










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombia Médica
On-line version ISSN 1657-9534
Colomb. Med. vol.43 no.1 Cali Jan./Mar. 2012
Salivary cortisol levels as a predictor of preeclampsia in adolescents Niveles de cortisol salivario como predictor de preeclampsia en adolescentes Jaime Salvador-Moysén, MD1, José M. Ramírez-Aranda, MD2, 1Professor researcher, Scientific Research Institute, Universidad Juárez del Estado de Durango, Durango, México. e-mail: jsmoysen@gmail.com Received for publication January 26, 2011 Accepted for publication July 15, 2011 Summary
Yolanda Martínez-López, ScD,1*, Marisela Aguilar-Durán, MSc1**
1*Professor researcher, Scientific Research Institute, Universidad Juárez del Estado de Durango, Durango, México. e-mail:ymtzlopez@gmail.com
1**Professor researcher, Scientific Research Institute, Universidad Juárez del Estado de Durango, Durango, México. e-mail:aguilarduran_marisela@hotmail.com
2 Professor researcher, Department of Family Medicine, Hospital Universitario Dr. José Eleuterio González, Universidad Autónoma de Nuevo León, Monterrey, México. e-mail: rmz544383@yahoo.com.mx
Methods: We carried out a nested case-control study. Somatometric, clinical, and biochemical data were obtained from 100 healthy pregnant adolescents and salivary cortisol was measured at 8:00, 12:00, and 20:00 hours on two occasions during pregnancy, before 20 weeks, and after 30 weeks of gestation. The cortisol values between the group of healthy pregnant women and the group that developed preeclampsia were compared by using the Student's t, MannWhitney, and Wilcoxon tests. Also, the ROC curve of cortisol values and the Positive and Negative Predictive values of cortisol were estimated.
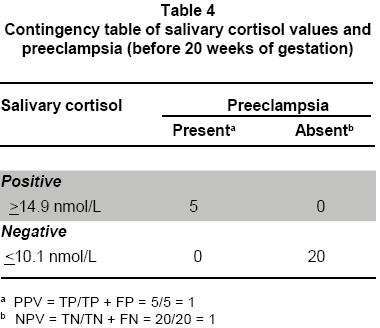
Results: Values >14.9 nmol/L of cortisol were observed in the group that developed preeclampsia, providing a positive predictive value of 1 (100%). Values <10.1 nmol/L were observed in the control group, the negative predictive value was 1 (100%). The cutoff point of the ROC curve -before 20 weeks of gestationin the members of the cohort was 13.9 nmol/L.
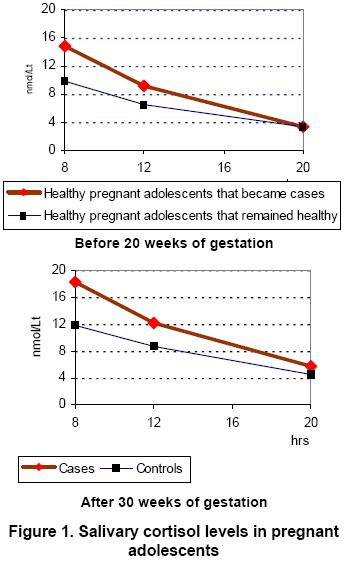
Conclusions: The salivary cortisol values observed in the two evaluations made to each of the groups showed statistically significant differences between the groups at 8 and 12 hours of the day. The values obtained enable establishing gradients that allow separating the group of healthy women that got ill with preeclampsia from the group that did not develop the illness before week 20. After week 30, the cortisol gradients are established more clearly in the group with preeclampsia and in the control group. The validation of these findings in larger samples would allow implementing this procedure as a screening test for preeclampsia in groups of pregnant adolescents.
Keywords: Pregnancy in Adolescence; Pre-Eclampsia; Physiological Stress; Salivary cortisol.
Resumen
Objetivo: Determinar la utilidad del cortisol salivario como un predictor de preeclampsia en adolescentes.Métodos: Se realizó un estudio de casos y controles anidado en una cohorte.Se obtuvieron datos somatométricos, clínicos y bioquímicos, de un grupo de 100 mujeres adolescentes, embarazadas y sanas. Se les cuantificó cortisol salivario a las 8:00, 12:00 y 20:00 h en dos ocasiones durante el desarrollo de su proceso gestacional, antes de la semana 20 y después de la semana 30. Los valores de cortisol obtenidos, tanto en el grupo de mujeres que permanecieron sanas, como en el que desarrolló preeclampsia, se compararon empleando las pruebas t de Student, Mann-Whitnney y Wilcoxon; también se estimaron los valores predictivos y la curva ROC para los valores de cortisol.
Resultados: El grupo que se convirtió en casos presentó valores de cortisol >14.9 nmol/L con un valor predictivo de 1 (100%) en relación con la ocurrencia de preeclampsia; el grupo que fue seleccionado como control tuvo valores de cortisol <10.1 nmol/L con un valor predictivo de 1 (100%) en relación con la no ocurrencia de preeclampsia. El punto de corte identificado -antes de la semana gestacional 20en la curva ROC para las integrantes de toda la cohorte fue 13.9 nmol/L.
Conclusiones: Los valores de cortisol salivario, que se obtuvieron en las dos evaluaciones realizadas a las integrantes de cada uno de los grupos, mostró diferencias estadísticamente significativas intergrupales a las 8:00 y 12:00 h del día. Los valores obtenidos permiten establecer gradientes que separan antes de la semana 20, al grupo de mujeres saludables que desarrollaron un cuadro de preeclampsia del grupo de mujeres que no presentaron la enfermedad. Después de la semana 30 los gradientes de cortisol entre el grupo con preeclampsia y el grupo control se definen más nítidamente. La validación de estos hallazgos en muestras poblacionales mayores permitirá la implementación de este procedimiento como una prueba de tamizaje aplicable a grupos de adolescentes embarazadas.
Palabras clave. Embarazo en adolescentes; Pre-eclampsia; Estrés fisiológico; Cortisol salivario.
Toxemias of pregnancy represent some of the most relevant problems in reproductive health. Preeclampsia is a hypertensive disorder that affects 3% to 10% of pregnancies and causes 15 to 20% of deaths related to reproduction in developed countries; it is also the number one cause of maternal death in developing countries and an important cause of perinatal death, preterm birth, and intrauterine growth restriction1-3The etiology of toxemia of pregnancy is unknown, despite the large amount of research carried out on the subject. One of the reasons that can explain this is the lack of studies incorporating relevant findings from different cognitive fields to explain the origin of the disease. For example, the epidemiological findings associated with the disease are not usually considered in the research from a clinical point of view. Also, the clinical and molecular evidence related with the toxemias are not incorporated in the epidemiological designs4-7.
Another explanation derives from the absence of a guideline that links the socio-epidemiological variables of vulnerable population groups (low educational levels, unstable family economy, low social support) with the clinical and biochemical aspects of the disease, which has limited the construction of a general principle to explain the genesis of this health problem. It is important to mention that it has been documented that psychological stress and psychosocial stress have both been associated with preeclampsia in women from different social and geographic settings8-12. From this perspective, the concept of stress is operationally defined as: a psychobiological process mediator, whose physiological, biochemical, and molecular levels are the translation of the individual's organic response to stimuli from various socio-cultural environments they perceive as threatening9. According to this evidence, we can hypothetically say that high levels of psychological and psychosocial stress will necessarily appear in the biochemical aspect. If this hypothesis is valid, it will lead to new paths to solving this millennial health problem.
The main purpose of this study was to evaluate salivary cortisol as a positive, as well as a negative, predictor of preeclampsia13 in pregnant adolescents. Also, to biologically establish through cortisolthe findings reported in literature that establish the association of psychological and psychosocial stress with the occurrence of preeclampsia. The selection of cortisol was based on information documented to measure stress conditions in different population groups14-16.
Materials and methods
Study participants.A cohort of 100 healthy pregnant adolescents was formed to evaluate the predictive capacity of cortisol as an early indicator of preeclampsia. We designed a nested case-control study to reach this goal. The participants were recruited from two settings; institutional and community. The inclusion criteria were: 1) age 15 to 20 years (The upper age limit was 20 years old because the lack of personal economic and solvency and autonomy were attributes shared within the group of adolescent women and, for this study purpose, this condition was more important than chronological age); 2) gestation of <20 weeks; 3) adolescent with up to 3 pregnancies; 4) voluntarily and informed participation in the study. The exclusion criterion was pregnant adolescents with a history of metabolic and/or vascular processes. The definition of preeclampsia was: systolic blood pressure >140 mm Hg or diastolic blood pressure > 90 mm Hg, and proteinuria >300 mg/urine of 24 hours.
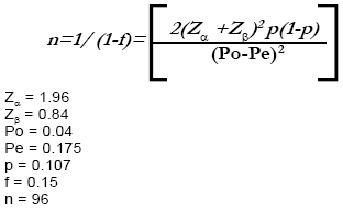
The sample size was calculated by using a formula applicable to cohort studies17:
Procedure. The first evaluation was carried out on gestational week 15 on average and the second on week 32 on average. Somatometric, clinical, and biochemical (cortisol) data were obtained. Calibrated equipment and standardized technique were also used. Socio-demographic data was recorded on the first evaluation.
Recruitment was performed by identifying pregnant adolescents in two Health Clinics of the Ministry of Health of the State of Durango, Mexico. We also included pregnant adolescents from the community by using a census done by the Ministry of Health and the Mexican Social Security Institute from the same city. The evaluations were carried out in an institutional setting, as well as in the community, depending on the place where the pregnant adolescents were recruited. The control group was made up of 20 adolescents (four controls for each case) randomly chosen from the group that did not develop a pathologic process during pregnancy and that had complete somatometric, clinical, and biochemical evaluations in the two gestational stages included in the study design.
Demographic, clinical, and somatometric data. The demographic data collected by interview and recorded in a questionnaire designed for this purpose were: age, marital status, educational level, and occupation. Blood pressure was measured by using two new, portable, calibrated mercury column sphygmomanometers. We followed the recommendations established by the Official Mexican Norm, NOM-030-SSA2-1999, with regard to the observer, the subject, and the surroundings18. Height and weight recordings were made with a new calibrated stadimeter, according to recommendations suggested by the World Health Organization and the Pan American Health Organization19. We calculated mean blood pressure, body mass index (BMI) -before the 20th week of gestationand the expected weight for their height and gestational age19 -after the 30th week of gestation.
Salivary cortisol measurement. Three saliva samples were collected to determine cortisol levels by using a Salivette system (Sarstedt, AG & Co, Nümbrecht, Germany) at three different moments during the same day, 8:00, 12:00, and 20:00 h, before gestational week 20 and on a second occasion after week 30. The samples were centrifuged at 1000 g for 5 min, decanted to preserve the saliva without mucus, and frozen at -20°C until analysis.
The concentration of salivary cortisol was determined by immunoassay on micropla tes (Active®Cortisol EIA, Diagnostic System Laboratories, Inc. Webster, TX). We added 100 µl of enzyme conjugate to 25 µl of each control or standard sample and then covered and mixed them for 10 seconds. Afterwards, 100 µl of cortisol antiserum was added and the samples were incubated at room temperature for 45 min with continuous shaking at 700 rpm. Washings and aspiration were performed for five cycles by using washing buffer with a semiautomatic microplate washer. Thereafter, 100 µl of TBM chromogen solution was added and the samples were incubated at room temperature for 15 min with continuous shaking at 700 rpm. We added 100 µl of stop buffer and determined the cortisol concentration with an ELx800 (Lionheart Diagnostics, Marshall MI.) universal plate reader at 450 nm14
Cortisol readings were performed in blind fashion with regard to the clinical condition of the cohort participants.
Statistical analyses. We analyzed the data with the Student's t, Mann-Whitney, and Wilcoxon tests. A p<0.05 was considered statistically significant. We used Microsoft Excel 2000 for data collection and SPSS version 7.5 for statistical analysis. Also, the ROC curve of cortisol values and the positive and negative predictive values of cortisol were estimated.
Ethical considerations. All cohort participants provided informed consent and the project was approved by the Ethics Committee of the «Dr. José Eleuterio González» University Hospital of Universidad Autónoma de Nuevo León.
Results
Definition of analysis groups was made when all cohort participants ended their pregnancy. Five cases of preeclampsia were diagnosed and confirmed in the gynecology-obstetrics service of the Health Ministry's General Hospital in Durango, Mexico. The controls were 20 adolescents (four for each case) randomly chosen from the group with complete somatometric, clinical, and biochemical evaluations that did not develop preeclampsia.
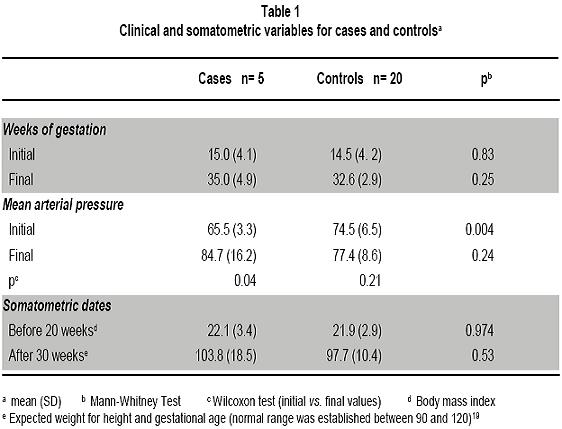
Mean age of the case group was 17 years ±1 SD; while in the control mean age was 17±1.9 SD. Only one participant (20%) was married in the case group and 15 (75%) were either married or had a partner in the control group. The educational level observed was 9 years in cases and 8.2 years in the control group. Four (80%) cases and 14 (70%) controls were housewives; one case (20%) and three (15%) controls were students and only one (15%) control was a worker. The percentage values observed in the control group are very similar to the values obtained in the subjects in the cohort who did not develop preeclampsia and that did not differ significantly from the case group, with the exception of marital status. Average values of mean blood pressure (2DBP+1SBP/3) during both evaluations performed on the case group were 65.5±3.3 SD and 84.7±16.2 SD with a 19 mm Hg increase being observed between the first and second evaluation (for analysis purposes, five adolescents who developed preeclampsia were considered as the case group in the two moments of evaluation before week 20 and after week 30. The same applies to the 20 adolescents in the control group). In the control group, the readings obtained were 74.5 mm Hg±6.5 SD and 77.4±8.6 SD on the first and second evaluation, respectively. The increase observed between both measurements was 2.9 mm Hg. This is 6.5 times less than that observed in the cases.
With regard to the body mass index (BMI), the data recorded during the initial measure (before week 20 of gestation) showed the following average results: cases 22.1±3.4 SD; control group 21.9±2.9 SD; in the second anthropometric measurement, the expected weightfortheirheightandgestational age was estimated19. This represents a more appropriate evaluation after week 20 of pregnancy, observing in the case group a value of 103.8±8.5 SD and in the control group a value of 97.7±10.4 SD -the normal range was established between 90 and 12019(Table 1).
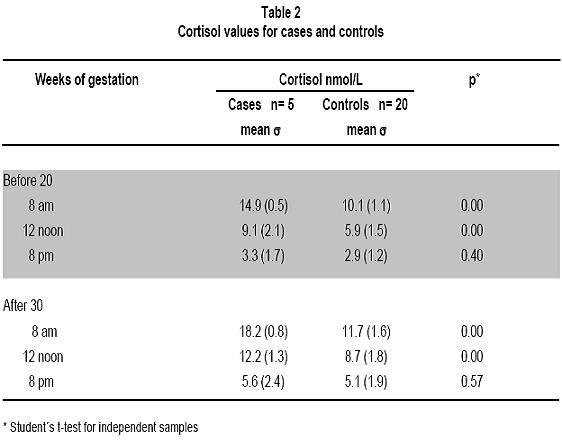
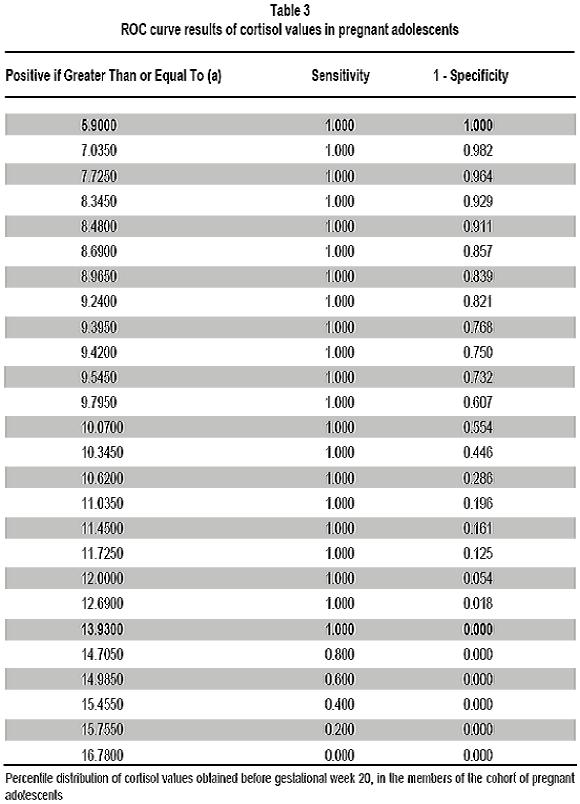
The findings obtained by measuring salivary cortisol (Table 2), (Figure 1) at 8.00 and 12.00 h, at different moments during pregnancy showed statistically significant differences when the case group is compared with controls; the values observed at 20.00 h, were similar in both groups. The cutoff point of the ROC curve -before 20 weeks of gestationin the members of the cohort was 13.9 nmol/L with a 100% of sensitivity and 99% of specifity. The group of participants who did not develop preeclampsia and from which controls were selected is within the range set between 5.9 nmol/L and 13.93 nmol/L. The group of adolescents who developed preeclampsia is exclusively within the range established between 14.9 nmol/L and 16.78 nmol/L (Table3). The positive and negative predictive value of salivary cortisol was 1 (100%) (Table 4).
Discussion
The positive predictive value20 of salivary cortisol with regard to preeclampsia was 1 (100%) with cortisol levels >14.9 nmol/L; with levels <10.1 nmol/ L, the negative predictive value was 1(100%). These results, using salivary cortisol as an indicator of biochemical stress, show epidemiological coherence20, with different authors' observations, in different epidemiological approaches related to the association of psychological and psychosocial stress conditions with toxemias of pregnancy8-12. It is important to mention that evidence is insufficient in scientific publications that validate the cortisol and preeclampsia findings presented herein, such as Sikkema et al.21 who evaluated cortisol levels in a group with preeclampsia patients and compared to a control group. The values observed in affected patients were less than those for the control group, and statistically significant differences were not observed. Something remarkable in the Sikkema et al., work is that, in the case group, the drop in cortisol values during the first evaluation (week 17-18) is abrupt between 8 and 10 h, reducing by almost 40%, contrary to the control group, whose reduction was almost 12%, meaning 3.3 times less. In the second evaluation made in the same study (week 27-28), although observing the same pattern with less magnitude, the curve in the case group loses continuity showing irregularities not observed in the control group; this unusual finding in the circadian behavior of cortisol levels, observed in the group with preeclampsia -clearly showed on graphics by the authorscould have a relevant clinical meaning, associated to stress conditions that, though it was not possible to statistically demonstrate, does not exclude the possibility of alteration of the hypothalamic-pituitary-adrenal system of women with preeclampsia. It is important to note that the average age in the Sikkema et al.21 study was of 30 years; rather, in the work we conducted, the average age of the participants was 17 years, which implies possible different neuroendocrine and metabolic conditions attributable to age. On the other hand, there is evidence of a clear increase in salivary cortisol levels, with statistically significant values, in a group of pregnant women to whom an experimental stressor was applied16.
The rigorous methodology used during the study, as well as to perform the first cortisol measure before the 20th week of pregnancy support the validity of our conclusions, although the reduced number of preeclampsia cases could mean that the conclusions obtained could be preliminary and not definitive although reasonably valid.
Validation of these findings in a larger sample and in different geographical contexts would allow implementing an early screening test -in institutional, as well as community settingsin groups of pregnant adolescents to confidently identify those at risk for preeclampsia.
It is important to carry out studies that include, in articulated and coherent manner, the most important socio-epidemiological, clinical, and biochemical risk factors and indicators documented in the literature that are related to preeclampsia. This new way of approaching the problem would provide a wider and possibly more promising perspective to identify the cause of the disease.
Conflict of interest. None of the authors has conflicts of interest related to this study.
Acknowledgments
The authors would like to thank the financial support from the Council of Science and Technology of the State of Durango (COCyTED), N° 9702076, and the strong commitment of the Scientific Research Institute, Universidad Juárez del Estado de Durango, México. We would also like to recognize the help in statistical review by Sergio Estrada-Martínez MSc. and Edgar Felipe Lares-Bayona MSc.
References
1. Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005; 365: 785-99. [ Links ]
2. Rudra C, Williams M. Monthly variation in preeclampsia prevalence: Washington State, 1987-2001. J Matern Fetal Neonatal Med. 2005; 18: 319-24. [ Links ]
3. World Health Organization. Maternal mortality in 1995. Estimates developed by WHO, UNICEF and UNFPA. WHO/ RHR/01.9. Geneve : World Health Organization, Department of Reproductive Health and Research; 2001. [ Links ]
4. Roberts J, Cooper D. Pathogenesis and genesis and genetics of preeclampsia. Lancet. 2001; 357: 53-6. [ Links ]
5. Luft F. Pieces of the preeclampsia puzzle. Nephrol Dial Transplant. 2003; 18: 2209-10. [ Links ]
6. Redman C, Sargent I. Latest advances in understanding preeclampsia. Science. 2005; 308: 1592-4. [ Links ]
7. Walker J. Pre-eclampsia. Lancet. 2000; 356: 1260-5. [ Links ]
8. Salvador J, Martínez Y, Lechuga A, Terrones A, Ruiz R. Situación psicosocial de las adolescentes y toxemias del embarazo. Salud Publica Mex. 2000; 42: 99-105. [ Links ]
9. Salvador J, Martínez Y, Lechuga A, Terrones A. Hipertensión inducida por el embarazo en adolescentes: un estudio multicéntrico. Ansiedad y Estres. 2005; 11: 17-25. [ Links ]
10. Cerón M, Harlow S, Sánchez C, Nuñez, R. Risk factors for pre-eclampsia among working women in Mexico City. Paediatr Perinat Epidemiol. 2001; 15:40-6. [ Links ]
11. Herrera JA, Ersheng G, Shahabuddin AKM, Lixia D, Wei Y, Faisal M, et al. Evaluación periódica del riesgo biopsicosocial prenatal en la predicción de las complicaciones maternas y perinatales en Asia 2002-2003. Colomb Med. 2006; 37 (Supl 1): 6-14. [ Links ]
12 .Terrones A, Salvador J, Lechuga A, Martínez Y, Garvalena MJ, Nápoles C. Diferencias en ansiedad estado-rasgo entre adolescentes con hipertensión inducida por el embarazo y adolescentes embarazadas sanas. Ansiedad y Estres. 2003; 9: 7-16. [ Links ]
13. Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwing LM, et al. Towards complete and accurate reporting of studies of diagnostic accuracy: The STARD initiative. Clin Chem. 2003; 49: 1-6. [ Links ]
14. De Weerth C, Graat G, Buitelaar J K, Thijssen JH. Measurement of cortisol in small quantities of saliva. Clin Chem. 2003; 49: 658-60. [ Links ]
15. Covelli M. Prevalence of behavioral and physiological risk factors of hypertension in African American adolescents. Pediatr Nurs. 2007; 33:323-32. [ Links ]
16. De Weerth C, Gispen De Wied C, Jansen L, Buitelaar J. Cardiovascular and cortisol responses to a psychological stressor during pregnancy. Acta Obstet Gynecol Scand. 2007; 86: 1181-92. [ Links ]
17. Browner WS, Newman TB, Hulley SB .Tamaño de muestra necesario por grupo cuando se usa la prueba de z para comprobar las proporciones de las variables dicotómicas. En: Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB (eds.). Diseño de investigaciones clínicas. 3a ed. Barcelona: Williams & Wilkinns; 2008: 97-9 [ Links ]
18. Secretaría de Salud. Norma oficial mexicana NOM-030SSA2-1999, para la prevención, tratamiento y control de la hipertensión arterial. México, DF: Secretaría de Salud. [ Links ]
19. Ávila RH, Tejero BE. Evaluación del estado de nutrición. En: Casanueva E, Kaufer HM, Pérez LA, Arroyo P (eds.). Nutriología médica. México: Editorial Médica Panamericana; 2001: 593-669. [ Links ]
20. Last JM. A dictionary of epidemiology. 4th ed. Oxford: International Epidemiological Association; 2001, p 32. [ Links ]
21. Sikkema J, Robles de Medina P, Schaad R, Mulder E. Salivary cortisol levels and anxiety are not increased in woman destines to develop preeclampsia. J Psychosom Res. 2001; 50: 45-9. [ Links ]
