










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombia Médica
On-line version ISSN 1657-9534
Colomb. Med. vol.42 no.3 Cali July/Sept. 2011
Behavior of indirect maximal oxygen uptake on users of the PROSA Program at Universidad de Antioquia, Medellín, Colombia
Jorge Jaime Márquez, MD1, Gildardo Díaz, Lic2, Cristiam Paul Tejada, Lic3
1. Professor, University Institute of Physical Education, Universidad de Antioquia, GRICAFDE Group, Medellín, Colombia. e-mail: jaimejorge33@yahoo.com
2. Professor of Physical Education, Universidad de Antioquia, GRICAFDE Group, Medellín, Colombia. e-mail: coorprosa@gmail.com
3. Professor of Physical Education, Popular Sports Schools Program, INDER, Medellín, Colombia. GRICAFDE Group. e-mail: cristejada2002@yahoo.es.
Received for publication October 23, 2009 Accepted for publication April 24, 2010
ABSTRACT
Objective: This research work sought to describe the behavior of maximal oxygen uptake (VO2max) in a population of adults who performed regular physical activity and classify the level of cardio-respiratory fitness.
Methods: 819 results were analyzed with the estimated 2000-m VO2max test from 2001 to 2009 of 125 subjects who exercise regularly in the PROSA program at Universidad de Antioquia and were discriminated by decade and gender.
Results: The results showed that VO2max reached its peak between 30 and 39 years of age in men (52.0 ± 2.5 ml * kg-1 * min-1) and women (42.9 ± 3.5 ml * kg-1 * min-1). There were significant differences between the VO2max of men and women and the decline in all age groups, except for those over 70 years of age. The VO2max of men in the study was maintained between the 70 and 90 percentiles, while that of women was between 70 and 80 percentiles.
Conclusion: The decline in VO2max associated with age is different for men and women and it is different in almost all age groups.
Keywords: Maximal oxygen uptake; Cardio-respiratory fitness; Aging.
Colomb Med. 2011; 42: 327-33
Comportamiento del consumo máximo de oxígeno indirecto en los usuarios del Programa PROSA de la Universidad de Antioquia, Medellín, Colombias
RESUMEN
Objetivo: Describir el comportamiento del consumo máximo de oxígeno (VO2Máx) en una población de adultos que realiza actividad física regular y clasificar el nivel de fitness cardiorrespiratorio.
Métodos: Se analizaron 819 resultados del VO2Máx estimado con la prueba de 2000 metros entre los años 2001 a 2009 de 125 sujetos que realizan ejercicio físico regular en el Programa PROSA de la Universidad de Antioquia y se discriminaron por década y sexo.
Resultados: Se mostró que el VO2Máx alcanzó su pico máximo entre las edades de 30 a 39 años en hombres (52 ± 2.5 ml * kg-1 * min-1) y mujeres (42.9 ± 3.5 ml * kg-1 * min-1). Se encontraron diferencias significativas entre el VO2Máx de hombres y mujeres y en la disminución en todos los grupos etarios, excepto en los mayores de 70 años. El VO2Máx de los hombres del estudio se mantiene entre los percentiles 70 y 90; el de las mujeres entre los percentiles 70 y 80.
Conclusión: La disminución del VO2Máx asociada con la edad es diferente para hombres y mujeres y también en casi todos los grupos etarios.
Palabras clave: Consumo máximo de oxígeno; Fitness cardiorrespiratorio; Envejecimiento.
Colomb Med. 2011; 42: 327-33
There is sufficient evidence to support that levels of cardio-respiratory fitness are inversely associated with all-cause mortality, heart disease, cancer, and other chronic diseases and that cardio-respiratory fitness is related to health, independence, and functional capacity1-4 and there is interest in the investigation of the decline in age-related VO2max5; although there are differences in the studies, these generally reported a decrease of 0.4-0.5 ml/kg/min/year (9%-10% per decade) for men and women, regardless of the level of activity5,6. High-intensity regular exercise can reduce this loss to 50% in young or middle-aged men but not in older adults; women do not seem to be able to reduce it to less than 10% per decade. The loss of age-related VO2max appears to occur non-linearly in association with decreased physical activity. In sedentary individuals, this occurs between 20 and 30 years of age, and in athletes after reducing or completing training5.
Measuring or estimating VO2max can be performed with direct and indirect standardized assessments7,8. Direct assessments are those that measure VO2max and other physiological variables by using, for example, respiratory gas analyzers. Indirect assessments are those designed to estimate VO2max without the need for special equipment and are based on equations with variables such as gender, age, height, weight, and distance traveled and can be performed on a running track, a treadmill, etc.; these include the Cooper test, Balke test, the Rockport 1-mile test, 1.5-mile running test, and the 2000-m Ukk test9.
In our environment, we know of no published research on the subject and because of the variability of results, the aim ofthis study was to describe the behavior of maximal oxygen intake in a population of adults who perform regular physical activity and secondarily, to classify the level of cardio-respiratory fitness.
MATERIALS AND METHODS
This descriptive study was conducted by reviewing digital records from the 2000-meter Test of PROSA program users from 2001-2009.
PROSA is the psychophysical health program of Universidad de Antioquia and it employs physical activity and exercise as a means for disease prevention and health promotion. It is directed to employees, teachers, and retirees of Universidad de Antioquia, regardless of gender and age. The program works year round, with a frequency of 5 days per week and with a 1-h duration per session. The 380 individuals are divided into 13 groups who exercise mornings, noon, and evenings. Each of the users participating in the program has a sports medical follow-up seeking to prescribe and monitor exercise (the execution and exercise prescription is to be individualized and follow the American College of Sports Medicine (ACSM) recommendations)6.
Secondary sources were used (digital records) of 125 subjects intentionally selected from a total population of 380 individuals. Subjects who had at least three assessments of indirect maximal oxygen intake between 2001 and 2009 were considered as inclusion criterion. We excluded subjects who had less than three assessments to consider only people who have had greater participation in the program.
Estimation of VO2max. To estimate the indirect maximal oxygen uptake of users of the PROSA program, we calculated the time spent in the 2000-m test by using the following parameters: For individuals who can only perform the test by walking, we consider the following variables and formulas, respectively: time: duration of the run in minutes and seconds; heart rate: at the end of the test (in beats per minute); body mass index (BMI): (weight divided by the square of height in meters); age: years old; VO2max = 84.9-4.65 * time-0.22 * heart rate -0.26 * age-1.05 * BMI (for men). VO2max= 116.2-2.98 * time-0.11 * heart rate-0.14 * age-0.39 * BMI (for women). For individuals who take the test by jogging, we have accounted the time spent in minutes and seconds and used the following formula: VO2max=11.6 + 0.176 * (2000/time).
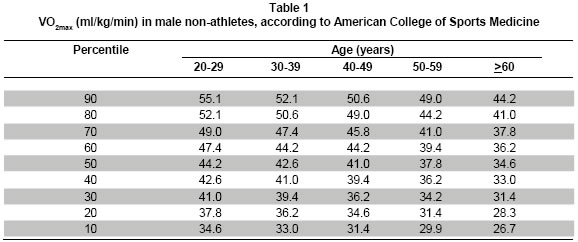
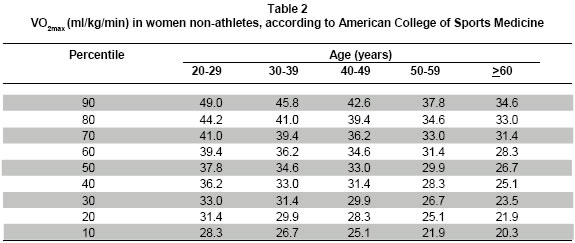
Statistical analysis. For statistical analysis, data collected from digital files were entered into the Excel® spreadsheet and we calculated the mean, standard deviation, and coefficient of variation. VO2max data were grouped into 10-year intervals in both men and women, and were placed into percentiles and compared with ACSM reference tables (Table 1 and 2)6. We also applied the Student t test to establish significant differences between the values of VO2max for men and women, as well as by age groups. ANOVA was applied and a Tukey test was applied to determine significant differences between age groups of men and between age groups of women.
RESULTS
We analyzed the records of the 2000-m test of 125 subjects, 50 men (40%) and 75 women (60%) with mean age of 57.7 ± 9.1 years and 54.7 ± 11.6 years, respectively.
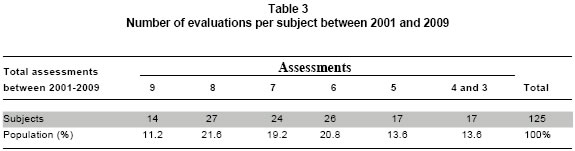
Table 3 shows the number of follow-up evaluations conducted between 2001 and 2009. It is noted that subjects with 6, 7, 8, and 9 assessments represent 73% of the study population.
In whole, we analyzed 819 data of VO2max, 338 (41.3%) from men and 481 (58.7%) from women. Table 4 adds the evaluations between 2001 and 2009. It is observed that between 50 and 59 years of age, 305 evaluations were analyzed for men and women.
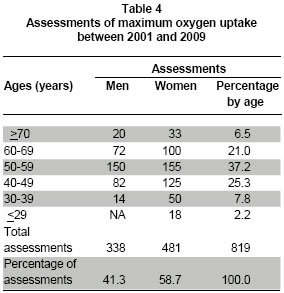
Table 5 presents changes in VO2max with age in men and women. It is noted that the best average was between 30 and 39 years for both men (52 ml * kg-1 * min-1) and women (49.2 ml * kg-1 * min-1); thereafter, there is a decrease of VO2max. Significant differences were found between maximal oxygen uptake for men and women and there were also differences between age groups, except for those older than 70 years of age (p=0.30).
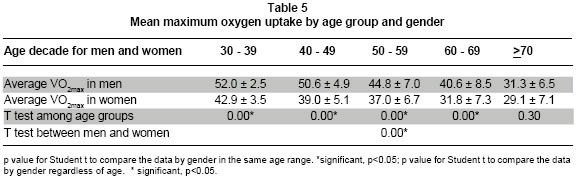
According to the results presented in Table 6, in the group of men there are significant differences from 40 years of age; in that of women, although differences existed between 30 and 40 years of age, the differences become more well-known and constant from 50 years of age.
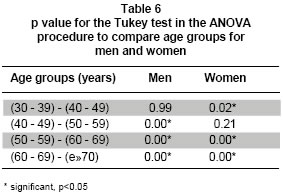
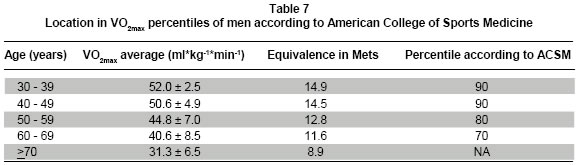
Table 7 shows the VO2max expressed in ml* kg- 1*min-1 and Mets per decade in men and the location in percentiles according to the ACSM. It is noted that the average VO2max with age in men is between the 70th and 90th percentiles. For men over 70 years of age, percentiles were not found because ASCM tables do not report accurate data for that age range.
Table 8 describes the VO2max expressed in ml * kg-1 * min-1 and at Mets per decade in women and their location in percentiles according to the ACSM. It is noted that the average VO2max according to age in women is between the 70th and 80th percentiles.
DISCUSSION
This study describes changes in VO2max associated with age over a period of nine years. The direct comparison with other cross-sectional or longitudinal studies is not the most accurate because there are differences in methodology and population, but, in general, in these, the trend is the decline of VO2max with age in men and women5,10-16 starting from 25 to 30 years of age, once physical maturity has been reached5,13,17.
There is controversy on the impact of physical activity in the rate of loss of aerobic power10,18,19,20,21. The meta-analysis of cross-sectional studies found no association between increased physical activity with decreased VO2max10,19, longitudinal studies suggest that regular vigorous exercise may slow to 50%, but the reduction or suspension of training with the elderly may result in a misleading acceleration in that decline10; a study recently reported decreased VO2max of 1% per annum after 25 years in subjects who do not perform physical activity and of 0.5% per annum for adult athletes; for other researchers, aerobic capacity declines 5-15% per decade5,17, an equivalent reduction of as much as 60% from 30 to 70 years ofage; a recent review reported an average 5 ml/kg/min per decade for all age groups and reported that progressive aerobic training can improve VO2max at least 5-6ml/kg/min22 and others report that the annual rate of decline in VO2max expressed in relative terms varies from 0.25 to 1.04ml/kg/min, depending on gender and level of physical activity17.
In our study population, the decrease of VO2max behaves indifferent form between every decade of life and significant differences between age groups exist (p=0.00); therefore, it would be suitable to express the VO2max and its decrease during the course of time, according to age groups in men and women.
Multiple studies suggest that age-associated decline is greater in men than in women when expressed in absolute terms such as l or ml / min, but when expressed per decade, the apparent gender difference disappears10. Although cross-sectional studies show a linear decrease of VO2max through life, a decline nonlinear acceleration of about 20% after 70 years of age was reported in longitudinal studies5,13,17.
In our study and in a longitudinal study13, the rate of decline in VO2max varies among decades and has a considerable increase after 60 years of age. Also, there is an accelerated decrease per decade independent from the level of physical activity in men and women; comparatively, women have lower VO2max; this has also been reported in another study in individuals 60-92 years of age14.
For all the foregoing, it is proposed that the percentage or the annual change in VO2max can not be generalized but expressed in terms of age and gender of the individuals.
VO2max loss is due to central and peripheral adaptations5,17 and the decline in vigorous physical activity and age-related sarcopenia exacerbate the process13,17; related to these changes and to improve health, ACSM and other organizations recommend aerobic and strength training since early stages of life6.
Vigorous aerobic training can produce a 25% improvement of VO2max (5-6 ml/kg/min) in the elderly, potentially delaying the loss of independence by 10 to 12 years6,22. Controlled programs of regular exercise could contribute to the attenuation of the decline in agerekted VO2max6,14.
A recent meta-analysis23 reported that those with the best cardio-respiratory fitness (VO2max ≥ 7.9 Mets vs. VO2max ≤ 7.9 Mets) is associated with lower risk of mortality from all causes and cardiovascular events in healthy men and women. The lowest level of VO2max (8.3 Mets) -70th percentile- was for women over 70 years of age, but this value is classified as highly fitting into percentiles based on the location. This may mean they would get those benefits associated with the level of fitness and reduced risk of coronary heart disease, cancer, other chronic diseases, and better health and independence1-4,22,23.
Although a limitation of the study was measured by indirect VO2max 2000-m UKK test, a 0.85 correlation was found with laboratory tests, along with a prediction error of 0.05 ml * min-1 * kg-124; similarly, the 2000-m running test has a correlation of 0.71 (p<0.0001) with respect to ergospirometric evidence25. It should also be noted that the ACSM VO2max data are from the United States population, but they are now the world reference6.
On the other hand, physical activity should ideally be assessed to stratify the groups and get more specific results from the age groups. Therefore, it would be important to perform prospective longitudinal studies that allow easily controlling multiple variables.
CONCLUSIONS
VO2max had its peak in individuals between 30 and 39 years of age; in men it was 52 ± 2.5 ml * kg-1 * min-1 and 42.9 ± 3.5 ml * kg-1 * min-1 in women; thereafter, decreasing over the years. The decline in VO2max associated with age is different for men and women and also different in almost all age groups.
In comparison with the ACSM tables, the population of individuals in the PROSA program remain at least at the 70th percentile, therefore, their cardio-respiratory fitness -VO2max- for age is high.
Conflict of interest. None of the authors has conflicts of interest related to this study.
REFERENCES
1. Laukkanen JA, Pukkala E, Rauramaa R, Makikallio TH, Toriola AT, Kurl S. Cardiorespiratory fitness, lifestyle factors and cancer risk and mortality in Finnish men. Eur J Cancer. 2010; 46: 355-63. [ Links ]
2. Prasad DS, Das BC. Physical inactivity: a cardiovascular risk factor. Indian J Med Sci. 2009; 63: 33-42. [ Links ]
3. Lavie CJ, Thomas RJ, Squires RW, Allison TG, Milani RV. Exercise training and cardiac rehabilitation in primary and secondary prevention of coronary heart disease. Mayo Clin Proc. 2009; 84: 373-83. [ Links ]
4. Nocon M, Hiemann T, Müller-Riemenschneider F, Thalau F, Roll S, Willich SN. Association of physical activity with all-cause and cardiovascular mortality: a systematic review and meta-analysis. Eur J Cardiovasc Prev Rehabil. 2008; 15: 239-46. [ Links ]
5. Hawkins S, Wiswell R. Rate and mechanism of maximal oxygen consumption decline with aging: implications for exercise training. Sports Med. 2003; 33: 877-88. [ Links ]
6. American College of Sports Medicine. ACSM's Guidelines for Exercise Testing and Prescription. 7a ed. Philadelphia: Lippincott Williams & Wilkins; 2006. [ Links ]
7. Reilly T, Morris T, Whyte G. The specificity of training prescription and physiological assessment: a review. J Sports Sci. 2009; 27: 575-89. [ Links ]
8. Arboleda S. Convalidación de pruebas y ecuaciones predictivas para la estimación de la capacidad aeróbica: una necesidad del medio colombiano. Actividad física y desarrollo humano. 2006; 3: 65-80. [ Links ]
9. Pérez M. Pruebas funcionales de valoración aeróbica. En: López J. Fisiología del ejercicio. 3a ed. Madrid: Médica Panamericana; 2006. p. 442-70. [ Links ]
10. Zoeller RJ. Gender differences in cardiorespiratory fitness with advancing age: is the age-associated decline in VO2max more rapid in men and do older men and women respond differently to exercise? Am J Lifestyle Med. 2008; 2: 492-9. [ Links ]
11. Stathokostas L, Jacob-Johnson S, Petrella RJ, Paterson DH. Longitudinal changes in aerobic power in older men and women. J Appl Physiol. 2004; 97: 781-9. [ Links ]
12. Hollenberg M, Yang J, Haight TJ, Tager IB. Longitudinal changes in aerobic capacity: implications for concepts of aging. J Gerontol A Biol Sci Med Sci. 2006; 61: 851-8. [ Links ]
13. Fleg JL, Morrell CH, Bos AG, Brant LJ, Talbot LA, Wright JG, et al. Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation. 2005; 112: 674-82. [ Links ]
14. Weiss EP, Spina RJ, Holloszy JO, Ehsani AA. Gender differences in the decline in aerobic capacity and its physiological determinants during the later decades of life. J Appl Physiol. 2006; 101: 938-44. [ Links ]
15. Paterson DH, Govindasamy D, Vidmar M, Cunningham DA, Koval JJ. Longitudinal study of determinants of dependence in an elderly population. J Am Geriatr Soc. 2004; 52: 1632-8. [ Links ]
16. Eskurza I, Donato AJ, Moreau KL, Seals DR, Tanaka H. Changes in maximal aerobic capacity with age in endurancetrained women: 7-yr follow-up. J Appl Physiol. 2002; 92: 2303-8. [ Links ]
17. Kenny GP, Yardley JE, Martineau L, Jay O. Physical work capacity in older adults: implications for the aging worker. Am J Ind Med. 2008; 51: 610-25. [ Links ]
18. Pimentel AE, Gentile CL, Tanaka H, Seals DR, Gates PE. Greater rate of decline in maximal aerobic capacity with age in endurance-trained than in sedentary men. J Appl Physiol. 2003; 94: 2406-13. [ Links ]
19. Wilson TM, Tanaka H. Meta-analysis of the age-associated decline in maximal aerobic capacity in men: relation to training status. Am J Physiol Heart Circ Physiol. 2000; 278: H829-34. [ Links ]
20. Fitzgerald MD, Tanaka H, Tran ZV, Seals DR. Age-related declines in maximal aerobic capacity in regularly exercising vs. sedentary women: a meta-analysis. J Appl Physiol. 1997; 83: 160-5. [ Links ]
21. Tanaka H, Desouza CA, Jones PP, Stevenson ET, Davy KP, Seals DR. Greater rate of decline in maximal aerobic capacity with age in physically active vs. sedentary healthy women. J Appl Physiol. 1997; 83: 1947-53. [ Links ]
22. Shephard RJ. Maximal oxygen intake and independence in old age. Br J Sports Med. 2009; 43: 342-6. [ Links ]
24. Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009; 301: 2024-35. [ Links ]
24. Zakariás G, Petrekanits M, Laukkanen R. Validity of a 2-km Walk Test in predicting the maximal oxygen uptake in moderately active Hungarian men. Euro J Sport Sci. 2003; 3: 1-8 [ Links ]
25. Díaz D, Valbuena L, Pérez J, Cardona, O. Correlación entre la ergoespirometria y la prueba de los 2000 metros. Rev Ant Med Dep. 2000; 3: 17-20. [ Links ]

