Letter to editor
Clinical differences between children with asthma and rhinitis in rural and urban areas
1Universidad del Valle, School of Public Health, Faculty of Health, CISALVA Institute, Cali, Colombia.
Dear Editors:
In their article, Sánchez, et al
1 have reported about an interesting study on asthma and rhinitis symptoms among children in urban and rural Colombian areas, describing that the control of symptoms, over time, is more difficult among children in urban areas. Their article has the methodological advantage of having done a prospective follow-up of pediatric patients with asthma and rhinitis; nevertheless I have some questions:
1) The sample size calculation is not clear. The authors mentioned the prevalence of asthma and rhinitis in the urban areas and their corresponding error, but they did not use these parameters in the sample size calculation. On the other hand, the authors argued that the main outcome was comparing the treatment of asthma and rhinitis between urban and rural areas; thus readers could assume that the measure of effect was the difference of the Asthma Control Test (ACT) score between both areas; but the authors did not clearly explain it. Furthermore, it is not clear why the ratio of urban/rural subjects is 1.57; is the ratio observed in the study health centers? In this line, it seems that the appropriate sample size calculation must have been the difference of means between two independent populations, although the authors did not report any ACT effect size based on previous studies. Thus, I have estimated the means difference (as the effect size) given the power (80%) and the study sample size (urban= 201 and rural= 128) provided by the authors; using Stata® 14.2 (power twomeans command). In this manner, the detectable effect size would be 3.5; which is higher than the ACT effect size estimated in the Sánchez, Sánchez and Cardona’s article (i.e.: 3.0), leading to an underpowered study, at least for the cross-sectional estimates. In this manner, what was the appropriate sample size calculation?
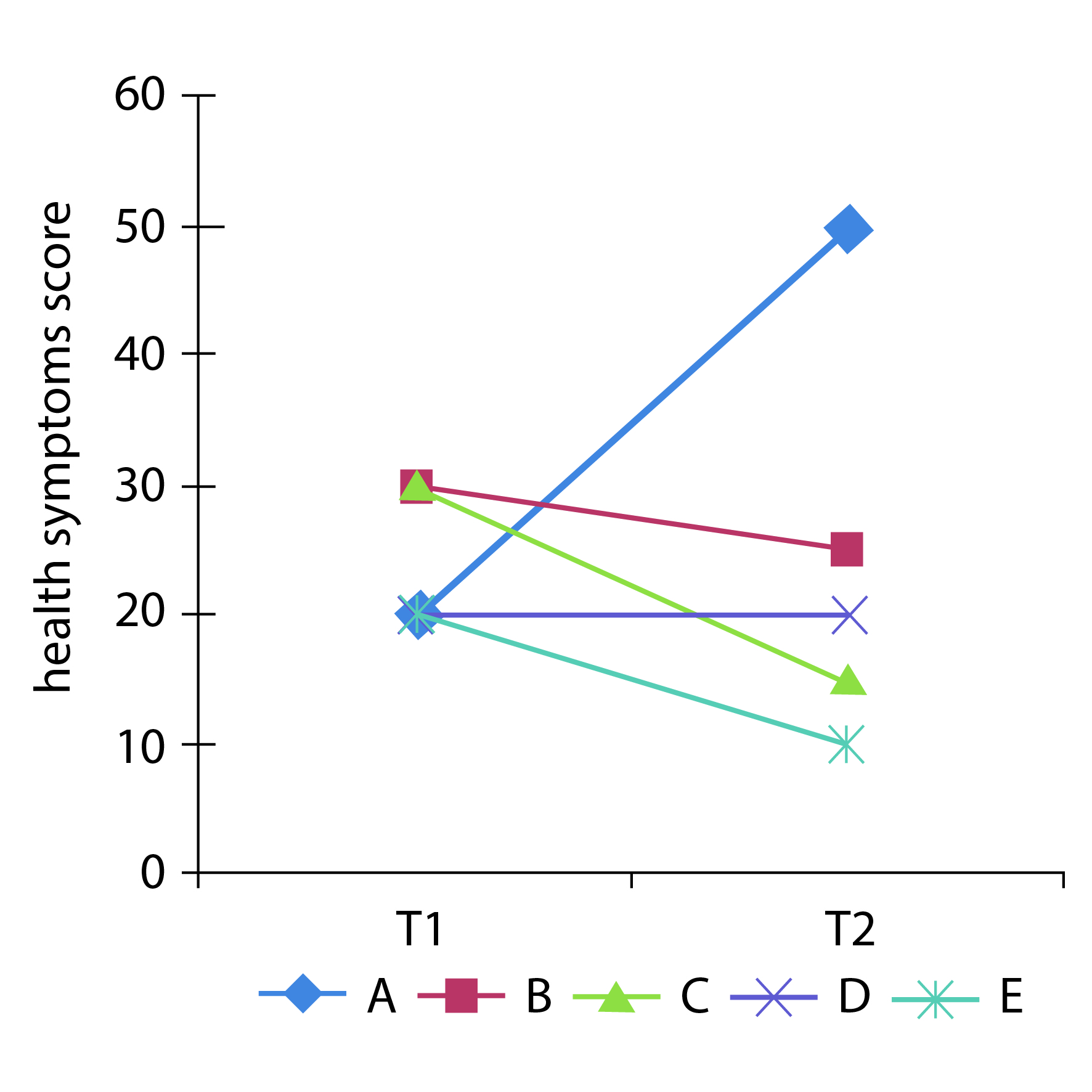
2) The research was designed as a follow-up study with four assessments, at 3, 6, 9 and 12 months, but the statistical analyses were done using a cross-sectional approach at each measurement without taking into account the multilevel nature of the repeated (or longitudinal) measures of each patient and without the baseline adjustments of the outcome scores. The cross-sectional analyses are not appropriate for determining within-subject’s longitudinal patterns; for example, Figure 1 shows the hypothetical follow-up of a health symptoms score of five subjects, with two assessments over time (T=1 and T=2). The estimated cross-sectional mean at each time is the same (24 points), but individual persons’ trajectories (i.e. the lines) show different patterns: some subjects improve and others worsen over time. In this manner, it is important to emphasize that in the Sánchez, Sánchez and Cardona’s article, the monthly measures of each single patient are nested (or clustered) into each individual, which constitutes a longitudinal multilevel structure2. Nowadays, there are several parametric and non- parametric statistical approaches for dealing appropriately with this kind of longitudinal data analysis: i.e. follow-up of patients with repeated measures of the outcome variables over time 3,4. The current longitudinal data analyses techniques have the advantage of allowing for the analyses of incomplete and unbalanced longitudinal data: i.e. data with missing measurements (under the MCAR or MAR missing data assumptions), attrition and/or different assessment moments5,6. Furthermore, nowadays these longitudinal data analysis, with mixed regression models or Bayesian approaches, have been implemented in several statistical software packages (4). These techniques allow dealing not only with normal continuous outcomes, but also with non-normal continuous, dichotomous and polytomous categorical outcome variables 6. Furthermore, in Sánchez, et al. (1, Figure 3, the 12-months pharmacotherapy comparisons between urban and rural children did not adjust for the baseline values of the corresponding pharmacotherapy scores, which were different between urban and rural children. Thus, the estimated differences at the 12-months follow-up could be explained, instead, by those baseline scores. Finally, due to the research design is an epidemiological observational study, it is necessary to perform analyses adjusting for the confounding variables which are conceptually related with the outcome variables 7,8, because children’s urban or rural residences were not randomly allocated. In this manner, what are the effects of the urban environment on the pharmacotherapy scores and the symptoms of asthma and rhinitis over time, after performing the appropriate statistical analyses (i.e. multipleand repeated measures 3,4 regression models)?
3) When the design of a research is a longitudinal study with repeated measures, and its data are appropriately analyzed with up-to-date statistical methods, this situation allows dealing with smaller sample size given the efficiency of the longitudinal data analysis methods, which improves when adding more measurements per subject 4. Sample size calculation guidelines, for studies with repeated measures, have been addressed by Guo, Logan, Glueck and Muller 9. Did you take into account these sample size calculations in your study?
4) Neither the location nor the health care level of the study centers are clear; nor are the criteria to select them. For example, if children of rural areas with the worst symptoms levels are referred to higher complexity health centers different to those in the study, it could be a selection bias which could affect the study findings 7,10. Thus, which are the health care levels and locations of the study centers and which are the related potential biases?
References
1. Sánchez J, Sánchez A, Cardona R. Clinical differences between children with asthma and rhinitis in rural and urban areas. Colomb Med (Cali). 2018; 49(2): 169-174.
[ Links ]
2. Snijders TAB, Bosker RJ. Multilevel analysis: an introduction to basic and advanced multilevel modeling. 2nd ed. Los Angeles: SAGE; 2012.
[ Links ]
3. Fitzmaurice G, Davidian M, Verbeke G, Molenberghs G. Longitudinal data analysis. Boca Raton: CRC Press Taylor & Francis Group; 2009.
[ Links ]
4. Brown H, Prescott R. Applied mixed models in medicine. 3rd ed. West Sussex: Wiley; 2015.
[ Links ]
5. Cnaan A, Laird NM, Slasor P. Using the general linear mixed model to analyse unbalanced repeated measures and longitudinal data. Statist Med. 1997; 16(20): 2349-2380.
[ Links ]
6. Gueorguieva R, Krystal JH. Move over ANOVA: progress in analyzing repeated- measures data and its reflection in papers published in the Archives of General Psychiatry. Arch Gen Psychiatry. 2004; 61(3): 310-317.
[ Links ]
7. Szklo M, Nieto J. Epidemiology beyond the basics. 2nd ed. Sudbury, MA: Jones and Bartlett; 2007.
[ Links ]
8. Hernán MA, Hernández-Díaz S, Werler MM, Mitchell AA. Causal knowledge as a prerequisite for confounding evaluation: an application to birth defects epidemiology. Am J Epidemiol. 2002; 155(2): 176-184.
[ Links ]
9. Guo Y, Logan HL, Glueck DH, Muller KE. Selecting a sample size for studies with repeated measures. BMC Med Res Methodol. 2013; 13(1): 100.
[ Links ]
10. Hernán MA, Hernández-Díaz S, Robins JM. A structural approach to selection bias. Epidemiology. 2004;15:615-625.
[ Links ]
Dear Editors:
We greatly appreciate the interest shown in the article "Clinical differences between children with asthma and rhinitis in rural and urban areas", which we hope will be one of several future articles that we intend to carry out in the study cohort. To the questions generated by the reader, one is focused on the calculation of the sample size, while the other two questions are focus in the method of analysis, and the reader suggests, it could be more robust.
Regarding the sample size, we describe that infant asthma in urban areas of Medellin was 11% and rhinitis 23%, according to previous studies. There is no data available for the rural area. We note that with a confidence level of 95%, a power of 80% and a sample size error of 0.5%, the sample size was calculated; estimating 201 children for the urban area and 128 for the rural area. Finally, we recruited and were able to continue for a year, a total of 248 children from the urban area and 134 from the rural area. The complaint of the reader, is focus that the more appropriated technique would be "… the appropriate sample size calculation must have been the difference of means between two independent populations, although the authors did not report any ACT effect size based on previous studies." First, we fully agree with the reader that for this type of design, the study lost power by the form of sample size calculation. We did not find studies with the urban and rural ACT tests in the studied population, which made it impossible to obtain these parameters to perform the sample size calculation by the technique "power two means" (difference of means of two independent groups). ). As we noted in the article, we do not have previous data in the rural population that allow us to infer the precise prevalence of asthma in this area; as we also noted in the article the prevalence in Colombia of asthma in the general urban population is 11%, there are also data that indicate that in the child population (less than 12 years) it is around 23%; if we work with these two prevalence where we assume that the highest in children is for the urban population and that possibly the lowest corresponds to what happens in the rural population 1 and assuming the parameters; alpha 0.05, power 0.80, delta 0.12 rural prevalence 0.11 vs. urban prevalence 0.23, a sample size of 306 is required; 153 for each group; in the urban area we had the availability of 201 children and in the rural area we made 128, which is close to the desired. Therefore we consider that we fulfill the expectation according to the mathematical formula used (chi-squared test comparing two independent proportions).
Regarding the following two questions of the reader that are focus in the design of the study and the analysis of the data; it is important to clarify that although a follow-up was carried out over time, for this study we wanted to focus in compared two groups (rural and urban) specially after 12 months of clinical treatment. We agree with the reader that a longitudinal analysis of repetitive measures would be appropriate and would provide additional interesting information for the effect of changes in the tests over time (e.g. ACT), however, for this study, we wanted to focus the results and the discussion, in compare these measures in two moments clinically relevant for the doctor; In the first consultation, the doctor sends a treatment and in the follow-up can make adjustments according to the clinical response; usually after one year if patient have a good clinical control, begins the process of dismantling the therapies. That’s why we preferred to highlight the final moment versus the initial moment. We recognized that the information in the intermediate times (3 months and 6 months) could be analyze in a longitudinal way, and in this form, we could evaluate the effect, but it contributes less for the objective that we planted, that was to compare if there were differences in the groups studied, especially at the end of the study, presumably due to the medical interventions carried out.
Again, we thank the reader for their pertinent suggestions that put in their real dimension the results of our research and that will serve us for the next analyzes that we will carry out with this population.
Estimados editores:
Apreciamos enormemente el interés mostrado por el artículo "Diferencias clínicas entre niños con asma y rinitis en áreas rurales y urbanas", el cual esperamos sea uno de los futuros artículos que pretendemos llevar a cabo en la cohorte del estudio. A las preguntas generadas por el lector, una se enfoca en el cálculo del tamaño de la muestra, mientras que las otras dos preguntas se enfocan en el método de análisis. El lector sugiere que podría ser más sólido.
Con respecto al tamaño de la muestra, describimos que el asma infantil en las áreas urbanas de Medellín fue del 11% y la rinitis del 23%, según estudios anteriores. No hay datos disponibles para el área rural. Notamos que con un nivel de confianza del 95%, una potencia del 80% y un error de tamaño de muestra del 0.5%, se calculó el tamaño de la muestra; estimando 201 niños para el área urbana y 128 para el área rural. Finalmente, reclutamos y pudimos seguir por un año, un total de 248 niños del área urbana y 134 del área rural. La solicitud del lector, se centró en que la técnica más apropiada sería "... el cálculo del tamaño de muestra apropiado debe haber sido la diferencia de medias entre dos poblaciones independientes, aunque los autores no informaron ningún tamaño de efecto de ACT basado en estudios anteriores". Primero, estamos totalmente de acuerdo con el lector en que para este tipo de diseño, el estudio perdió potencia por la forma de cálculo del tamaño de la muestra. No se encontraron estudios con las pruebas ACT urbanas y rurales en la población estudiada, lo que hizo imposible obtener estos parámetros para realizar el cálculo del tamaño de la muestra mediante la técnica "potencia de dos medias" (diferencia de medias de dos grupos independientes). Como señalamos en el artículo, no tenemos datos previos en la población rural que nos permitan inferir la prevalencia precisa del asma en esta área; Como también señalamos en el artículo, la prevalencia de asma en Colombia en la población urbana en general es del 11%, también hay datos que indican que en la población infantil (menos de 12 años) es de alrededor del 23%; si trabajamos con estas dos prevalencias donde asumimos que la más alta se encuentra en niños de la población urbana y que posiblemente la más baja corresponda a lo que sucede en la población rural 1 y asumiendo los parámetros; alfa 0.05, potencia 0.80, delta 0.12 prevalencia rural 0.11 vs. prevalencia urbana 0.23, se requiere un tamaño de muestra de 306; 153 para cada grupo; en el área urbana tuvimos la disponibilidad de 201 niños y en el área rural reclutamos 128 niños, que está cerca del numero deseado. Por lo tanto, consideramos que cumplimos con las expectativas de acuerdo con la fórmula estadisitica utilizada (prueba de chi cuadrado que compara dos proporciones independientes).
Con respecto a las siguientes dos preguntas del lector que se centran en el diseño del estudio y el análisis de los datos; es importante aclarar que aunque se realizó un seguimiento a lo largo del tiempo, para este estudio quisimos centrarnos en comparar los dos grupos (rurales y urbanos), especialmente después de 12 meses del tratamiento clínico. Estamos de acuerdo con el lector en que un análisis longitudinal de medidas repetitivas sería apropiado y proporcionaría información adicional interesante para el efecto de los cambios en las pruebas a lo largo del tiempo (p. ej., ACT); sin embargo, para este estudio, quisimos enfocar los resultados y la discusión en comparar estas medidas en dos momentos clínicamente relevantes para el médico; en la primera consulta, el médico envía un tratamiento y en el seguimiento puede realizar ajustes de acuerdo con la respuesta clínica. Generalmente después de un año, si el paciente tiene un buen control clínico, comienza el proceso de desmantelamiento de las terapias. Es por eso que preferimos resaltar el momento final frente al momento inicial. Reconocimos que el análisis de la información en los tiempos intermedios (3 meses y 6 meses) fue de forma longitudinal y, que de esta forma, podíamos evaluar el efecto, pero contribuye menos al objetivo que planteamos, que fue comparar si hubo diferencias en los grupos estudiados, especialmente al final del estudio, probablemente debido a las intervenciones médicas realizadas.
Nuevamente, agradecemos al lector sus sugerencias pertinentes que ponen en su dimensión real los resultados de nuestra investigación y que nos servirán para los próximos análisis que realizaremos con esta población












 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink