











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Remark
| 1. Why was this study conducted? |
| To provide a summary of available diagnostic tests for SARS-CoV-2 for a better understanding and use of these tests. |
| 2. What were the most relevant results of the study? |
| We describe the different tests that identify viral RNA, viral antigen, and host antibodies against viral antigens; what these tests are useful for and their characteristics. |
| 3. What do these results contribute? |
| This is a summary of diagnostic tests for SARS-CoV-2 that can be used to get a better understanding of the different tests and protocols available for SARS-CoV-2. |
Introduction
In the past four months SARS-CoV-2 has reached most countries in the world. Countries have struggled to slow down its transmission with a common goal to avoid saturation of health care systems and reduce the economic impact of quarantines and other isolation measures. COVID-19 diagnostic testing is an important component of strategies to reduce transmission of SARS-CoV-2 1. The world learned from experiences in Singapore, Taiwan, Hong Kong, and South Korea, where screening tests for the general population occurred, that widespread testing help reduce local transmission of SARS-CoV-2. Identification of positive cases can lead to proper timely isolation, adequate monitoring and quarantine of case contacts, and to the implementation of strategies to reduce transmission in health care centers/institutions were cases concentrate (e.g., closure and decontamination of high-risk areas) 2.
Confirmatory tests
SARS-CoV-2 infection confirmatory diagnosis is based on polymerase chain reaction (PCR) testing that amplifies and identify viral RNA sequences. In some cases PCR may not be able to detect viral RNA due to early onset of symptoms, issues with sampling and handling of samples, quality of the kit, or test performance 3. In these cases chest computed tomography has been suggested as a complementary diagnostic tool 4,5. In January 2020, the WHO designed and started distributing a quantitative reverse-transcriptase-based PCR (RT-PCR) test for detecting SARS-CoV2 1. To date, different RT-PCR assays, along with other SARS-CoV-2 diagnostic assays, are available 6,7 with other tests kits being developed.
RT-PCR testing usually takes 4 to 6 hours to complete, it is complex and requires a high level of laboratory expertise. In addition, RT-PCR is expensive (compared to serological testing) and requires high-level personnel training to obtain and process patient samples, usually lower respiratory tract samples with higher and more prolonged levels of viral RNA, which are more difficult to obtain 8. Because of these complexities, RT-PCR testing is usually centralized in specialized laboratories. However, testing centralization slows down the identification of cases, as it requires special handling and shipping of clinical samples from regions to the laboratories in major cities. For example, evidence shows that centralized PCR testing in Colombia, at the Instituto Nacional de Salud, during the first weeks of transmission of SARS-CoV-2 in the country lead to important delays (up to 11 days) to obtain confirmatory diagnoses 9. This slowed down reaction times to conduct public health measures across regions.
Alternatively, new developments in rapid and automated point-of-care RT-PCR assays (although more costly due to equipment and reagent kits costs) can provide tests results in minutes. For example, the Xpert® Xpress SARS-CoV-2 test (Cepheid) 10 targets multiple regions of the viral genome and can provide results in 45 minutes using the GenXpert benchtop system. Also, the recent developed Abbott ID NowTM COVID-19 test uses isothermal nucleic acid amplification technology and provides positive results in just 5 minutes 11. Tests are run in the ID NOW, a small, lightweight and portable platform that can be used in wide range of healthcare settings. To date, the Abbott ID NowTM COVID-19 test is only available in the United States (50,000 tests are being produced every day), but is expected that it will soon be available in other countries.
Antigen testing
Monoclonal antibodies against SARS-CoV-2 antigens, such as the nucleocapsid (N) protein and the S1 or S2 domains of the spike (S) protein, can also be used to detect viral infection 12. Antigen testing is performed in lateral flow immunoassays using nasopharyngeal or oropharyngeal swab samples 2. An advantage of antigen testing is that they are available in rapid test kits that are easy to use and can provide results in 20-60 minutes. However, given that they do not replicate viral RNA sequences, there is concern about their sensitivity 2 (sensitivity is the ability of a test to identify correctly those with the infection, compared to a gold standard, such as RT-PCR) (Appendix 1) 13. Also, the development on monoclonal antibodies requires more time than that to develop other tests (e.g., antibody testing), and although promising, accurate tests to identify SARS-CoV-2 antigens are not yet available 2,14.
Antibody serological immunoassays
Serological immunoassays are a low-cost alternative that can be widely used at the community level, and that can provide results in 15 to 20 minutes. Serological immunoassays (including rapid lateral flow immunoassay, automated chemiluminescence immunoassay and manual ELISA) 15 use immobilized recombinant viral proteins/domains of viral proteins to which human antibodies bind if present in the blood. A positive test indicates that the person has antibodies against the virus, offering an indirect measure of past/current viral infection 1. Because blood samples (including blood from finger pinprick) can be used in these tests, it requires less intensive training to obtain and process samples, and to interpret results. To date, multiple serological test strips, for Immunoglobulin M (IgM) and G (IgG), are available in the market (many more are in the development/certification process), and are being approved for use in different countries 1,2,16.
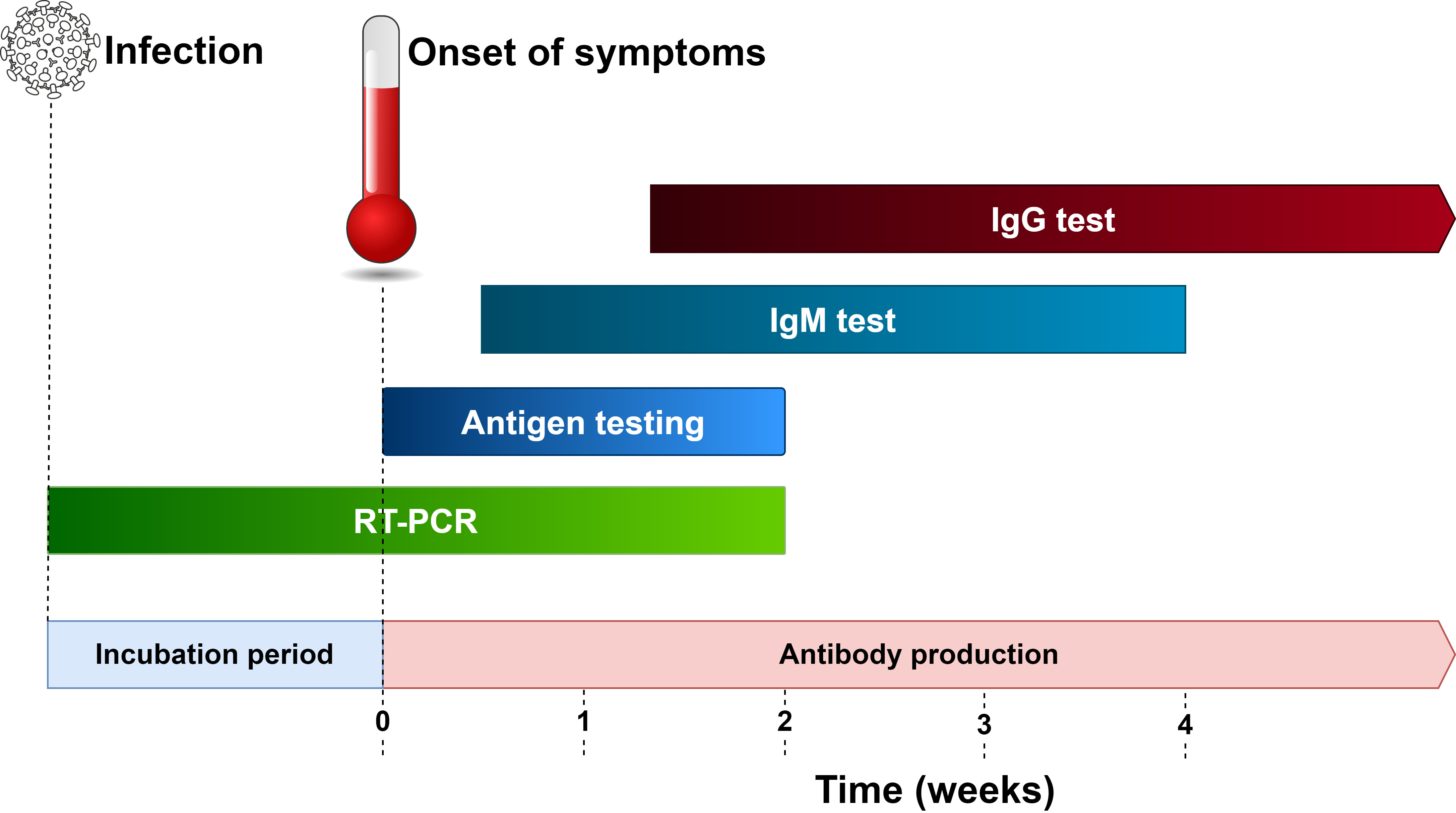
Serological immunoassays are considered screening rather than confirmatory tests. Because they measure antibodies in patients’ blood, plasma or serum, their sensitivity can vary greatly across disease stages. It is known that antibody response can take several days 17, for example IgM against SARS-CoV-2 can be first detected, on average, from 5 to 10 days, after the onset of symptoms, and IgG around 10 days after onset of symptoms (Figure 1) 17. This causes the sensitivity of serological tests to be lower in initial stages of the disease, with a number of those infected with the virus testing negative (false negatives). However, the sensitivity increases as the body produces antibodies against the virus, leading to a reduction in false negatives.
In addition, some individuals exposed to other coronaviruses, but not to SARS-CoV-2, may test positive for SARS-CoV-2 in serological immunoassays (false positives). This occurs because patients’ antibodies against viral proteins from other coronavirus can also bind to SARS-CoV-2 proteins used in these tests.
Testing sensitivity and specificity of serological immunoassays vary across available kits. For example, a study shows that the overall testing sensitivity of the COVID-19 IgM/IgG Rapid Test 18, which simultaneously tests for both IgM/IgG, was 88.66% and the specificity 90.63%, when using blood samples from 397 PCR confirmed cases and 128 negative patients 18. Recent developed rapid lateral flow immunoassay kits also claim to have high sensitivity (97.2%-100%) and specificity (98-100%) for IgG, but lower sensitivity (85-91.8%) and high specificity (96%-100%) for IgM 19-21, although this evidence is not supported by published studies. A recent study conducted in the United States shows evidence of the sensitivity and specificity of different commercial kits 22. Detailed information on available serological immunoassays for SARS-CoV-2 is available elsewhere 1,2,16.
Despite the described limitations of serological immunoassays, adding serological tests to the diagnostic toolbox, along and not instead of RT-PCR, is paramount to confront the epidemic, especially considering the complexity of PCR procedures and the common shortages of supplies of key reagents to run these tests 2. Serological testing can help screen presumptive cases for isolation purposes, but it can also help those with immunity to the virus to leave their homes, get back to work and take care/help others in need. Serologic immunoassays are also useful for ongoing surveillance and studies on vaccine effectiveness 7. Individuals who are immune to the virus, with detectable antibodies against SARS-CoV-2, could also provide plasma to treat patients, as some studies demonstrate this type of treatment may improve health outcomes in patients with severe respiratory symptoms 23,24.
In conclusion, multiple available protocols and kits provide solutions to diagnose SARS-CoV-2 infection. Testing is a key strategy to reduce viral transmission, not only for this pandemic, but also for others to come. Countries can be prepared to fight epidemics if they design or acquire appropriate tools to rapidly identify cases of infection, to then conduct appropriate clinical and public health actions that can minimize the burden that high-transmissible and deadly pathogens pose on human populations.

