











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Remark
| 1) Why was this study conducted? |
| Preeclampsia is a multiorgan disorder that is significantly associated with maternal and perinatal morbidity and mortality. Preeclampsia is defined by the presence of new-onset hypertension and proteinuria in women who are at least 20 weeks pregnant. The etiology of preeclampsia remains unknown; its clinical presentation and dynamics vary, and no method can predict its occurrence. In Peru, preeclampsia incidence is greater than 10%, and it accounts for 22% of maternal deaths. Genome and genetic epidemiologial studies have found an association of preeclampsia and certain gene polymorphisms and variants. In this study, we evaluated the susceptibility gene polymorphisms related to endothelial function, angiogenesis, immunologic and inflammatory processes, and metabolic syndrome in Peruvian preeclamptic women. |
| 2) What were the most relevant results of the study? |
| No association was found between the studied genetic markers and preeclampsia. However, in the -174G/C polymorphism of the IL6 gene, significant differences mainly in the GG genotype and G allele were found, wherein the frequencies were higher in the cases than in the controls. |
| 3) What do these results contribute? |
| This study contributes to our knowledge of the genetic factors associated with preeclampsia, an emergent research topic in Peru. High genetic mixing and other factors may partially explain the conflicting findings for the Peruvian population. |
Introduction
Hypertension is the most frequent medical complication of pregnancy 1, and the most severe clinical presentation of hypertensive disorders of pregnancy is preeclampsia, a condition that is significantly associated with maternal and perinatal morbidity and mortality.
Preeclampsia is the leading cause of maternal death in the western world. It is a multiorgan disorder involving new-onset hypertension (>140/90 mm Hg) and proteinuria in women who are at least 20 weeks pregnant 2. The clinical presentation and dynamics of preeclampsia are variable; for instance, hypertension and proteinuria may not always be present 3. In the absence of proteinuria, preeclampsia diagnosis is based on the occurrence of hypertension accompanied by low platelet count (below 100,000/mL), abnormal liver function (indicated by serum transaminase levels that are twice the normal concentrations), kidney failure (indicated by serum creatinine level exceeding 1.1 mg/dL or by serum creatinine levels that are twice the levels in the absence of other renal diseases), pulmonary edema, or de novo presentation of cerebral or visual alterations 2.
Preeclampsia affects 3% to 8% of pregnant women, depending on the population and region being studied and on the definition of preeclampsia being used 4,5. In Peru, preeclampsia incidence is greater than 10% in various regions 3), and it accounts for 22% of all maternal deaths.
The common factors associated with preeclampsia development in developed countries are obesity, insulin resistance and hyperlipidemia, whereas in developing countries, the associated factors are ethnicity, poor nutritional habits, subclinical infections, and other socioeconomic characteristics 6.
The etiology of preeclampsia remains unknown. However, it has been found that genetic factors cause a defective immune adaptation 7, which in turn leads to inadequate trophoblast invasion and inappropriate placenta development. Abnormal endometrial cytotrophoblast infiltration generates arterial disorders, such as loss of elasticity that affects vascular remodeling and impairs the fetus’s blood supply 8,9. Placental ischemia and hypoxia as well as oxidative stress and endotheliosis then develop 6, compromising the placenta and important maternal organs and systems. Oxidative stress stimulates the syncytiotrophoblast to release proinflammatory cytokines, exosomes, antiangiogenic factors, and cell-free fetal DNA into the maternal circulation 4,10.
Complications can emerge at any point during pregnancy, frequently surreptitiously and severely. Prior to the development of a clinical disease, vasospasm, activation of the coagulation cascade, and reduction in plasma volume occur. There are more harmful effects when preeclampsia appears early, including intrauterine growth retardation (IUGR) and prematurity 3. Moreover, placental senescence is accelerated 11, the concentration of pro-inflammatory cytokines, cell-free DNA, leptin, placental apoptotic debris and soluble fms-like tyrosine kinase 1 (sFLT1) in maternal blood increases, and placental growth factor (PlGF) levels decrease 12.
There is no method that can predict the onset of preeclampsia, and there is no cure for this condition other than the delivery of the fetus and the placenta. Preeclampsia usually resolves soon after delivery. However, epidemiological studies have associated preeclampsia with metabolic, cardiovascular and cerebral disorders 2,13-15 that will appear later in the mother and child, and this association has a great impact on disability and heathcare expenditure eventually 15-17.
Genome and genetic epidemiology studies have found an association between preeclampsia and certain genes 7,18, polymorphisms and other molecular and inflammatory markers 7,8,19,20. Thus, detecting these biomarkers early in gestation will allow us to predict and manage preeclampsia properly.
Several pro- and anti-angiogenic proteins are produced in the placenta from the beginning of pregnancy; these substances play a role in endothelial dysfunction and the risk of preeclampsia 9,20. The most important angiogenic factors 21,22 include the vascular endothelial growth factor (VEGF) 22 and the placental growth factor (PGF) 23. Antiangiogenic substances are abundantly expressed in preeclampsia and cause maternal endothelial cell dysfunction and damage 1,3,24, which have negative consequences to a mother and her fetus. The genes encoding for the important antiangiogenic factors include the soluble tyrosinase-like factor (sFLT-1) gene, the VEGF soluble Fms-like tyrosine kinase -1 (VEGFR-1) 25 gene, and the endothelin-1 gene polymorphisms 26,27.
Due to the high prevalence of preeclampsia in Peru and considering that oxidative stress induces the syncytiotrophoblast to release pro-inflammatory cytokines, exosomes, anti-angiogenic factors, and cell-free fetal DNA into maternal circulation 4,10, we decided to characterize some of these biomarkers in preeclamptic Peruvian women and verify whether these biomarkers can be applied to predict, prevent and manage preeclampsia among Peruvian women. We studied some genes and polymorphisms involved in preeclampsia, including the VEGF +936C/T and +405G/C polymorphisms, interleukin-6 (IL-6) gene polymorphisms, IL-1β gene -511C/T polymorphism 28, and polymorphisms of both the Apo A-1 and Apo B-100 genes, in preeclamptic and healthy Peruvian pregnant women. Our findings increase our knowledge of the genetic factors associated with preeclampsia, an emergent research topic in Peru.
Materials and Methods
This study is an observational associative case-control study performed between 2012 and 2018. The participating institutions were the Institute of Clinical Investigations and the Biochemistry and Nutrition Research Center of the Faculty of Medicine, National University of San Marcos, Lima, Peru. Subjects were recruited from the Hospital Docente Madre-Niño San Bartolomé, a public institution that is managed by the Peruvian Ministry of Health.
A preeclamptic woman was defined as a pregnant woman with a blood pressure of >140/90 mm Hg and proteinuria of ≥300 mg/24 h (>1+ dipstick) according to the International Federation of Gynecology and Obstetrics classification, which was updated in the year 2000 1.
The sampling method was non-probabilistic (for convenience). The inclusion criteria for the preeclampsia group were as follows: pregnant women aged ≥18 years who had been diagnosed with severe preeclampsia in the second half of pregnancy as confirmed by clinical and laboratory data and who had signed an informed consent. Pregnant women without proteinuria or those with chronic hypertension, diabetes, and other medical conditions as well as those with incomplete information were excluded. For the control group, the inclusion criteria were as follows: pregnant women aged ≥18 years who were apparently healthy without preeclampsia and without relevant diseases and who signed the informed consent. Table 1 presents the number of cases and controls studied for each gene polymorphism.
Table 1 Number of preeclamptic women and controls included in the study.
| Gene | Polymorphism | Preeclampsia | Control | Total |
|---|---|---|---|---|
| VEGF | +936 C/T | 45 | 49 | 94 |
| +405 G/C | 39 | 45 | 84 | |
| IL-6 | -174 G/C | 20 | 39 | 59 |
| IL1β | -511 C/T | 49 | 50 | 99 |
| Apo A-1 | -75 G/A | 47 | 45 | 92 |
| Apo B-100 | 2 488 C/T (Xbal) | 47 | 45 | 92 |
We obtained approval for our study protocol from the Ethics Committee of the Faculty of Medicine of the National University of San Marcos and from the ethics committee of the participating hospital. An ad hoc clinical file was filled with mother and newborn data. Written informed consent was obtained from all participants. Blood samples (5 mL) were drawn from the participants’ antecubital vein, and the samples were kept in a refrigerator and then transported to the laboratory. The blood samples were subjected to DNA extraction with the commercial kits used for genotype and allele determination for the investigated genes.
The maternal data entered in the ad hoc file were as follows: age, marital status, height, weight, personal medical history (hypertension, previous preeclampsia, diabetes mellitus, neuropathy, cardiopathy, and metabolic syndrome), family medical history (hypertension, diabetes mellitus, obesity, metabolic syndrome, and other conditions), number of pregnancies, preterm deliveries, low-weight newborns, hemoglobin levels, type of delivery, gestational age at delivery, and hospital stay (in days). The newborn data obtained were as follows: weight, Apgar scores at 1 and 5 min, gestational age, complications (fetal distress, respiratory distress, and perinatal asphyxia), IUGR, prematurity, respiratory distress syndrome, jaundice, infection, fetal death, neonatal death, malformations, and hospital stay (in days).
In the genetic molecular analysis, the PCR-RFLP technique was used, specific protocols was employed for each gene, and adequate laboratory conditions were ensured. The genotypes of the polymorphisms were confirmed by automated Sanger sequencing.
VEGF gene +936C/T and +405G/C polymorphisms
The specific primers F: 5’AAGGAAGAGGAGACTCTGCGCAGAGC3’ and R: 5´TAAATGTATGTATGTGGGTGGGTGTGTCTACAGG3´ were used for the +936C/T amplification, and the NlaIII enzyme was used for digestion according to the protocol of Papazoglou 29. For +405G/C, the primers F: 5’CCGACGGCTTGGGGA GATTGCTC3’ and R: 5’CGGCGGTCACCCCCAAAAGCAG3’ were used for amplification, and the BsmFI enzyme was used for digestion according to the protocol of Banyasz 30 and Garza-Veloz 31.
IL-6 gene -174G/C polymorphism
The specific primers F: 5´TGACTTCAGCTTTAC TCTTTGT’3 and R: 5’CTGATTGGAAACCTTATTAGG’3 were used for amplification, and the restriction enzyme SfaNI was used fo digestion according to Berthold 32. The GG and GC genotypes obtained by PCR-RFLP and Sanger sequencing are reported in Figure 1.
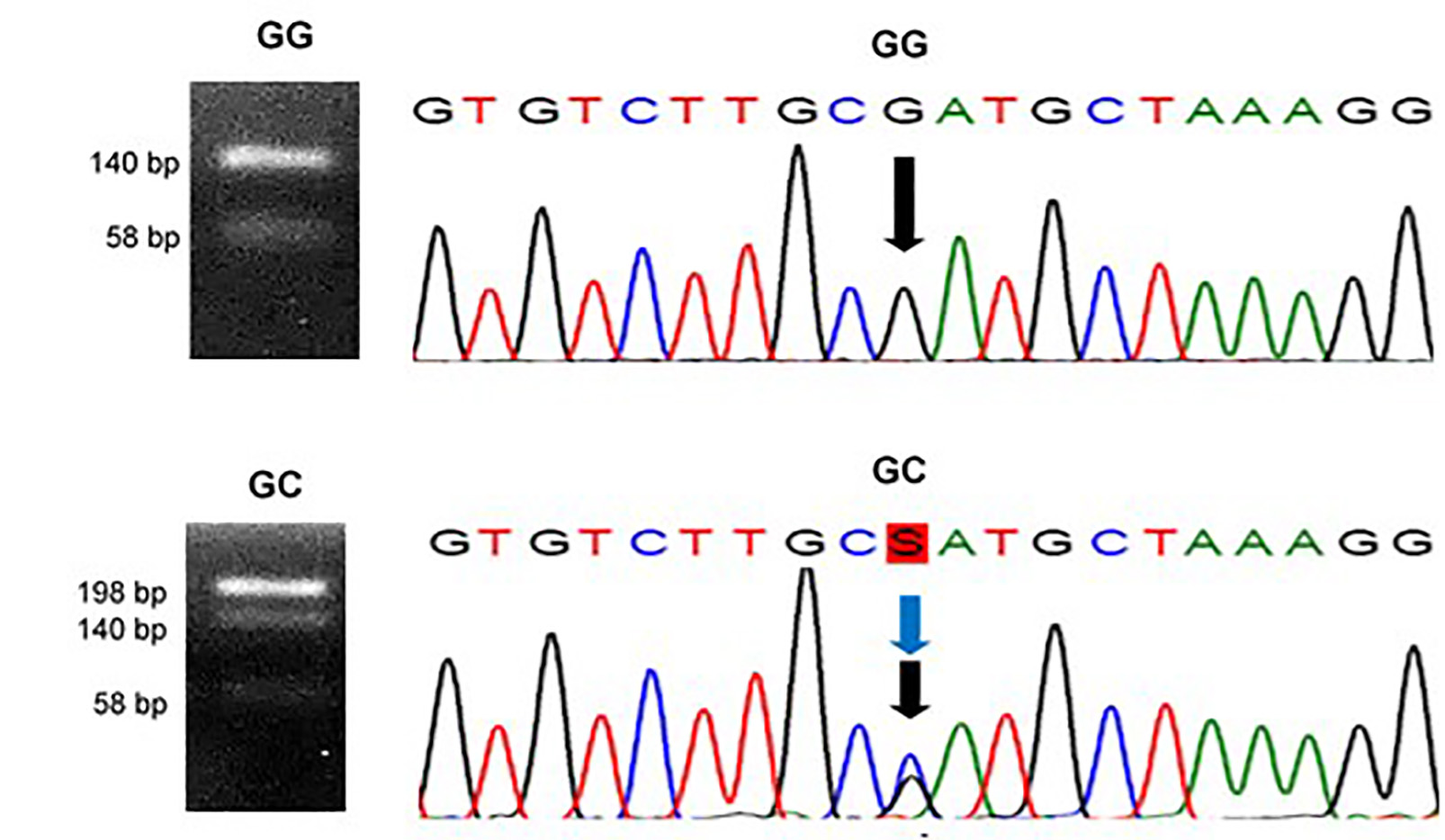
Figure 1 Determination of the genotypes of the -174 G/C polymorphism in IL6 gene. Left: Agarose gels with homozygous GG (140 and 58 bp) and heterozygous GC (198, 140 and 58 bp) genotypes as determined by PCR-RFLP with SfaNI as the restriction enzyme 32. Right: Chromatograms obtained by automated Sanger sequencing confirming the GG and CC genotypes (marked with arrows).
IL-1β gene -511C/T polymorphism
The specific primers F: 5′TGGCATTGATCTGGTTCATC3′ and R: 5′GTTTAGGAATCTTCCCACTT3´ were used for amplification, and the restriction enzyme Aval was used for digestion according to Acosta 28.
Apo A-1 gene -75G/A polymorphism
The specific primers F: 5′AGGGACAGAGCTGATCCTTGAACTCTTAAG3′ and R: 5′TTAGGGGACACCTACCCGTCAGGAAGAGCA3′ were used for amplification, and the restriction enzyme Mspl was used for digestion according to Ordovas 33.
Apo B-100 gene 2488C/T (XbaI) polymorphism
The specific primers F: 5′GGAGATATTCAGAAGCTAA3′ and R: 5′GAAGAGCCTGAAGACTGACT3′ were used for amplification, and the restriction enzyme XbaI was used for digestion according to Hu 34.
The data analysis involved the calculation of the allele and genotypic frequencies based on the assumption of the Hardy-Weinberg principle. Moreover, either the chi-square (Ji 2) or he Fisher’s exact test was applied to establish the association between genetic polymorphisms and preeclampsia based on p <0.05 and odds ratio (OR). We used IBM SPSS version 22.0, Arlequin version 3.5.2, and a genetic association software in our analysis.
Results
Adding all the participants of the preeclampsia projects between 2012 and 2017, 450 pregnant women were contacted, 22 of whom were excluded because of the following reasons: unmet inclusion criteria for either group, incomplete data, presence of a relevant disease, clotting of blood samples, unwillingness to participate, or failed sample amplification.
The results of allele and genotype frequencies, for the Hardy-Weinberg equilibrium, and for the association and statistical significance are presented in Table 2.
Table 2 Genetic variants in Peruvian pregnant women with preeclampsia and controls.
| Gene | Genotypes and alleles | Preeclampsia | Controls | OR | 95% CI | p a |
|---|---|---|---|---|---|---|
| n (%) | n (%) | |||||
| VEGF +936 C/T | CC | 19 (42.2) | 19 (38.8) | Reference | 0.062 | |
| CT | 12 (26.7) | 23 (46.9) | 0.523 | 0.203-1.341 | ||
| TT | 14 (31.1) | 7 (14.3) | 2.000 | 0.661-6.056 | ||
| C | 50 (55.6) | 61 (62.2) | Reference | 0.434 | ||
| T | 40 (44.4) | 37 (37.8) | 1.319 | 0.736-2.362 | ||
| GG | 7 (17.0) | 15 (33.3) | Reference | 0.256 | ||
| +405 G/C | GC | 27 (69.2) | 24 (53.4) | 2.411 | 0.842-6.904 | |
| CC | 5 (12.8) | 6 (13.3) | 1.786 | 0.403-7.906 | ||
| G | 41 (52.6) | 54 (60.0) | Reference | 0.356 | ||
| C | 37 (47.4) | 36 (40.0) | 1.354 | 0.734-2.498 | ||
| CC | 4 (20.0) | 13 (33.3) | Reference | 0.004 | ||
| CG | 7 (35.0) | 23 (59.0) | 0.989 | 0.243-4.028 | ||
| IL6 -174 G/C | GG | 9 (45.0) | 3 (7.7) | 9.750 | 1.744- 54.525 | |
| C | 15 (37.5) | 49 (62.8) | Reference | 0.011 | ||
| G | 25 (62.5) | 29 (37.2) | 2.816 | 1.281-6.191 | ||
| CC | 30 (61.2) | 29 (58.0) | Reference | 0.946 | ||
| CT | 18 (36.7) | 20 (40.0) | 0.870 | 0.385-1.968 | ||
| IL1B -511 C/T | TT | 1 (2.1) | 1 (2.0) | 0.967 | 0.058-16.192 | |
| C | 78 (79.6) | 78 (78.0) | Reference | 0.863 | ||
| T | 20 (20.4) | 22 (22.0) | 0.909 | 0.460-1.798 | ||
| GG | 13 (27.7) | 12 (26.7) | Reference | 0.832 | ||
| GA | 23 (48.9) | 20 (44.4) | 1.062 | 0.396-2.849 | ||
| APOA1 -75 G/A | AA | 11 (23.4) | 13 (28.9) | 0.781 | 0.254-2.400 | |
| G | 49 (52.1) | 44 (48.9) | Reference | 0.768 | ||
| A | 45 (47.9) | 46 (51.1) | 0.878 | 0.493-1.566 | ||
| X-X- (CC) | 28 (59.6) | 25 (55.6) | Reference | 0.676 | ||
| APOB100 | X- X+ (CT) | 12 (25.5) | 15 (33.3) | 0.714 | 0.282-1.813 | |
| 2488 C/T (XbaI) | X+X+ (TT) | 7 (14.9) | 5 (11.1) | 1.250 | 0.352-4.442 | |
| X- | 68 (72.3) | 65 (72.2) | Reference | 0.883 | ||
| X+ | 26 (27.7) | 25 (27.8) | 0.994 | 0.521-1.896 |
The genotype frequencies of the +936 C/T and +405 G/T variants of the VEGF gene and of the 2488 C/T (XbaI) polymorphism of the APOB100 gene in women with preeclampsia were in Hardy-Weinberg disequilibrium. a According to chi-square test or Fisher’s exact test.
The genotypic frequencies of the VEGF +936C/T and +405G/C polymorphisms in controls were found to be in Hardy-Weinberg equilibrium; however, in cases they were in disequilibrium, indicating the influence of other factors.
No association was found between genotypes and alleles of the VEGF +936 C/T polymorphism and preeclampsia (p= 0.062 and p= 0.434). The differences between genotypic and allelic frequencies of the VEGF +405 polymorphism in cases and controls were not significant (p= 0.256 and p= 0.356). However, we would like to highlight that the proportions of heterozygous GC (69.2%) and C allele (47.4%) were higher in the preeclamptic women than in the control.
As regards the allelic and genotypic frequencies of the IL-6 -174 G/C polymorphism, in Hardy-Weinberg equilibrium, showed different distribution patterns between the preeclamptic women and the controls. Under a codominant model, the GG genotype (OR= 9.750, IC 95%: 1.744-54.525, p= 0.004, with CC genotype as reference) and the G allele (OR= 2.816, IC 95%: 1.281-6.191, p= 0.011, with C allele as reference) are considered to be at risk and with significant differences, wherein the frequencies were higher in the cases than in the controls.
Regarding the -511C/T polymorphism of the IL-1β gene, no significant differences were found in the frequencies of the TT and CT+CC genotypes between the cases and the controls (p >0.946). The homozygous TT was the most frequent genotype (over 50%) in both groups. For the C and T alleles, the differences were not significant (p= 0.863).
The genotypic frequencies of the ApoA-1 -75G/A polymorphism in cases and controls were in Hardy-Weinberg equilibrium, as were the controls for the ApoB100 2488C/T (XbaI) polymorphism; however, preeclamptic pregnant women were in disequilibrium. Overall, genotype and allele frequencies for both ApoA-1 -75G/A and ApoB100 2488C/T (XbaI) polymorphisms, between cases and controls, did not show significant differences (p >0.05) and were not associated with preeclampsia.
Discussion
The cause of preeclampsia remains unknown, and no methods can prevent or treat this disease. Moreover, this obstetric complication may appear unexpectedly in any pregnant woman 3.
An association was observed between preeclampsia and family history of pregnant women, and a genetic factor is considered to be involved in its origin. Until 2012, 178 genes associated with preeclampsia had been described 35. In 2014, from among over 22 million PubMed records, 28,000 articles related to preeclampsia were found, including 729 articles about 535 genes and genetic variants with a “significant” association with preeclampsia 36.
Specific gene polymorphisms, including angiogenic and antiangiogenic factor genes, have been described in pregnant women with preeclampsia. One angiogenic factor is VEGF, which plays a crucial role in vasculogenesis and vascular permeability. It is usually expressed at optimal levels following an adequate blastocyst placentation 37,38. VEGF is genetically regulated; some allelic variations of which are possibly associated with preeclampsia, and some of its polymorphisms function as hypoxia-induced factors that play a role in preeclampsia 37. When placentation is defective, such as in preeclampsia and IUGR, VEGF levels are low 39. A decrease in VEGF levels may result in placental oxidative stress 40. Studies have attempted to determine the relationship between VEGF polymorphisms and preeclampsia 41,42, and some studies have associated these polymorphisms with endothelial dysfunction 43,44, preeclampsia severity 45, or HELLP syndrome 46. The association of some VEGF gene polymorphisms (30, such as +936C/T, with preeclampsia has also been reported 30,31.
However, no association of the VEGF +936C/T and +405G/C polymorphisms with preeclampsia was observed in the studied Peruvian pregnant women (p= 0.062 for +936C/T and p= 0.256 for +405G/C). In the +936C/T polymorphism, the mutant homozygous genotype TT was more frequent in the cases, whereas the heterozygous CT genotype was more frequent in the controls. The differences in the frequencies of C and T alleles in the cases and controls were not significant (p= 0,434), for the genotypes as well, but close to the limits of significance (p=0,062). In terms of the VEGF +405 polymorphism, the proportions of heterozygous GC (69.2%) and C allele (47.4%) were higher in the preeclamptic women than in the controls.
Some studies, such as those of Shim 47 and Papazoglou 29, have reported an association between VEGF polymorphisms and preeclampsia. By contrast, other researchers have found no association of preeclampsia with VEGF +936C/T polymorphism 48; with +813C allele 49; with VEGF rs699947, rs1570360, rs2010963, and rs25648 minor alleles 30; with eNOS and DDAH genes 50; and with VEGF -2578C/A, -634G/C, and 936C/T alleles. The 936C/T allele has been associated only with severe preeclampsia 45. In Latin America, Sandrim et al.51, have found an association of the − C2578A, -1154G, and -634C haplotypes with preeclampsia prevention, and a similar association with the C-2578A allele was found by Cunha et al. 48; both studies were conducted in Brazil. However, in Ecuador, Sandrim’s group has not found such an association with VEGF C2578A and G634C in the same way that Chedraui et al. 44, have not found the said association with the VEGF -2578 C/A, -1498 C/T, -1154 A/G, -634 C/G, and -936C/T polymorphisms 7.
Alterations in inflammatory cytokine and lipid profiles have been associated with the presence and severity of hypertensive disorders of pregnancy 28,52. Cytokines are proteins secreted by innate or adaptive immune cells, many of the functions of which are mediated by cytokines 53. The placenta expresses various pro- and anti-inflammatory cytokines, adipokines, and cytokine-like angiogenic growth factors. However, their production of these markers is altered in preeclampsia, at least partially due to hypoxia. It is postulated that endothelial dysfunction underlies the disease manifestations of preeclampsia 54. Endothelial cell activation seems related to impaired maternal immune response, placental ischemia 55, oxidative stress, and generation of inflammatory cytokines56.
One class of cytokines are ILs, which modify biological responses. The cytokines involved in the pathophysiology of preeclampsia 11,57,58 include IL-6 59, IL-1β 60-62, IL-17, and IL-35 63. Increased stress during pregnancy is a predictor of an elevated production of IL-1β and IL-6 pro-inflammatory cytokines by lymphocytes during the third trimester. This alteration in the cell function of the immune system increases the risk of preeclampsia and preterm delivery 64. Moreover, having a female fetus is associated with low levels of pro-inflammatory IFNγ and IL-12 cytokines in the first trimester and with increased levels of pro-inflammatory IL-1β and TNFβ, anti-inflammatory IL-4r, and regulatory IL-5 and IL-10 cytokines in the second trimester 65. Fetal sex is thus related to the variability in cytokine levels.
IL-6 is a cytokine produced by many innate immune cells, neutrophils, and monocytes/macrophages, and it is expressed during states of cellular stress, such as inflammation, infection, wound, and cancer 66. IL-6 is an important mediator of acute-phase immune response and of trophoblast proliferation, invasion, and differentiation 67,68. Studies have suggested that the IL-6 -174 promoter polymorphism is a major genetic regulator in the etiology of early-onset preeclampsia 69-73. A systematic review that included 73 articles and analyzed 57 unique markers has found that the proinflammatory markers IL-6, IL-8, and tumor necrosis factor alpha have garnered the most support as the potential inflammatory markers for the clinical surveillance of preeclampsia, particularly during the second and third trimesters 58.
However, conflicting results in relation to the role of circulating IL-6 in preeclampsia have been found 69. In Latin America, the Brazilian study conducted by Pinheiro et al. 72, has found an association of the IL-6 -174G/C allele with protection for preeclampsia; however, another Brazilian study conducted by Daher et al. 73, and a Mexican study by Valencia et al. (74, have found no association of this allele with the risk of preeclampsia. Our study on the -174G/C polymorphism of the IL-6 gene showed an association of preeclampsia risk with the GG genotype and the G allele in the preeclamptic Peruvian women. However, these results must be verified in a larger population.
IL-1 is secreted by macrophages, endothelial cells, and some epithelial cells, and it activates endothelial cell inflammation and coagulation. IL-1β gene polymorphisms have been associated with preeclampsia 62,63, preterm birth 75, and recurrent pregnancy loss 76. In their Brazilian study, Leme et al. 77, have found an association of preeclampsia risk with the IL-1β rs1143630 T allele, while Pontillo et al. 78, who also conducted their study in Brazil, have found no association of IL1β rs1143634 with preeclampsia risk, a finding similar to that of other studies 79. The -511 C/T polymorphism in the IL-1β gene promoter region is implicated in the differential production of cytokines. Moreover, it may be associated with the immune inflammatory response in obesity, dyslipidemia, cardiopathy, cancer, infections, and treatment with nutrients and drugs. The IL-1β gene -511C/T polymorphism has also been studied in Peruvian Mestizo, Amazonian, and Andean subpopulations 28, and the T mutant allele associated with an increased cytokine production was frequently observed in these subpopulations. In our study, no significant difference in frequency distribution of the IL-1β gene -511C/T polymorphism TT and CT+CC genotypes between cases (n= 49) and controls (n= 50) was found.
Plasma lipoprotein metabolism is regulated and controlled by the specific apolipoproteins (apo-), constituents of the various lipoprotein classes 80. Apolipoproteins regulate protein metabolism by transporting and redistributing lipids to cells and tissues. Lipoprotein A (LpA) is a low-density lipoprotein (LDL) particle modified with an apolipoprotein A (Apo A-1), the main component of the structural particles of high-density lipoprotein (HDL), which exhibits anti-inflammatory properties, inhibits LDL oxidation, and clears up excess cholesterol from macrophages 81,82. Apo A-1 also protects the trophoblast-endothelial cell integration in the presence of a pro-inflammatory stimulus. Women with preeclampsia have low Apo A-1 levels, which deter their ability to control LDL and inflammation 83,84. Apo B-100 represents the Apo B particles circulating in the body, and it is an LDL. The Apo B-100/Apo A-1 quotient has been proposed as a reliable parameter used to predict atherosclerosis and mortal events resulting from cardiovascular disease that is linked to lipid alterations 85.
Apo A-1 concentrations have been found to increase in normal pregnancy and to decrease in women with preeclampsia 84; thus, Apo A-1 concentrations are an important risk factor for atherosclerosis among preeclamptic women 86. Other researchers have found lower levels of Apo A-1 only in patients with severe preeclampsia 87. Apo B is considered a measure of atherogenic lipoproteins, and it can be used to predict the risk of atherosclerotic cardiovascular disease 88. However, no difference in Apo A-1 and Apo B levels was observed between preeclamptic and normal pregnant women 87,89. In our study on Apo A-1 and Apo B-100 genes, no significant differences in genotypes and alleles were found between the women with severe preeclampsia and the controls.
A higher Apo B/Apo A-1 ratio has been associated with an increased risk of preeclampsia 90. Timur et al. 91, have reported that preeclamptic patients display significantly low Apo A-1 levels and a high Apo B-100/Apo A-1 ratio and that they consider these parameters as useful markers. By contrast, Kharb et al. 92, have found that the serum and cord blood Apo A-1 and Apo B levels were lower in preeclamptic women than in normotensive pregnant women. We have found controversies in the literature regarding the levels of Apo A-1 and Apo B-100 and regarding the possible association of the Apo A-1/Apo B-100 ratio with preeclampsia. Nevertheless, studies have found an association of these gene polymorphisms with cardiovascular disease 93, dyslipidemia 94, osteonecrosis 95, and other disorders.
In this study, the Hardy-Weinberg disequilibrium of the genotype frequencies of the two polymorphisms of the VEGF gene as well as of the Apo B-100 gene in preeclamptic women may indicate population admixture and/or specific characteristics of the patients. However, the lack of association with preeclampsia was corroborated by the Armitage trend test, the result of which is valid even when the frequencies depart from the Hardy-Weinberg equilibrium.
The search for susceptibility genes has led to a drastic increase in the number of published studies associating genetic factors with preeclampsia. However, attempts to replicate the findings of these studies have produced inconsistent results, except for the genes ACE, CTLA4, F2, FV, LPL, and SERPINE1 (96.
Conclusions
The present study analyzed polymorphisms related to endothelial function, angiogenesis, immunological and inflammatory processes, and metabolic syndrome in Peruvian preeclamptic women. No association was found between the genetic markers studied and preeclampsia. However, the -174G/C polymorphism in the IL-6 gene presented significant differences mainly for the GG genotype and the G allele, whose frequencies were higher in the cases with respect to the controls; according to OR calculations, they would be risk factors. The limitation of the study of this polymorphism is the number of case samples (n=20), which should be a stimulus for further studies.
The contradictory results of the work can be partially explained by the genetic composition of the Peruvian population. Lima, the Peruvian city where the study was carried out, has a mixed population, characterized by a high Amerindian component, around 70%, and by European, Asian and African ancestry 97. Therefore, genetic ancestry and other variables, such as the sex of the fetus, can be considered in future research.
The present study contributes to a better understanding of the genetics of preeclampsia in Peru. Further research is needed to include larger populations of pregnant women and other Peruvian regions, as well as to comprise additional genes related to preeclampsia, a polygenic disorder.

