










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombia Médica
On-line version ISSN 1657-9534
Colomb. Med. vol.45 no.2 Cali Apr./June 2014
Original Article
Caffeine modifies blood glucose availability during prolonged low-intensity exercise in individuals with type-2 diabetes
Cafeína altera la disponibilidad de glucosa en sangre durante ejercicio prolongado de baja intensidad en diabéticos tipo 2
Luiz Augusto da Silva1, Leandro de Freitas2, Thiago Emannuel Medeiros2, Raul Osiecki3, Renan Garcia Michel4, André Luiz Snak5 Carlos Ricardo Maneck Malfatti5*
1 Midwest State University of Parana, Pharmaceutical Science Postgraduate Program, Guarapuava, PR, Brazil.
2 State University of Santa Catarina, Physical Education Postgraduate Program, Florianópolis, SC, Brazil.
3 Federal University of Paraná, Department of Physical Education, Curitiba, PR, Brazil.
4 Campo Real College, Department of Biomedicine, Guarapuava, PR, Brazil.
5 Midwest State University of Parana, Department of Physiotherapy, Guarapuava, PR, Brazil.
*Corresponding author: Carlos Ricardo Maneck Malfatti, Department of Physiotherapy, Rua Simeão Camargo Varela de Sá, 03, 84015-430; Guarapuava- PR, Brazil. Phone: +55 42 3621 1000; FAX: +55 42 3621-1090. e-mail: crmalfatti@gmail.com.
da Silva LA, Freitas L, Medeiros TE, Osiecki R, Garcia MR, Snak AL, Maneck MCR. Caffeine modifies blood glucose availability during prolonged low-intensity exercise in individuals with type-2 diabetes. Colomb Med. 45(2): 72-76.
© 2014 Universidad del Valle. This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Article history: Received: 9 December 2013. Revised: 22 April 2014 Accepted: 28 May 2014
Abstract
Objective: The study investigated the effect of supplementation with maltodextrin (CHO) alone or associated to caffeine during exercise in T2DM subjects.
Methods: Pilot study, using Eight subjects with T2DM, aged 55±10 years, received CHO (1g/kg) or caffeine (1.5 mg/kg) alone or associated before exercise protocol. The exercise was executed at 40% heart rate (HR) reserve for 40 min, with 10-min recovery. Blood pressure (BP) and perceived exertion scale (Borg) were checked every 2 min. Blood glucose (BG) was checked every 10 min. For statistical analysis, ANOVA test was used and the value was considered statistically significant at p <0.05.
Results: The results showed that BP and HR did not change significantly among all treatments. Caffeine promoted a significant reduction in BG of 75 mg/dL (65%, p <0.05) during 40 min of exercise protocol compared to all groups.
Conclusion: Supplementation with 1.5 mg/kg of caffeine reduces BG concentration during prolonged exercise in T2DM patients.
Keywords: Diabetes mellitus, caffeine, supplementary feeding, exercise.
Resumen
Objetivo: El objetivo del estudio fue investigar los efectos de la suplementación con maltodextrina (CHO) sólo o combinado con cafeína durante el ejercicio en sujetos con diabetes tipo 2.
Métodos: Estudio piloto que incluyó ocho sujetos con DM2, de 55±10 años, el CHO (1g/kg) o cafeína (1.5 mg/kg) sólo o combinado antes del protocolo de ejercicio. El ejercicio se realizó a 40% de la frecuencia cardiaca (FC). Reserva del corazón durante 40 min con 10 min de recuperación. La presión arterial (PA) y la escala de esfuerzo (Borg) fueron revisados cada 2 min. La glucosa en sangre (GS) se comprobó cada 10 minutos. El análisis estadístico se realizó mediante ANOVA y consideró significación estadística un valor de p <0.05.
Resultados: Los resultados muestran que PA, FC y Borg no difirió significativamente entre los tratamientos. La cafeína promueve una reducción significativa en los niveles de glucosa en la sangre de 75 mg/dL (65%, p <0.05) durante un protocolo de ejercicio de 40 min en comparación con todos los grupos.
Conclusiones: Suplementación con 1.5 mg/kg de cafeína redujo significativamente los niveles de GS durante el protocolo de ejercicio en pacientes con DM2.
Palabras clave: Diabetes mellitus, cafeína, suplementación alimenticia, ejercicio.
Introduction
Diet and glycemic control during exercise is very important, preventing or delaying complications during and after exercise, like hyperglycemia or hypoglycemia, frequently detected in non-monitored diabetic patients. In addition, blood glucose (BG) control has a positive impact on long-term clinical outcomes in individuals with diabetes by delaying the onset and slowing the progression of serious diabetes-associated complications1.
The postprandial BG response is related to overall glucose control2 and it is significantly affected by the amount and type of carbohydrate (CHO) and the rate of carbohydrate digestion3. Slower rates of CHO digestion and absorption after a low-glycemic index meal result in a smaller rise in postprandial BG and a smaller rise in insulin4. Furthermore, diet modifications designed for people with diabetes may provide other benefits besides BG control in rest and during exercise5. The observed improvements in exercise performance with CHO ingestion have been attributed to maintenance of plasma glucose and glycogen availability6. Elevation of BG associated with supplementation is suggested to improve aerobic performance through reduction of muscle glycogen use or through the use of BG as a predominant fuel source as glycogen becomes depleted7. A recent study characterized the better dose for CHO supplementation, improved glycogen availability in muscle and liver. The CHO supplementation before exercise increased muscle and hepatic glycogen storage after prolonged exercise only by 1.0 g/kg in liver and 2.0 g/kg in muscle without insulin and lipid oxidation alterations8.
In diabetic patients, diet control and BG availability pre-exercise is very important, avoiding risk situations during exercise. Prior studies revealed that diet manipulation pre-exercise, like caffeine supplementation, can be employed as an ergogenic agent for a wide range of exercise conditions9 and it is often proposed that this effect is mediated by enhancing fat oxidation and decreasing CHO use in active muscles, but without mechanisms to support this theory. In fact, caffeine can directly antagonize adenosine receptors in many tissues, including tissues in the central nervous and cardiovascular systems and skeletal muscle and adipose tissue. This could result in a multitude of responses including adrenaline and noradrenalin secretion, altered blood flow, increased sympathetic nerve activity and blood pressure (BP), and increased BG and triglyceride mobilization10.
Awareness of the impact of caffeine on glucose availability in type 2 diabetes mellitus (T2DM) patients is rare and very limited. Thus, this study was performed to verify BG availability and cardiovascular alterations during aerobic exercise in diabetic patients pre-exercise CHO associated with caffeine feeding.
Materials and Methods
Subjects
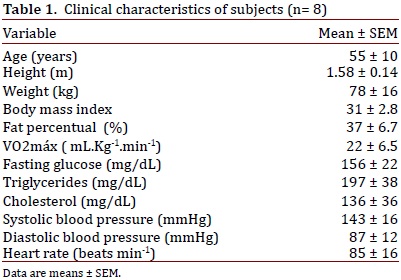
The pilot study consisted by group of eight T2DM patients; aged 55±10 years (see clinical conditions on Table 1). The subjects received maltodextrin (1.0 g/kg), caffeine (1.5 mg/kg), caffeine associated with maltodextrin (caffeine and maltodextrin drink), or placebo prior to testing. Informed consent was obtained for the study in accordance to Resolution of the National Council of Health, which was approved by the Ethics Committee of the Midwest State University of Parana (p.79538/2012).
Inclusion and exclusion criteria
The study only included patients with medical diagnosis of T2DM in accordance with the Report by the Expert Committee on the Diagnosis and Classification of Diabetes mellitus11; these subjects were free of other complications (cardiovascular disease, nephropathy, neuropathy, or retinopathy), as confirmed by their physicians. All subjects, but one, were considered non-caffeine users as defined by the consumption of <2 caffeinated coffee or tea beverages and/or <5 caffeine-containing soft drinks per week. Twelve hours prior to oral supplementation and exercise execution, hypertensive and diabetic medications were suppressed.
Protocol of physical exercise
Indirect VO2max was determined by using the Mile test protocol by Kline et al.,12. The exercise protocol was performed by using a treadmill ergometer. Patients were asked to exercise at 40% heart rate (HR), reserve for 40 min, followed by a 10-min passive recovery rate (HRmax) for age (using tables from the American Heart Association). The exercise rate was adjusted for individuals to find intensity in 40% of HR reserve.
Oral supplementation
The subjects received maltodextrin [1.0 g/kg; Design Nutrition Advanced (DNA)] or caffeine (1.5 mg/kg; SIGMA reagents), or Maltodextrin associated with caffeine in the same prior doses or placebo (3.5 g of CHO; light tangerine juice) dissolved in distilled water 30 min before exercise. Patients were fasted 8 h before supplementations. In addition, they were instructed to follow a diet with no caffeine-containing products and alcohol, and avoid strenuous physical activity two days before the experiments.
Laboratory analysis
Prior to the prescription of exercise and treatments (one week before), the patients were evaluated in the laboratory to obtain the biochemical, physiological, anthropometric, and physical information. Body mass and height were measured by using anthropometric devices (Welmy Corp., USA). Body fat was measured by means of the skinfolds technique13,14 using a skinfold caliper (Cescorf Corp., USA).
Cardiovascular parameters of BP (mercury column) and HR (Polar-T-61) were measured at rest, during different moments and after exercise session (checked every 2 min). The subjective perceived exertion and pain was rated by the Borg and Pain scale, respectively, used during exercise sessions15,16.
Venous blood samples (5 mL) were drawn randomly for biochemistry laboratory at 9.00 a.m., and were centrifuged at 1,500 rpm during 8 min for plasma separation. Plasma triglycerides, cholesterol, and glucose were dosed by glycerol phosphate oxidase/peroxidase and oxidase/peroxidase assay, respectively. In all methods, a BioSystems register kit was used.
Capillary blood samples (25 µL) were used to determine glucose concentrations during exercise during different moments (checked every 10 min) using a digital glucosimeter (ACCU - CHEK Performa, Roche®).
Statistical analyses
All data are expressed as means ± SEM. Statistical analysis was carried out by one-way analysis of variance (ANOVA) and F-values are presented only if p <0.05. Post hoc analysis was carried out, whenever appropriate, by the Tukey test.
Results
Within the exercise protocol, the patients were subjected to HR of predominant intensity at 40% of HR reserve. This intensity is in accordance with recent ADA recommendations17 for diabetic patients. Table 2 shows a similar cardiac work in different phases during 40 min of aerobic exercise, followed by 10 min of recovery period, which did not show any significant difference among treatments. Hence, systolic and diastolic BP were not different during the same protocol. The present results can characterize a non-positive cardiovascular stimulus by caffeine or CHO use.
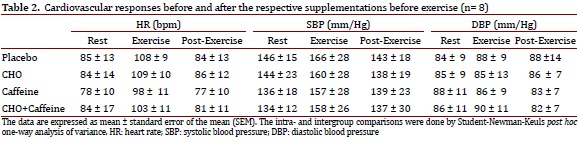
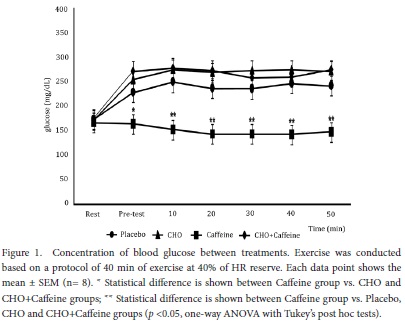
Figure 1 shows BG results. Blood glucose was not different at rest before all supplementations. Although, after 30 min of supplementations, before exercise, caffeine-induced BG reductions compared to CHO + Caffeine (87%), CHO alone (83%), or placebo (65%) groups. In addition, BG was different during 40 min of exercise protocol, with caffeine-induced BG reductions compared to CHO + Caffeine (83%) and CHO alone (87%) [F(3,28): 5.3; p <0.001], but there was no significant difference between caffeine alone compared to placebo. Hence, BG was different during 10 min after the exercise protocol, with caffeine-induced BG reductions compared to CHO + Caffeine (85%), CHO alone (84%), or placebo (63%) [F(3,28): 5.3; p <0.001].
Discussion
Past and recent studies with caffeine-induced modifications in glucose homeostasis have been contradictory. However, most studies concerning acute caffeine response to glucose homeostasis revealed increased insulin resistance due to immediate secretion of epinephrine18. In contrast, most long-term epidemiological studies revealed that long-term caffeine consumption via caffeinated drinks, such as coffee, had a rather beneficial action in glucose homeostasis to reduce the risk of T2DM19. A recent study showed that in diabetic rats with insulin resistance and secretion deficit, long-term consumption of caffeine improved both sensitivity and glucose-stimulated insulin secretion, regardless of caffeine associated CHO addition; whereas, sucrose itself aggravated insulin resistance. Improved insulin sensitivity resulting from long-term caffeine consumption, in both normal and diabetic rats, was related to reduced body weight and fat20.
It has been reported that concentrations of caffeine could directly stimulate the β cell secretion of insulin20,21. Caffeine alters the expression of glucose transporter 2 (GLUT2) and glucokinase in β cells, involved in the phosphorylation of the glucose mechanism and, consequently, with the release of insulin22. In the muscle, caffeine may improve the expression of GLUT4, by increasing concentrations of Ca2+ intracellular and also improved expression of AMPK enzyme22. Caffeine could also be acting on adenosine receptors on the cell membrane of the hepatocyte, which are involved in glycogenolysis and gluconeogenesis23.
Although this study was not designed to assess the mechanisms by which caffeine leads to glucose homeostasis, other studies showed increased serum insulin with the ingestion of caffeine21-23. The results obtained by these studies, through measurement of C-peptide concentrations, support the hypothesis that caffeine increases insulin concentrations via increased pancreatic secretion of the hormone rather than an alteration in insulin clearance24,25, along with decreased BG concentrations by the association of caffeine with effect of better glucose uptake obtained with exercise20,25.
Acute supplementation of caffeine and its effects can be seen from two different points: contribution to a suggestive increase of insulin release and BG control. However, it may have an adverse effect, it may have peaks of glucose uptake and cause hypoglycemia20-22,24; whereas, the effects of administering caffeine on glucose homeostasis are not clear. In the present study, administering 1.5 mg/kg caffeine during 40 min of exercise contributed to maintenance of BG levels at ~140 mg/dL. It has been proposed that during exercise these diabetic patients need adequate BG maintenance at approximately 100 mg/dL17,26.
Van Nieuwenhoven et al.27, showed that consumption of 1.4 mg/kg of caffeine and 45 g of glucose administered for 90 min of exercise at 70% of maximal power output (Wmax) resulted in a significant increase of 23% in intestinal absorption of glucose consumption compared with glucose alone. According to the authors, caffeine could influence the activity of glucose transporters in the digestive system increasing BG. In the present study, intake of caffeine associated with CHO bears no difference in BG compared to intake of CHO alone, maybe due to the effect of caffeine on intestinal absorption of glucose, keeping BG to the Caffeine + CHO group the same as supplementation with CHO alone. Yeo et al.28, demonstrated in their study that no difference in BG concentration was noted during exercise with carbohydrate intake associated to caffeine compared to treatment with carbohydrates.
In relation to chronic use, Conde et al.29, concluded that long-term caffeine intake (1 g/L) prevented development of insulin resistance by elevated blood insulin and lower blood glucose in diabetic rats.
A study by Noordzij et al.30, revealed that the influence of caffeine on cardiovascular stimulation is directly related to the amount of caffeine consumed. The effect of caffeine on cardiovascular responses is due to the classic effect of caffeine on increased release of catecholamines, which directly influence the sympathetic nervous system and the consequent increase in blood pressure31. In this study, no significant difference was observed among the groups possibly related to the dosage of 1.4 mg/kg of caffeine.
Thereby, the results showed in this study pilot, that acute caffeine ingestion in low doses prior to exercise could amplify peripheral glucose uptake and consumption during aerobic exercise.
Acknowledgment
This work was supported by the Brazilian agencies: CNPq, National Council for Science and Technology and FA, Araucária Foundation from Paraná State.
Conflict of Interest
All authors do not have any possible conflicts of interest.
References
1. World Health Organization . Diabetes. Descriptive data 312. 2009. [ Links ]
2. Monnier L, Lapinski H, Colette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of patients with T2DM: variations with increasing levels of HbA(1c) Diabetes Care. 2003; 3: 881-5. [ Links ]
3. O'Dea K, Snow P, Nestel P. Rate of starch hydrolysis in vitro as a predictor of metabolic responses to complex carbohydrate in vivo. Am J Clin Nutr. 1981; 34: 1991-3. [ Links ]
4. Wolever TM, Yang M, Zeng XY, Atkinson F, Brand-Miller JC. Food glycemic index, as given in glycemic index tables, is a significant determinant of glycemic responses elicited by composite breakfast meals. Am J Clin Nutr. 2006;83:1306-1312. [ Links ]
5. Voss AC, Maki KC, Garvey T, Hustead DS, Alish C, Fix B, et al. Effect of two carbohydrate-modified tube-feeding formulas on metabolic responses in patients with type 2 diabetes. Nutrition. 2008; 24: 990-7. [ Links ]
6. Coggan AR, Coyle EF. Reversal of fatigue during prolonged exercise by carbohydrate infusion or ingestion. J Appl Physiol. 1987; 63: 2388-95. [ Links ]
7. Coyle EF, Coggan AR, Hemmert MK, Ivy JL. Muscle glycogen utilization during prolonged strenuous exercise when fed carbohydrate. J Appl Physiol. 1986; 61: 165-72. [ Links ]
8. Ruffo AM, Osiecki R, Fernandes LC, Felipe CS, Osiecki AC, Malfatti CRM. Moderate to high dose of maltodextrin before exercise improves glycogen availability in soleus and liver after prolonged swimming in rats. JEPonline. 2009; 12: 30-8. [ Links ]
9. Graham TE. The possible actions of methylxanthines on various tissues. Clin Pharmacol Sport Exerc. 1997:257-267. [ Links ]
10. Paluska SA. Caffeine and exercise. Curr Sports Med Rep. 2003; 2: 213-9. [ Links ]
11. American Diabetes Association Diagnosis and classification of diabetes mellitus. Diabetes Care. 2010; 33(1): s62-9. [ Links ]
12. Kline GM, Porcari JP, Hintermeister R. Estimation of VO2max from a one-mile track walk, gender, age, and body weight. Med Sci Sports Exerc. 1987; 19: 253-9. [ Links ]
13. Jackson AS, Pollock ML, Graves JE, Mahar MT. Reliability and validity of bioelectrical impedance in determining body composition. J Appl Physiol. 1998; 64: 529-34. [ Links ]
14. Siri WE. Body composition from fluid spaces and density. Washington DC: National Academy of Science; 1961. [ Links ]
15. Borg G, Noble BJ. Psycophysical bases of perceived exertion. Med Sci Sport Exerc. 1982;14:377-381. [ Links ]
16. Huskisson EC. Measurement of pain. Lancet. 1974;2:1127-31. [ Links ]
17. American Diabetes Association. Physical Activity/Exercise and Diabetes Mellitus. Diabetes Care. 2006; 29: 1433-8. [ Links ]
18. Keijzers GB, De Galan BE, Tack CJ, Smits P. Caffeine can decrease insulin sensitivity in humans. Diabetes Care. 2002; 25: 364-9. [ Links ]
19. Salazar-Martinez E, Willett WC, Ascherio A, Manson JE, Leitzmann MF, Stampfer MJ, et al. Coffee consumption and risk for type 2 diabetes mellitus. Ann Intern Med. 2004; 140: 1-8. [ Links ]
20. Park S, Jang JS, Hong SM. Long-term consumption of caffeine improves glucose homeostasis by enhancing insulinotropic action through islet insulin/insulin-like growth factor 1 signaling in diabetic rats. Metab Clin Exp. 2007; 56: 599-607. [ Links ]
21. Bruton JD, Lemmens R, Shi CL, Persson-Sjögren S, Westerblad H, Ahmed M. Ryanodine receptors of pancreatic beta-cells mediate a distinct context-dependent signal for insulin secretion. FASEB J. 2003; 17: 301-3. [ Links ]
22. Park S, Scheffler TL, Gunawan AM, Shi H, Zeng C, Hannon KM, et al. Chronic elevated calcium blocks AMPK-induced GLUT-4 expression in skeletal muscle. Am J Physiol Cell Physiol. 2009; 296(1): c106-15. [ Links ]
23. Yasuda N, Inoue T, Horizoe T, Nagata K, Minami H, Kawata T, et al. Functional characterization of the adenosine receptor contributing to glycogenolysis and gluconeogenesis in rat hepatocytes. Eur J Pharmacol. 2003; 459: 159-66. [ Links ]
24. Greenberg JA, Owen DR, Geliebter A. Decaffeinated coffee and glucose metabolism in young men. Diabetes Care. 2010; 33: 278-80. [ Links ]
25. Chu Y-F, Chen Y, Black RM, Brown PH, Lyle BJ, Liu RH, et al. Type 2 diabetes-related bioactivities of coffee: Assessment of antioxidant activity, NF-kB inhibition, and stimulation of glucose uptake. Food Chemistry. 2011; 124(3): 914-20. [ Links ]
26. American College of Sports Medicine Exercise and Type 2 diabetes. Med Sci Sport Exerc. 2010; 42: 2282-303. [ Links ]
27. Van Nieuwenhoven MA, Brummer RM, Brouns F. Gastrointestinal function during exercise: comparison of water, sports drink, and sports drink with caffeine. J Appl Physiol. 2000; 89: 1079-85. [ Links ]
28. Yeo SE, Jentjens RLPG, Wallis GA, Jeukendrup AE. Caffeine increases exogenous carbohydrate oxidation during exercise. J Appl Physiol. 2005; 99: 844-50. [ Links ]
29. Conde SV, Nunes da Silva T, Gonzalez C, Mota Carmo M, Monteiro EC, Guarino MP. Chronic caffeine intake decreases circulating catecholamines and prevents diet-induced insulin resistance and hypertension in rats. Br J Nut. 2012; 107(1): 86-95. [ Links ]
30. Noordzij M, Uiterwaal CS, Arends LR, Kok FJ, Grobbee DE, Geleijns JM. Blood pressure response to chronic intake of coffee and caffeine: a meta-analysis of randomized controlled trials. J Hypertens. 2005; 23(5): 921-8. [ Links ]
31. Nurminen ML, Niittynen L, Korpela R, Vapaatalo H. Coffee, caffeine and blood pressure: a critical review. Eur J Clin Nutr. 1999; 53(11): 831-9. [ Links ]
