










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombia Médica
On-line version ISSN 1657-9534
Colomb. Med. vol.42 no.3 Cali July/Sept. 2011
Levels of physical activity, barriers, and stage of change in an urban population from a municipality in Colombia
Elkin Fernando Arango, MD1, Fredy Alonso Patiño, MSc2, Mario Andrés Quintero, MD3, Mónica María Arenas, MSc4
1. Professor, Instituto de Educación Física, Universidad de Antioquia, Medellín, Colombia. e-mail: elkinarango@yahoo.com
2. Assistant Professor, Instituto de Educación Física, Universidad de Antioquia, Medellín, Colombia. e-mail: fredpa18@hotmail.com
3. Medicine Advisor, Sports and Recreation Institute of the Department of Antioquia (INDEPORTES Antioquia), Medellín, Colombia. e-mail: mquint@une.net.co
4. «Por su salud, muévase pues» Program Coordinator, INDEPORTES Antioquia, Medellín, Colombia. e-mail: monicamaria41@hotmail.com.
Received for publication October 25, 2010 Accepted for publication April 17, 2011
SUMMARY
Objective: To assess the levels of physical activity, barriers, and stage of change in an urban population 25 to 50 years of age from the Municipality of Santa Rosa de Osos, department of Antioquia.
Materials and methods: A prevalence study was conducted, with a two-stage random sampling among 357 individuals not suffering from any known cardiovascular disease. A pre-designed survey was conducted to assess the levels of physical activity, the stage of change, and physical activity barriers.
Results: The total low physical activity was 9%, and by domains: work 66.9%, transport 60.8%, household and garden (yard work) 44.8%, and leisure-time 76.2%. The most important physical activity barriers were «lack of willpower» (70%) and «lack of time» (46.2%). The most prevalent stages of change were «contemplation» (40.3%) and «preparation» (17.1%).
Conclusion: low physical activity levels were found in different domains of daily life, together with a high prevalence of barriers and stages prior to physical activity practice, mainly among women and obese subjects.
Keywords: Physical activity; Physical exercise; Health promotion; Prevalence; Chronic diseases; Colombia.
Colomb Med. 2011; 42: 352-61
Niveles de actividad física, barreras y estados de cambio en una población urbana de un municipio de Colombia
RESUMEN
Objetivo: Evaluar el nivel de actividad física, barreras y estados de cambio, en la población urbana entre 25 y 50 años de edad del municipio de Santa Rosa de Osos, Antioquia.
Materiales y métodos: Se realizó un estudio de prevalencia, con muestreo aleatorio bietápico en 357 personas sin enfermedad cardiovascular conocida; se administró una encuesta prediseñada para evaluar los niveles de actividad física, los estados de cambio y las barreras para la práctica de la actividad física.
Resultados: La actividad física baja total fue del 9% y por ámbitos: trabajo 66.9%; transporte 60.8%; hogar 44.8% y tiempo libre 76.2%. Las barreras más relevantes para la práctica de la actividad física fueron la «carencia de voluntad» (70%) y la falta de tiempo (46.2%). Los estados de cambio más prevalentes fueron el «contemplativo» (40.3%) y el de «preparación» (17.1%).
Conclusión: Se encontraron niveles de actividad física baja en los diferentes ámbitos de la vida diaria, acompañados de una prevalencia alta de las barreras y de los estados previos a la práctica de la actividad física, principalmente en las mujeres y las personas obesas.
Palabras clave: Actividad física; Ejercicio físico; Promoción de la salud; Prevalencia; Enfermedades crónicas; Colombia.
Colomb Med. 2011; 42: 352-61
The 2002 World Health Report, published by the World Health Organization (WHO), estimated that a sedentary lifestyle constitutes one of the 10 leading causes of mortality and disability. Furthermore, it indicated that 76% of all deaths in the American continent were due to non-communicable diseases (NCDs), and that the population proportion whose health is at risk by a sedentary lifestyle is near to 60%1. In Colombia, research such as the 2005 National Nutrition Survey (ENSIN 2005)2, the 2007 National Health Survey (ENS 2007)3, and the 2008 Diagnostic Study of Global Cardiovascular Risk in Medellin4 showed that the prevalence of low physical activity ranges from 42.6% to 67.7%.
Several studies have demonstrated that physical activity (PA) and exercise were useful tools for controlling the risk factors for heart disease, a phenomenon that was proven by Morris5 in England half a century ago. Despite these benefits, there has been an increase in sedentary lifestyle in different populations, which has been defined mainly according to PA levels during leisure-time, without considering other domains of daily life such as transport, household, and work. Likewise, there are difficulties in making people increase their PA levels, this is due in part to disinformation about the factors that determine the beginning and maintenance of a physically active life. Therefore, it is necessary to assess physical activity in particular communities. This permits guiding interventions tending to increase its practice according to each population's own characteristics.
The objective of this study was to determine the characteristics of physical activity practice in different domains of daily life, the barriers and stage of change in a population 25 to 50 years of age from the urban area of the municipality of Santa Rosa de Osos (department of Antioquia).
MATERIALS AND METHODS
Type of study, population, and sampling design. A cross-sectional study was conducted in a population aged 25 to 50 years living in the urban area of the municipality of Santa Rosa de Osos (department of Antioquia). According to the 2005 Colombian General Census, the total population in that municipality was 31,028 people - 10,665 of them between this age range, and approximately 50% were living in the urban area6.
The sample size was calculated with a 50% probability, given the absence of a previous study on the occurrence of the phenomenon studied in the municipality of Santa Rosa de Osos. A population (N) of 5,300 individuals was recruited, with a 95% confidence level, less than 5% significance, 5% maximum allowable error (E=5%), and 95% power. The sample size (n=358 individuals) was increased by 10%, to foresee possible losses during the development of the research, leaving a final sample of 394 subjects.
Sampling. A two-stage stratified probability sampling was carried out. It was stratified by neighborhoods, according to the population proportion in each of them. First stage: homes in each neighborhood were chosen by simple random sampling (SRS). Second stage: A person in each home was selected by SRS, taking into account that if there resided a single person who fulfilled the inclusion criteria, that person was taken as an analysis unit; if there was no individual fulfilling such criteria, a new home was selected according to the description above; if there were two or more individuals fulfilling the criteria, only one was selected. The information provided by the Secretariat of Municipal Planning -which reported 39 neighborhoods and 3,991 homes in the urban area- was used for the sampling design.
Inclusion and exclusion criteria. Men and women aged 25 to 50 years who had been living in the urban area during the last 3 years and accepted to participate after having signed the written informed consent were included. Subjects with sensory, cognitive, and motor impairment, along with those suffering a psychiatric disorder or an established cardiovascular disease and pregnant women were excluded.
Bias control and data quality. Information biases were controlled by training the pollsters on the use of data collection instruments and also on their standardized processing. Quality control of the formats processed during the fieldwork was carried out, returning to the pollster those that had presented inconsistencies or missing data. Participants were explained the objectives of the study and the procedures performed; the privacy of the data provided was guaranteed. A pilot trial was conducted to know the possible difficulties during the implementation of the instrument and also to know how long its processing would take. To control selection bias, a random and representative sample of the study population was obtained with a known sampling frame.
Instruments and collection of information. Information was obtained through the application of a pre-designed survey containing the following items:
Socio-demographic aspects. Age, gender, socioeconomic level, marital status, education level (low: no education or elementary school; medium: high school; high: technical, technological and college), occupation, and affiliation to the Social Security System for Health.
Physical activity. It was assessed by using the International Physical Activity Questionnaire (IPAQ) long form7; frequency (sessions per week), volume (minutes per week), and intensity (moderate and vigorous) of PA were obtained as a whole and for the household, work, leisure-time, and transport domains; METs (metabolic equivalents) expended per week were calculated for each of these items. Subjects were categorized into three groups:
- High Physical Activity (at least 3 days of vigorous-intensity PA of at least 1500 MET-minutes/week, or 7 or more days of any combination of PA of at least 3000 MET-minute s/week).
- Moderate Physical Activity (3 or more days of vigorous-intensity PA of at least 20 minutes per day, or 5 or more days of moderate -intensity PA and/or walking of at least 30 minutes per day, or 5 or more days of any combination of PA of at least 600 MET-minutes/week), and
- Low Physical Activity (criteria for high and moderate categories were not fulfilled).
Barriers to the practice of physical activity. The Barriers-to-Being-Active Quiz was used8, which consists of 21 items and 7 categories («lack of time», «social influence», «lack of energy», «lack of willpower», «fear of injury», «lack of skill», and «lack of resources»).
Stage of change. Stage of Change was assessed by the Physical Activity Practice in Leisure-Time Questionnaire8, which consists of one question and 6 response options, mutually exclusive. Subjects were classified as: «pre-contemplation» (do not perform any PA and have no intention of doing so within the next six months), «contemplation» (do not perform any PA, but have the intention of doing so within the next six months), «preparation» (do not perform any PA, but have the intention of doing so within the next 30 days), «action» (have performed regular PA for less than six months), «maintenance» (have performed regular PA for more than six months, and «relapse» (performed PA regularly, but abandoned it recently.)
Physical evaluation. Weight and height were taken. Measuring equipments were calibrated and checked; an HD327 digital scale and a Seca Bodymeter 208 were used. A body mass index (BMI) >30 kg/m2 was defined as obesity.
Statistical analysis. The Kolmogorov-Smirnov test (n>50) was used to assess the normality of the quantitative variables. For the qualitative variables, frequency distribution (proportions), standard error and its confidence intervals were estimated; quantitative variables were summarized by using the mean and the standard deviation. The prevalence of PA levels, barriers, and stage of change were compared according to gender, age (tertiles), education, and obesity by using the Pearson Chi-square test. All analyses were made with an alpha value <0.05 and 95% reliability. The SPSS 15.0 statistical software was used.
Ethical aspects. This research was approved with a low risk qualification granted by the Research Technical Committee of the Institute of Physical Education at Universidad de Antioquia in Medellin, Colombia. Subjects signed the written informed consent, which took into account the Helsinki Declaration - Ethical Principles for Medical Research Involving Human Subjects - and the provisions of Resolution 08430 of 1993 from the Ministry of Health of the Republic of Colombia. Research results were returned to the participants involved and the cooperating institutions.
RESULTS
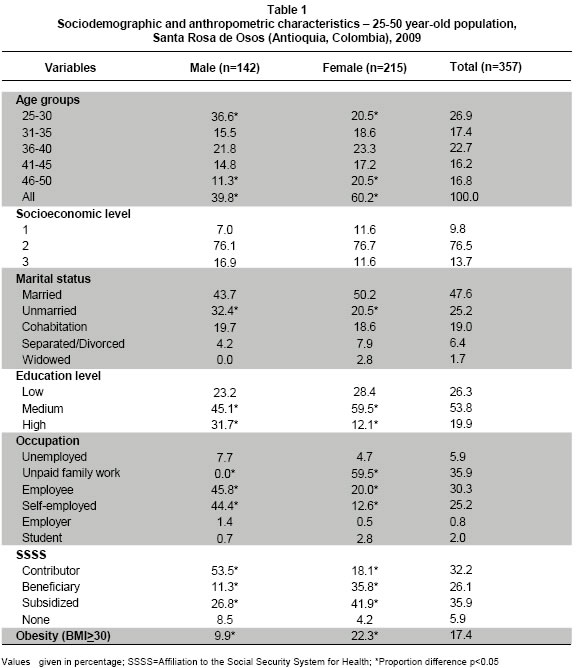
Socio-demographic characteristics and obesity. Six of 10 individuals (60.2%) were women, the average age was 36.9 years old (7.5 SD), and the age groups most represented in the sample were 25-30 (26.9%) and 3640 years of age (22.7%). Some 76.5% of them belonged to socioeconomic level 2, 47.6% of them were married, one-fifth (19.9%) had a high education level, 35.9% with an unpaid family work, and just over one-third (35.9%) was affiliated to the subsidized health insurance program. A BMI >30 kg/m2 was found in 17.4%. When stratifying by gender, the age group 25-30 years showed a higher proportion of men, whereas in the higher age range groups women were prevalent. Being unmarried was more frequent in men. Medium education level was reported most by women, and high education level by men. Regarding occupation, a higher proportion of women were dedicated to unpaid family (household) work, which is in contrast to a higher participation of men in work activities as employees or self-employed workers. A greater number of men were affiliated to the Social Security System for Health as contributors, while women were affiliated mainly as beneficiaries or subsidized (Table 1).
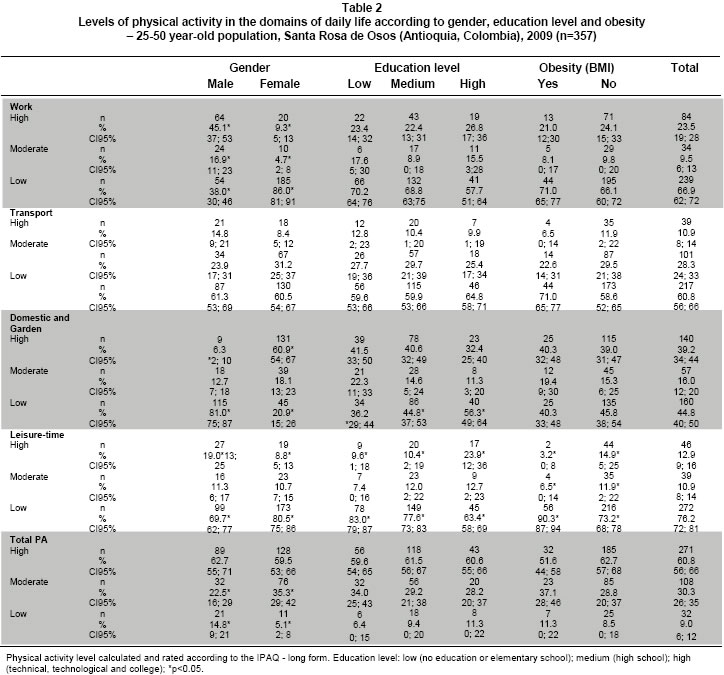
Levels of PA in the domains of daily life. A greater proportion of men with a high level of PA was found in work, transport, and leisure-time domains, whereas women presented it only in the household and garden domain; in the total high PA there were no differences when stratifying by gender. Regarding level of education, an inverse relation with high PA practice in the household domain was found, ranging from 41.5% in less educated people to 32.4% in those with high education levels. On the contrary, in low PA levels, those with a higher education level reported less PA in the household domain. High PA in leisure-time showeda direct relation with level of education, whereas in low PA this relation was inversed. There were no significant differences in PA levels in transport domain and total PA when stratifying by level of education. Obese individuals reported lower high and moderate PA levels and a greater proportion of low PA in leisure-time than those not suffering from obesity (p<0.05); in transport, similar tendencies were found without reaching statistical significance (Table 2).
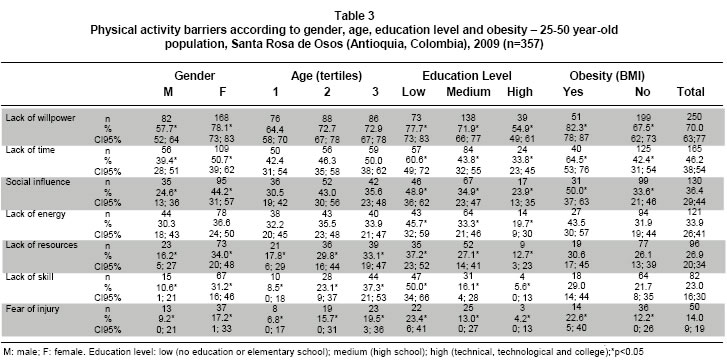
Perception of PA barriers. The most important PA barriers were «lack of willpower» (70%) and «lack of time» (46.2%). Women reported higher barrier values, and these differences were statistically significant, except for «lack of energy». As age increased, the barrier perception was greater - this relation was not found in «lack of willpower» and «social influence». Differences were significant in «lack of resources», «lack of skill», and «fear of injury» (p<0.05). There was an inverse relation between level of education and barriers (p<0.05). Obese individuals reported a greater barrier perception of which the differences among «lack of willpower», «lack of time», «social influence» and «fear of injury» were statistically significant (p<0.05) (Table 3).
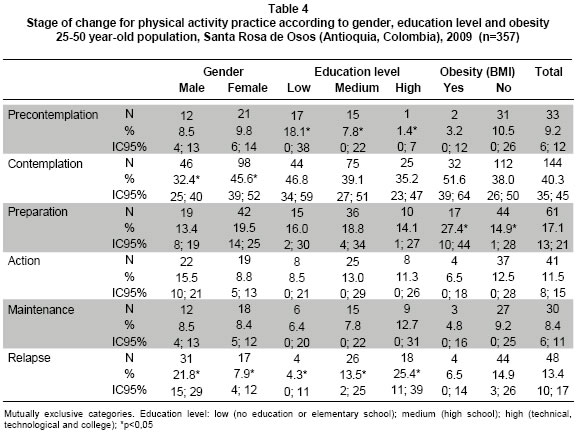
Stage of change for physical activity practice. The most prevalent stage of change was «contemplation» (40.3%), followed by «preparation» (17.1%); only 19.9% of the individuals reported the «action» and «maintenance» stages (physically active people). Statistically significant differences in proportions were found when stratifying by gender in «contemplation» and «relapse» stages; by education level in «pre-contemplation» and «relapse» stages; and among obese individuals in the «preparation» stage (Table 4).
DISCUSSION
The proportion of individuals reporting total low PA was 9% - a lower value than those referenced in some population studies made in Colombia: Medellin4 51.6% (IPAQ-long form), 2005 National Nutrition Survey (ENSIN 2005)2 57.4% (IPAQ-long form), and 2007 National Health Survey (ENS 2007)3 79% (leisure-time). These differences can be explained by: 1. the type of instrument used to assess the PA levels; 2. the qualification method used by the instrument in each study, and 3. each population's own characteristics. It must be taken into account that Santa Rosa de Osos is a village where the characteristics of work (agriculture and dairy cattle) and transport inside the urban area (walking or bicycling) demand physical activities with high calorie expenditures, while in a city like Medellin, sedentary working activities predominate, and transport is usually done in motor vehicles. When comparing the levels of total PA in Santa Rosa de Osos (60.8% high PA; 30.3% moderate PA; 9% low PA) with those reported by Bauman in a prevalence study on physical activity in 20 countries (IPAQ was used), it is found that these values are similar to those from the samples obtained from China, the Czech Republic, Lithuania, New Zealand, the United States, and Colombia, where high PA varied from 52.1% to 63.1%, moderate PA from 22.1% to 35.4%, and low PA from 6.9% to 17.2%9.
When only leisure-time is taken into account, a similarity was found between the low PA levels in Santa Rosa de Osos and those in the ENS 2007 (76.2% vs. 79%); this shows that people are less physically active in this domain. These values are higher than those reported in the United Stated and Teusaquillo (Colombia), where around 60.0% of adults do not perform any PA in leisure-time10,11, and lower than the ones reported in Brazil (87%)12.
In work domain, high PA was found in one out of 4 individuals in Santa Rosa de Osos, as well as in Teusaquillo11 (23.5% vs. 27.9%), and low PA was the most prevalent in both places and in the ENSIN 20052 (66.9%, 55.4%, and 79.9%, respectively). High PA in the domestic and garden domain was greater in Santa Rosa de Osos (39.2%) than in Teusaquillo (26.3%) - an opposite result to that found in low PA (44.8% vs. 53.6%)11. In the transport domain, PA levels were similar in both studies; low PA was 60% in Santa Rosa de Osos, as well as in Teusaquillo11, and high PA was close to 10%.
The prevalence rates of the PA levels in the different domains are similar to those reported in the literature, where men refer greater high PA levels in work, transport, and leisure-time domains, whereas women do this especially in the household and garden domain2,11,12. In this study, when stratifying by gender, there were no differences in the total high PA levels, while the moderate PA was greater among women (35.3% vs. 22.5%) and the low PA was greater among men (14.8% vs. 5.1%). All these can be explained by the kind of occupation they have. Women are mainly engaged in household tasks; while men work do not work at home. This situation forces them to use means of transport like bicycling and walking. Moreover, the kind of work (agriculture and dairy cattle) implies energy expenditure higher than that made by their female counterparts. It is possible that the lower participation of women in PA during leisure-time is due to a lower childhood stimulus for this practice and to being especially engaged in housekeeping and raising children.
Education level seems to affect the level of PA in the domestic and leisure-time domains. In high PA, an inverse relation in the domestic domain is present, i.e., lower high PA at higher education; while in the leisure-time domain there is a direct relation - higher high PA at higher education. People who have studied more years in formal education reported a greater prevalence of low PA in the domestic domain and less low PA during the leisure-time. These results agree with those reported in Teusaquillo and Guarne (Colombia)11,13.
Among obese individuals, the low PA level during leisure-time was higher than in subjects without this condition (73.2% vs. 63.4%), and although the high PA level had the lowest prevalence both in obese and nonobese individuals (3.2% vs. 14.9%) it interesting to note the very low participation of obese subjects in high-intensity physical activities. When comparing these results with literature reports, they are similar to data produced by cross-sectional studies, but in longitudinal studies there is still some controversy, given there is no universal agreement on whether obesity is a cause or effect of low levels of PA14. In a cross-sectional study was carried out in Finland, protective associations of the level of PA and the obesity risk were reported for both genders, with Odds Ratios (ORs) varying from 0.78 to 0.82 for moderate PA in men; from 0.59 to 0.65 in women; in high PA the ORs were from 0.42 to 0.47 in men; among women from 0.31 to 0.39; all of them with statistical significance15.
«Lack of willpower» and «lack of time» were the main reported barriers for not performing PA during leisure-time. Mantilla's study11 in a location of Bogotá (Colombia) revealed the same results. «Lack of time» for PA practice is one of the main barriers reported in literature, with prevalence rates ranging from 24.4% to 67.9%, this variability probably depends on each population's own characteristics and on the different data collection instruments, but this places it as a major obstacle to overcome in order to achieve a more active lifestyle13,16-19. It is remarkable, in this work, that women showed higher values in the different barriers, which hinders their participation in these kinds of activities. A similar situation was present in a study among college students in Chile16.
In this study, a higher perception of barriers was found when age increased, mainly in «lack of resources», «fear of injury», and «lack of skill»; when comparing with the studies carried out in Newcastle and Madrid, «lack of equipment», «money», and «resources» occurred more in young people; «getting injured» and «health problems» were more frequent among older people17,18. Concerning the «lack of skill» barrier, there were no data reported in these studies; nevertheless, the literature shows a loss of motor performance and of the capacity to learn new skills when age increases, hence, it is necessary to implement less-complex physical activities for older individuals to facilitate their adherence to the practice20.
Having a higher level of education was related to a lower perception of PA barriers; in a study carried out in Newcastle, «lack of time» and «lack of motivation» were more prevalent at the college level, while «lack of money» and «presence of disease» were more prevalent at the basic level18.
Obese subjects reported a greater proportion in barrier perception, mainly in «lack of willpower», «lack of time», «social influence», and «fear of injury». When comparing with a study carried out in the US among women 40 to 64 years of age, «lack of time» was more frequent among those who reported normal weight and «lack of willpower» was higher among people suffering obesity21. In another study (women 25 to 70 years of age), obese participants reported a higher «lack of motivation» as a PA barrier than did normal-weight subjects (63% vs. 31%)22.
Regarding the stage of change for PA practice in leisure-time, the «contemplation» stage was the most recurrent (40%), a higher value than the one reported by Gómez23 in Bogotá (24%), Mantilla11 in Teusaquillo (28.4%), Dumith24 in Brazil (13%), and Garber25 in Rhode Island (9%); this is in contrast to the «maintenance» stage, whose proportion in Santa Rosa de Osos (8.4%) was lower than in these studies. When comparing by gender, women reported a higher frequency in the «contemplation» stage - a tendency similar to that in other research16,24. In the stage of change regarding the level of education, statistically significant differences were found in «pre-contemplation», where individuals with less education reported a greater proportion of this stage. This tendency was repeated in the «contemplation» stage, even though it did not reach statistical significance; these data are similar to those from the study in Brazil24. The «relapse» stage had a direct relation with education level, i.e., individuals with greater education referred a higher PA desertion. Stages prior to action were more frequent in people suffering obesity, similar to what Dumith reported24. This might mean that this condition encourages thinking about starting a PA plan to control and diminish body weight; however, the «action» and «maintenance» stages are lower among obese individuals, this can be related to the «lack of willpower» for performing PA. Being the stage of change an estimator for PA practice in leisure-time, the low report of the «action» and «maintenance» stages confirms the low PA level reported through the IPAQ in this dimension.
This study presented the following limitations:
- difficulties in the subject selection at home: when there were two or more subjects fulfilling the inclusion criteria, some of them refused to participate in the randomization process;
- difficulties in accessing men, given their occupations and their lack of willingness to participate in the study, which caused the sample to be represented by four men for every six women;
- the use of the barriers and stage of change tests, even though they are instruments that provide relevant information about the PA in the population, they are not validated in our context. These instruments were used in this study to compare the results obtained to those reported in research conducted in other populations of Colombia and Latin America;
- the IPAQ instrument tends to overestimate the PA levels; this may lead to bias in the total prevalence estimates and by domains. Likewise, the IPAQ does not have a specific validation in Colombia, but the construction and validation of this instrument was carried out in 12 countries with a trans-cultural character; hence, the WHO recommends it to study the prevalence of physical activity levels, both within the national and regional scopes;
- differences in PA levels, barriers and stage of change found among people suffering obesity (Yes/No) were not adjusted by gender because the results lose power because the sample size was calculated to carry out a prevalence study and the adjustment levels were not considered from the beginning of the study.
In conclusion, in the population aged 25 to 50 years from the municipality of Santa Rosa de Osos, department Antioquia, the total high PA was the most prevalent; nevertheless, when stratifying by domains, these proportions decreased significantly. It was found that women are more active in the domestic domain, whereas men are more active during leisure-time, work, and transport; a high PA during leisure-time corresponded to a higher level of education and to a lower obesity prevalence. Furthermore, there was a high prevalence of the PA barriers perceived by people, where «lack of willpower», «lack of time», and «social influence» are significant. This affected in greater proportion of women, subjects with lower education levels, and obese individuals. Being older was related to an increase in the frequency of the «lack of resources», «lack of skill», and «fear of injury» barriers. Stage of change prior to action predominated («contemplation» and «preparation»), mainly among women and those suffering obesity; «maintenance» and «relapse» stages were mainly reported by individuals who have studied more years, and «pre-contemplation» by those who have studied less.
These findings permit suggesting both individual and collective actions that lessen the barriers to increase the levels of physical activity practice in the different domains of daily life, especially in women and obese individuals who referred to finding themselves in the «contemplation» and «preparation» stages of change.
If the barriers reported by the population studied are not intervened, the low PA practice during leisure-time might increase its prevalence in the coming years. Thus, the analysis of the barriers that hinder the PA practice is an essential step before planning any strategy to increase the motivation and adherence to an active lifestyle.
ACKNOWLEDGEMENTS
The authors thank the Committee for the Development of Research (CODI) and the Direction of Regionalization at Universidad de Antioquia, the Sports and Recreation Institute of the department of Antioquia (INDEPORTES Antioquia), and the Hospital San Juan de Dios in the municipality of Santa Rosa de Osos - their contributions funded this project.
Conflict of interest. The authors declare having no conflict of interest related to this study.
REFERENCES
1. Organización Mundial de la Salud. Informe sobre la salud en el mundo 2002. Reducir los riesgos y promover una vida sana. Available at: http://www.who.int/whr/2002/es/ Accessed 6 January 2008. [ Links ]
2. ICBF, Profamilia, Instituto Nacional de Salud, Universidad de Antioquia, OPS. Encuesta Nacional de la situación nutricional en Colombia (ENSIN). Bogotá; 2005. [ Links ]
3. Ministerio de Protección Social. Encuesta Nacional de Salud. ENS 2007. Available at: http://www.minproteccionsocial.gov.co/VBeContent/library/documents/DocNewsNo18358DocumentNo9089.PDF. Accessed 10 April 2010. [ Links ]
4. Secretaria de Salud de Medellín. Diagnóstico del riesgo cardiovascular global, evaluación de su impacto poblacional, Medellín y sus corregimientos 2007-2008. Available at: http://www.medellin.gov.co/irj/go/km/docs/AlcaldiaMedellin/SecretariaSalud/SitioTemporalSalud/descargables/EstudiosEInvestigaciones/Diagnostico_%20riesgo_%20cardiovascular_Medellin_%202007_2008.pdf. Accessed 20 October 2009. [ Links ]
5. Morris JN, Crawford MD. Coronary heart disease and physical activity of work; evidence of a national necropsy survey. Br Med J. 1958; 2: 1485-96. [ Links ]
6. Departamento Administrativo Nacional de Estadísticas. Censo Colombia 2005. Available at: http://www.dane.gov.co/index.php?Itemid=750&id=269&option=com_content§ionid=16&task=category. Accessed 15 May 2008. [ Links ]
7. IPAQ Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire - Short and Long Forms. Available at: http://www.ipaq.ki.se/scoring.pdf. Accessed 20 May 2008. [ Links ]
8. CDC-USDHHS, ed. Promoting physical activity. A guide for community action. USA: Human Kinetics; 1999. [ Links ]
9. Bauman A, Bull F, Chey T, Craig CL, Ainsworth BE, Sallis JF, et al. The International Prevalence Study on Physical Activity: results from 20 countries. Int J Behav Nutr Phys Act. 2009; 6: 21. [ Links ]
10. Schoenborn CA, Adams PF, Barnes PM. Body weight status of adults: United States, 1997-98. Adv Data. 2002; 330: 1-15. [ Links ]
11. Mantilla S. Actividad física en habitantes de 15 a 49 años de una localidad de Bogotá, Colombia, 2004. Rev Salud Publica. 2006; 8 (Supl. 2): 69-80. [ Links ]
12. Monteiro CA, Conde WL, Matsudo SM, Matsudo VR, Bonsenor IM, Lotufo PA. A descriptive epidemiology of leisure-time physical activity in Brazil, 1996-1997. Rev Panam Salud Publica. 2003; 14: 246-54. [ Links ]
13. Castro A, Patiño F, Cardona B, Ochoa V. Aspectos asociados a la actividad física en el tiemplo libre en la población adulta de un municipio antioqueño. Rev Salud Publica. 2008; 10: 679-90. [ Links ]
14. Petersen L, Schnohr P, Sorensen TI. Longitudinal study of the long-term relation between physical activity and obesity in adults. Int J Obes Relat Metab Disord. 2004; 28: 105-12. [ Links ]
15. Lahti-Koski M, Pietinen P, Heliovaara M, Vartiainen E. Associations of body mass index and obesity with physical activity, food choices, alcohol intake, and smoking in the 1982-1997 FINRISK Studies. Am J Clin Nutr. 2002; 75: 809-17. [ Links ]
16. Olivares S, Lera L, Bustos N. Etapas de cambio, beneficios y barreras en actividad física, consumo de frutas y verduras en estudiantes universitarios de Santiago de Chile. Rev Chil Nutr. 2008; 35: 25-35. [ Links ]
17. Rodríguez-RomoI? G, Boned-PascualII C, Garrido-Muñoz M. Motivos y barreras para hacer ejercicio y practicar deportes en Madrid. Rev Panam Salud Publica. 2009; 26: 244-54. [ Links ]
18. Chinn DJ, White M, Harland J, Drinkwater C, Raybould S. Barriers to physical activity and socioeconomic position: implications for health promotion. J Epidemiol Community Health. 1999; 53: 191-2. [ Links ]
19. Seclen-Palacin JA, Jacoby ER. Socio-demographic and environmental factors associated with sports physical activity in the urban population of Perú. Rev Panam Salud Publica. 2003; 14: 255-64. [ Links ]
20. Shea CH, Park JH, Braden HW. Age-related effects in sequential motor learning. Physiol Ther. 2006; 86: 478-88. [ Links ]
21. Rye JA, Rye SL, Tessaro I, Coffindaffer J. Perceived barriers to physical activity according to stage of change and body mass index in the West Virginia wise woman population. Womens Health Issues. 2009; 19: 126-34. [ Links ]
22. Genkinger JM, Jehn ML, Sapun M, Mabry I, Young DR. Does weight status influence perceptions of physical activity barriers among African-American women? Ethn Dis. 2006; 16: 78-84. [ Links ]
23. Cabrera G, Gómez L, Mateus J. Cabrera G, Gómez L, Mateus J.? Actividad física y etapas de cambio comportamental en Bogotá. Colomb Med. 2004; 35: 82-6. [ Links ]
24. Dumith SC, Gigante DP, Domingues MR. Stages of change for physical activity in adults from Southern Brazil: a population-based survey. Int J Behav Nutr Phys Act. 2007; 4: 1-10. [ Links ]
25. Garber CE, Allsworth JE, Marcus BH, Hesser J, Lapane KL. Correlates of the stages of change for physical activity in a population survey. Am J Public Health. 2008; 98: 897-904. [ Links ]

