











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Remark
| 1)Why was this study conducted? |
| To provide evidence about the use of whole body computed tomography in cases of severe trauma. There has been controversy about its use in hemodynamically unstable patients and in patients with severe trauma, furthermore, there are still many surgeons around the world reluctant to use this imaging tool in these escenarios |
| 2) What were the most relevant results of the study? |
| In a group of patients with severe trauma, more than half (65.4%) underwent non-operative management after receiving a whole-body CT. Total radiation doses were less than 20 mSv in most of the patients. Also, the calculated survival rates and the real survival rates did not vary between patients with penetrating or blunt trauma, with hemodynamical stability or instability. |
| 3) What do these results contribute? |
| Results provide evidence on the utility of Whole-Body Computed-Tomography on the management of severe trauma patients, who besides their severity, did not had any delay in their management and more than half could receive non-surgical management. Finally, the use of this imaging technique did not significantly increase radiation exposure or mortality when comparing with the calculated survival rates, proving that it was safe and efficient to use in our trauma patients. |
Introduction
Trauma is the second cause of death in men of all ages, accounting for 7% of all deaths in Colombia in 2018 1,2. During initial evaluation of trauma patients in the emergency department, prompt attention by the trauma team, early diagnosis and effective treatment have been the main survival determinants 3-5. Whole-body computed tomography is currently the standard method of workup recommended for the primary evaluation of trauma patients at many centers because of its high sensitivity and specificity for the diagnosis of injuries, in cases of abdominal trauma, it reaches a sensitivity of 94% and specificity of 95%, superior to ultrasound and clinical evaluation (S: 30-75%; E: 30-50%) 6. Moreover, there is a growing body of evidence on the benefits of this diagnostic method, increasing the probability of survival in polytrauma patients 7-10 without a significative increase in overall costs 1,2,11,12. In addition, compared with selective images, Whole-body computed tomography can identify less evident lesions that could go undetected, translating to improved prognosis, lower mortality and less waiting time in the emergency department 1,13-15. However, its use has been limited in hemodynamically unstable trauma patients because of the potential delay in therapeutic interventions 6 and exposure to unnecessary radiation 10,16-21. Many different whole-body computed tomography protocols have been used worldwide, but the optimal technique is still not clear 14,17,22-24. Achieving an optimal equilibrium phase is important to visualize arterial and venous phases in a single image acquisition, to identify the hemorrhage source and reduce the time in the computed tomography suite. The objective of this study was to describe the implementation of a new institutional single-pass whole-body computed tomography protocol in the management of patients with severe blunt/penetrating trauma, hemodynamically stable or unstable, as a diagnostic tool for the decision making between surgical or non-surgical treatment.
Materials and Methods
With prior institutional ethics approval, a descriptive evaluation of patients who underwent single-pass whole-body computed tomography was performed. The institutional single-pass whole-body computed tomography protocol of Fundación Valle del Lili (a Level I Trauma Center in Cali, Colombia) was created in 2016 establishing the indication for whole-body computed tomography in all patients with severe polytrauma: moderate to severe head trauma, suspected solid organ injury, hollow viscus or vascular injury, pelvic trauma and unstable fractures that arrived hemodynamically stable or unstable. All adult patients (>15-years) who met these criteria and underwent whole-body computed tomography between January, 2017 and December, 2018 were included and followed-up by a research assistant. Patients who were transferred from or to another institution were excluded, this way only patients with complete information and follow-up were included. Data on demographics, trauma mechanism, clinical severity (Injury Severity Score (ISS), New Injury Severity Score (NISS), SOFA Scale) and outcomes (surgical or non-surgical management, ICU admission and mortality) were extracted from clinical records. Calculated survival rates were assessed using the Trauma and Injury Severity Score (TRISS), which uses clinical parameters to determine the probability of survival, in order to perform comparisons with the real survival rate and evaluate possible impact on mortality with our management algorithm.
Data was acquired using a multi-slice IVR- computed tomography system (Aquilion ONE 320 Slice computed tomography scanner, software version 7.0, Toshiba Medical Systems Corp., Tochigi, Japan). The scanner is located adjacent to the trauma bay (<100 feet). Each patient was accompanied by the trauma team (Trauma and Acute Care Surgeon, Fellow, Surgery Resident, Emergency Physician and Trauma Nurses). The radiologist read each study in real time. Resuscitation was initiated in the trauma bay and continued during scanning.
Whole-body computed tomography included a non-contrast brain and a contrasted neck, chest, abdomen and pelvis (from the base of the skull to lower edge of the pubis) as a single-pass computed tomography helical acquisition (Table 1). Low osmolar non-ionic contrast medium (Iopromide Ultravist R. Whippany, NJ: Bayer Health Care Pharmaceuticals) was administered via an 18-gauge peripheral intravenous (IV) catheter. A total of 130 mL of contrast, with biphasic injection technique, was used with an inter-bolus delay of 45 seconds. First phase was a 60 mL bolus of iopramide IV, at a rate of 2.0 mL/s in 30 seconds, followed by an iopromide administration pause of 45 seconds. Second phase consisted of a 70 mL bolus of iopramide IV, at a rate of 4.0 mL/s in 17 seconds. Finally, 40 mL of normal saline solution IV was administered, at a rate of 4.0 mL/s in 10 seconds, with a total time of infusion of 175 seconds. Contrasted acquisition was started immediately after the second bolus.
Table 1 New Single-Pass WBTC Protocol
| Phase | Procedure | |
|---|---|---|
| Phase A | Simple acquisition phase: skull | |
| Phase B | Contrast administration phase: neck, thorax and abdomen IV contrast: Iodinated, non-ionic hypo-osmolar (370 mg/mL) | |
| Step 1: First injection | Flow rate= 2.0 cc/s | |
| Vol. Contrast medium= 60 cc | ||
| Pause of 45 s | ||
| Total duration: 75 seconds | ||
| Step 2: Second injection | Flow rate= 4cc/s | |
| Vol. Contrast medium= 60-70 cc | ||
| Sweep= 40 cc Normal saline | ||
| Duration:25 seconds | ||
| Total time: 100 seconds | ||
| Step 3: Contrasted acquisition | In the Descending Aorta ROI= 200 UH, after the second injection. | |
Sequential contrast bolus resulted in a single acquisition reflecting the combination of arterial and portal venous phases, with excellent image quality and fast image reconstruct. The reconstruction slices were 1 mm every 0.8 mm, total number of slices depended on the height of the patient. Computed tomography intravenous pyelogram was omitted in the whole-body computed tomography protocol, but this was added as needed.
Parameters such as the incidence of contrast-induced nephropathy, total radiation dose measured in millisieverts (mSv) (considered optimal when <20 mSv), number of cases that the whole-body computed tomography changed clinical management and time measured in minutes to reach final diagnosis, were evaluated. Patients were considered hemodynamically unstable on arrival when systolic blood pressure was <100 mmHg.
To evaluate outcomes of different scenarios that a trauma surgeon or emergency physician could face, patients were divided in three groups according to their mechanism of trauma and hemodynamics upon arrival:
Group 1: blunt trauma and hemodynamically stable
Group 2: blunt trauma and hemodynamically unstable
Group 3: penetrating trauma hemodynamically stable or unstable
Ethics approval
Ethics approval was granted by the Institutional Review Board from Fundación Valle del Lili under the number 554 in 2014 and has been update annually since its approval
Statistical analysis
Descriptive analysis was performed to display demographics, clinical condition upon admission, anatomical/physiological severity and clinical outcomes. Median and interquartile range (IQR) were used to report continuous variables without normal distribution, and median and standard deviation (SD) were used to report continuous variables with normal distribution. Continuous variables were compared using non-parametric test (Kruskal-Wallis Test) or parametric test (ANOVA), depending on their normality. Categorical variables are presented in absolute frequencies and percentages; comparisons were made with Ji 2 test or Fisher’s exact test when the frequencies were lower than 5. Data management and statistical analysis were performed on STATA/MP Software version 14.0 (StataCorp, College Station, TX).
Results
A total of 263 patients underwent whole-body computed tomography (Group 1: 168, Group 2: 50 and Group 3: 45. Most patients were male [223 (85.4%)]. Patients in Group 2 had the highest injury severity upon admission with the lowest systolic blood pressure [systolic blood pressure= Group 1: 124 mmHg (IQR: 113-140), Group 2: 85 mmHg (IQR: 70-93), Group 3: 112 mmHg (IQR: 96-138)], lowest Glasgow Coma Scores [Group 1: 13 (IQR: 7-15), Group 2: 10 (IQR: 3-14), Group 3: 15 (IQR: 10-15)] and were more acidotic [Base excess=Group 1: -5.9 mEq/L (IQR: -8.0 a -4.0), Group 2: -8.9 mEq/L (IQR: -12.6 a -5.7), Group 3: -6 (IQR: -10.0 a -4.8)] (Table 2).
Table 2 Parameters at admission to Emergency Department
| Variable | Total (n=263) | Group 1 (n= 168) | Group 2 (n= 50) | Group 3 (n= 45) | p |
|---|---|---|---|---|---|
| Age (median (IQR))* | 31 (23-49) | 32 (23-51) | 39 (27-51) | 26 (20-34) | <0.001 |
| Male Gender (n (%)) | 223 (85.4) | 142 (85.0) | 39 (78.0) | 42 (95.4) | NS* |
| Emergency Department Parameters | |||||
| SBP*, mmHg median (IQR) | 117 (100-138) | 124 (113-140) | 85 (70-93) | 112 (96-138) | <0.001 |
| HR*, median (IQR) | 90 (73-107) | 86 (71-100) | 108 (86-120) | 95 (81-107) | NS* |
| GCS, median (IQR) | 13 (7-15) | 13 (7-15) | 10 (3-14) | 15 (10-15) | 0.006 |
| Base excess, mEq/L median (IQR) | -6.2 (-9.0;-4.3) | -5.9 (-8.0; -4.0) | -8.9 (-12.6; -5.7) | -6 (-10.0; -4.8) | 0.002 |
| Lactate, mmol/L, median (IQR) | 3.0 (1.9-4.9) | 2.8 (1.8-4.1) | 4.2 (2.6-6.4) | 2.8 (1.7-5.6) | <0.001 |
| Severity | |||||
| ISS*, median (IQR) | 22 (16-30) | 21 (14-29) | 25 (18-34) | 26 (19-35) | NS* |
| NISS*, median (IQR) | 27 (18-41) | 26 (17-34) | 28 (21-41) | 42 (27-54) | <0.001 |
| Intraoperatory hemorrhage median (IQR) | 350 (100-1200) | 275 (100-800) | 750 (300-2000) | 550 (250-1450) | 0.007 |
| Resuscitation | |||||
| Crystalloids, median (IQR) | 2430 (1400-3690) | 2258 (1232-3260) | 3325 (2430-4800) | 2400 (1520-4010) | 0.02 |
| RBCU*, median (IQR) | 4 (2-5) | 2 (2-4) | 4 (2-5) | 4 (2-4) | 0.04 |
| Plasma, median (IQR) | 4 (2-6) | 4 (2-4) | 4 (2-6) | 4 (3-6) | 0.02 |
Group 1: blunt trauma and hemodynamically stable
Group 2: blunt trauma and hemodynamically unstable
Group 3: penetrating trauma hemodynamically stable or unstable
IQR: interquartile range
SBP: systolic blood pressure
HR: heart rate
GCS: Glasgow coma scale
ISS: injury severity score
NISS: new injury severity score
RBCU: red blood cells units
NS: non significant
Median injury severity score was 22 (IQR: 16-22), in Group 1 was 21 (IQR: 14-29), in Group 2 was 25 (IQR: 18-34) and in Group 3 was 26 (IQR: 19-35). Patients with blunt trauma and hemodynamically unstable required more resuscitation with higher rates of crystalloids, packed red blood cells and plasma transfusions during the first 24 hours upon arrival to the trauma center (Table 2). A total of 172 patients (65.4%) received selective non-surgical management and the main injured organ was the lung [Group 1: 36 (33.0%), Group 2: 12 (34.3%), and Group 3: 12 (42.9%); p= 0.62], followed by the brain [Group 1: 42 (38.5%), Group 2: 12 (34.3%), and Group 3: 6 (21.4%); p=0.24] and the liver [Group 1: 7 (6.4%), Group 2: 3 (8.6%), and Group 3: 5 (17.9%); p=0.17]. No differences were found between the groups in the distribution of affected organs.
Simple X-Rays were performed during the primary evaluation in 113 patients (42%) prior to whole-body computed tomography, which did not cause any delay in the transfer of the patients and were mainly indicated in cases of pelvic or head trauma as an earlier approach to rule out life threatening injuries. Time between arrival to emergency department and completion of the whole-body computed tomography was under 30 minutes in most patients [Group 1: 28 minutes (IQR: 14-55), Group 2: 29 minutes (IQR: 16-57), and Group 3: 31 minutes (IQR: 13-50); p=0.96]. The average time between whole-body computed tomography and the diagnosis of injuries was 22 minutes, with no differences among the groups [Group 1: 22 minutes (IQR: 14-34), Group 2: 21 minutes (IQR: 12-32), Group 3: 23 minutes (IQR: 14-28); p=0.64].
Median radiation dose was within optimal range (< 20 mSv) in all groups [Group 1: 18 mSv (IQR: 13-27), Group 2: 19 mSv (IQR: 13-41), and Group 3: 15 mSv (IQR: 12-23); p=0.56] (Table 3). Ninety-one (34%) patients required surgical intervention and no statistical difference was found regarding the surgical intervention rate among the groups [Group 1: 59 (35.1%), Group 2: 15 (30%), and Group 3: 17 (37.7%); p=0.23]. The days of mechanical ventilation and hospitalization were similar between all groups. We found no differences regarding mortality rates [Group 1: 26 (15%), Group 2: 13 (26%), and Group 3: 6 (13%); p=0.17] and none of them died in the scanner (Table 4). No statistical difference was found between calculated and real survival rate [Group 1: TRISS 86.4% vs. real survival rate 85% (p=0.69); Group 2: TRISS 69% vs. real survival rate 74% (p=0.25); Group 3: TRISS 93% vs. real survival rate 87% (p=0.07)].
Table 3 Whole-body computed tomography to diagnosis time (minutes), radiation exposure and renal fuction evaluation.
| Variable | Total (n=263) | Blunt Trauma - Hemodynamically Stable (n=168) | Blunt Trauma - Hemodynamically Unstable (n=50) | Penetrating Trauma (n=45) |
|---|---|---|---|---|
| ED X-Ray, n (%) | 113 (42.9) | 63 (37.5) | 26 (52.0) | 24 (53.3) |
| ED to WBCT time* median (IQR*) | 29 (14-55) | 28 (14-55) | 29 (16-57) | 31 (13-50) |
| WBCT to diagnosis time, median (IQR) | 22 (14-32) | 22 (14-34) | 21 (12-32) | 23 (14-28) |
| Radiation mSv* median (IQR) | 18 (12-27) | 18 (13-27) | 19 (13-41) | 15 (12-23) |
| Radiation mGy.cm2*, median (IQR) | 2114 (1646-2730) | 2156 (1780-2911) | 2114 (1621-2730) | 1935 (977-2471) |
| Creatinine, median (IQR) | 1.0 (0.9-1.2) | 1.0 (0.8-1.2) | 1.2 (0.9-1.6) | 1.1 (0.9-1.2) |
| Contrast Induced Nephropathy, n (%) | 1 (0.4) | 1 (0.6) | 0 (0) | 0 (0) |
| Dialysis, n (%) | 7 (2.7) | 3 (1.8) | 2 (4.0) | 2 (4.4) |
* IQR=interquartile range, mSv=millisievert, mGy.cm2= milligray/cm2
Group 1: blunt trauma and hemodynamically stable
Group 2: blunt trauma and hemodynamically unstable
Group 3: penetrating trauma hemodynamically stable or unstable
ED: Emergency Department
WBCT: whole-body computed tomography
Table 4 Clinical outcomes
| Variable | Total (n=263) | Blunt Trauma - Hemodynamically Stable (n=168) | Blunt Trauma - Hemodynamically Unstable (n=50) | Penetrating Trauma (n=45) |
|---|---|---|---|---|
| SOFA*- day 2, median (IQR)* | 3 (1-7) | 3 (1-7) | 6 (3-9) | 2 (1-7) |
| Multiorgan failure, n (%) | 80 (30.4) | 47 (27.9) | 22 (44.0) | 11 (24.4) |
| ICU stay*, median (IQR) | 4 (1-8) | 4 (1-8) | 5 (2-10) | 3 (1-8) |
| Mechanical Ventilation days, median (IQR) | 2 (0-5) | 2 (0-4) | 2 (1-5) | 1 (0-3) |
| Hospitalary stay, median (IQR) | 7 (3-13) | 6 (3-12) | 9 (3-19) | 7 (2-14) |
| Mortality, n (%) | 45 (17) | 26 (15) | 13 (26) | 6 (13) |
| Predicted Survival Rate (TRISS*) | 86.4% | 69% | 93% | |
| Real Survival Rate | 85% | 74% | 87% | |
| p value | 0.69 | 0.25 | 0.07 |
*SOFA= sequential organ failure assessment,
IQR=Interquartile range,
ICU=Intensive Care Unit,
TRISS=Trauma and Injury Severity Score
Finally, all patients who had findings on the computed tomography of injuries that required surgical repair were taken to the operating room had positive findings during surgery that required repair. Sixty-seven patients (25%) of the non-surgical treatment group required a follow-up selective computed tomography (organ-specific), most of which were brain computed tomography’s to evaluate possible progression of traumatic brain lesions detected during the first whole-body computed tomography, but none of them required a subsequent surgical intervention.
Discussion
Our newly developed Single-Pass whole-body computed tomography Protocol has proven to be a useful and safe diagnostic tool for initial evaluation of patients with blunt and penetrating trauma, independent of their hemodynamic status. Unlike other protocols used around the world, ours allows us to have both arterial and venous phases on a single image (including the neck) which in turn can detect and diagnose a source of active bleeding, giving valuable information to the treating surgeon 9,10,14,25-27. Whole-body computed tomography was proven to be safe in our patients given that just 1 patient out of 263 (<1%) developed contrast induced nephropathy and the total radiation dose was considered standard [18 msV (IQR: 12-27)]. We also proved it to be effective because the results obtained from the scan was the determining factor to perform non-surgical management in more than 65% of patients regardless of trauma mechanism, thus avoiding non-therapeutic surgical interventions. Whole-body computed tomography was also efficient because the time between arrival and whole-body computed tomography completion was less than 30 minutes, and the time between acquisition and definitive diagnosis was close to 22 minutes in all groups.
Imaging protocols vary around the world and an ongoing open debate remains on the most suitable technique. Our new protocol is different from those previously described in the literature. Usually, whole-body computed tomography is performed as a multi-pass computed tomography acquisition technique with separated helical CT phases of different body zones 10-15. Contrast medium is usually used for the thorax, abdomen and pelvis. Nguyen, et al. showed that Single-pass whole-body computed tomography decreased the acquisition time in 42.5% compared to conventional whole-body computed tomography 16. Unfortunately, the use of single-pass protocols is not yet universal and instead two or more passes are required to obtain arterial and venous phases 27. A Single-Pass Continuous Whole Body computed tomography-scan protocol allows biphasic application of contrast medium in 1 minute and 27 seconds, with acquisition of an image in a single-pass with high resolution of arterial and venous phases (Figure 1), with excellent visualization of heart and great vessels of the chest (Figure 2A), veins and arteries of the neck (Figure 2B), abdomen and pelvis (Figure 2C). This highlights the fact that whole-body computed tomography as a diagnostic tool is essential in diagnosing patients efficiently and promptly visualizing any vascular injury (Figure 3).
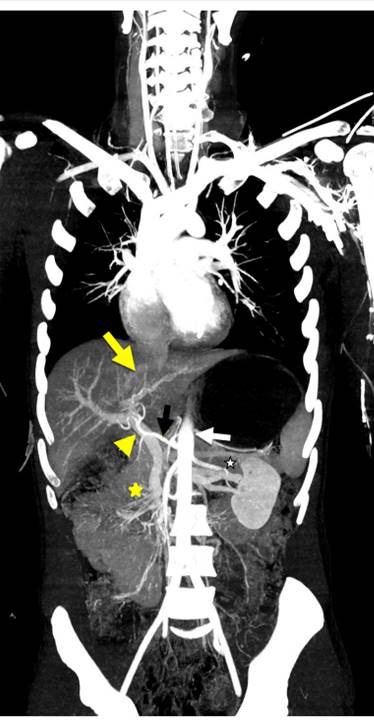
Figure 1 Coronal MIP reconstruction of Single-Pass WBCT. The aorta (White arrow) and hepatic artery (yellow arrow), with higher intensity than portal vein (yellow arrow head), and, median juxtahepatic vein (thick yellow arrow) with the lowest intensity. Also, mesenteric vein and artery (yellow star), and left renal vein and artery (white star) are visualized.
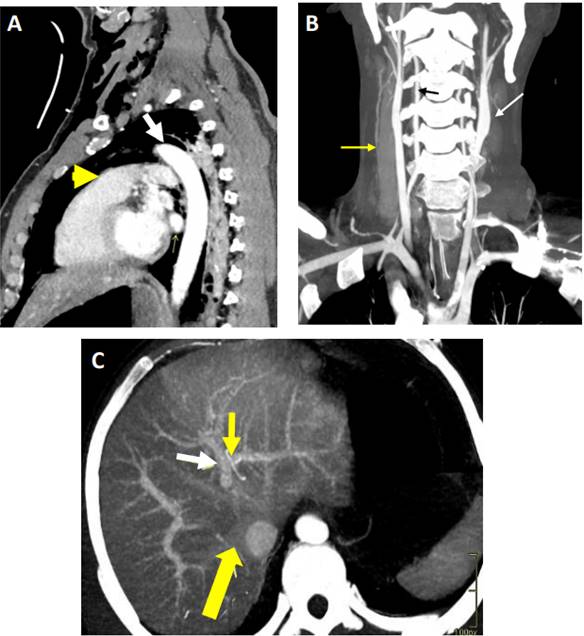
Figure 2 Visualization of solid organ and hollow viscous with Single-Pass WBCT. A) Sagital MIP reconstruction, right and left ventricles, right ventricle outlet tract (thick yellow arrow), left pulmonary vein (thinner right yellow arrow) and aorta (white arrow) are visualized. B) Coronal MIP reconstruction of neck, subclavian arteries, common carotids (white arrow), jugular veins (yellow arrow) and vertebral arteries (black arrow) are observed. C) Axial MIP reconstruction of liver and its vessels, aorta, right yuxtahepatic vein flowing into vena cava (thick yellow arrow), portal left branch (white arrow) and left hepatic artery (upper thin yellow arrow).

Figure 3 Coronal MIP reconstruction of the pelvis and abdomen. Patient with superior pubic rami fractures (yellow arrows), no associated injuries to adjacent external iliac arteries or veins (white stars).
Despite the multiple benefits of whole-body computed tomography over selective computed tomography in trauma patients, there is still uncertainty on its use in hemodynamically unstable trauma patients. This fear is based on the concept that whole-body computed tomography requires time which draws away from the prompt surgical management of these patients 15,16,28,29. However, our findings suggest that whole-body computed tomography can be used in patients with hemodynamic instability because the damage control resuscitation of the patient can be continued in and during the scan by the treating trauma staff. This implies a paradigm shift, because we have found that the use of this tool in a controlled setting is possible with an available trauma team that can continue with intravenous resuscitation while in the scanner and eventually securing prompt transfer of the patient to the operating room when warranted or to the Intensive Care Unit or angio suite in cases of non-operative management 30. Furthermore, we found that operative management occurred at a rate of 34% among all groups regardless of trauma mechanism and hemodynamic status. This translates to the fact that patients with either penetrating or blunt trauma had the same chance of requiring surgery which is in stark contrast to the standard belief that surgical intervention is usually required in most patients with penetrating trauma. It is important to highlight that although whole-body computed tomography is a valuable diagnostic adjuvant, it should not be used in all patients, a careful selection of patients with precise indications should be carried out, and this is why, the creation and implementation of an institutional whole-body computed tomography protocol is essential for it’s appropriate application.
Finally, radiation exposure is a widely discussed topic when considering the disadvantages of whole-body computed tomography. The radiation exposure of our patients was within the values considered optimal (10-20 mSv) 28. Therefore, even though, the performance of WBCT implied an increase in radiation exposure, it seems not to be significant enough to increase the lifetime risk of cancer but rather benefited the immediate triage of the patient to the appropriate treatment required during his or her trauma admission.
Limitations
Our study carries several limitations associated to its observational nature. The groups were heterogeneous by mechanism of injury and hemodynamic status making them not completely comparable and elevating the bias risk. Whole-body computed tomography is not widely performed in Colombia because of a significant lack of resources and availability, which in turn made the implementation of this protocol challenging. More evidence of the utility of this diagnostic tool and of our newly devised whole-body computed tomography Protocol is necessary with large randomized controlled trials to definitively assess the safeness, effectiveness and efficiency of this Single-Pass whole-body computed tomography.
Conclusion
Our new Single-Pass whole-body computed tomography Protocol proved to be safe and efficient to decide whether our patients with severe trauma requires surgical intervention, independent of mechanism of injury or hemodynamic stability. The use of this Single-Pass protocol in our institution allowed for a reduction in the time to diagnosis, a reduction in radiation exposure and facilitated the accurate diagnosis of potentially life-threatening traumatic injuries.

