Living. (2003). National Programme for Improving Mental Health and WellBeing: Action plan 2003-2006. Edinburgh: Scottish Executive. [ Links ]
Van Someren, M.W., Barnard, Y.F. & Sandberg, J.C. (1994). The think aloud method. A practical guide to modelling cognitive processes. London: Academic Press. [ Links ]
Wei, Y., Hayden, J., Kutcher, S., Zygmunt, A., & McGrath, P. (2013). The effectiveness of school mental health literacy programs to address knowledge, attitudes and help seeking among youth. Early Intervention in Psychiatry, 7, 109-121. [ Links ]
Williams, B., & Pow, J. (2007). Gender Differences and Mental Health: An Exploratory Study of Knowledge and Attitudes to Mental Health Among Scottish Teenagers. Child and Adolescent Mental Health, 12(1), 8-12. [ Links ]
World Health Organization. (2005) Atlas: Child and Adolescent Mental Health Resources: Global Concerns, Implications for the Future. Report, Geneva. [ Links ]
Wyn, J., Cahill, H., Holdsworth, R., Rowling, L., & Carson, S. (2000). MindMatters, a whole-school approach promoting mental health and wellbeing. Australian and New Zealand Journal of Psychiatry, 34, 594-601. [ Links ]

