











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Lipemia retinalis is a pathognomonic sign of hyperchylomicronemia. This infrequent complication of chylomicron accumulation in retinal vessels 1 is observed when serum triglyceride levels exceed values of 2,000 mg/dL 2 and gives them a white and creamy appearance in ocular fundus examination. Initially, peripheral vessels are involved, and central retinal vessels are affected as severity increases 3.
It was first described by Dr. Albert G. Heyl in 1880 as intraocular lipaemia 4, who depicted salmon color of the retinal arteries and veins in relation to the abnormally high presence of fat in blood serum in contrast to the light color of the fundus oculi.
Although the exact epidemiology of lipemia retinalis is still unknown, it is estimated that approximately 23% of patients with severe hypertriglyceridemia may develop this clinical manifestation 1 due to deficiency or saturation of the enzyme lipoprotein lipase (LPL), which causes a sustained accumulation of circulating chylomicrons 2,5.
We present the case of a 40-year-old patient who came to the emergency department because of visual acuity alteration as a guiding symptom. The observation of milky-colored retinal vessels on a salmon-colored eye fundus and the inspection of a creamy layer of supernatant in the biochemical tube were essential to determine the diagnosis of hyperchylomicronemia, and perform an early treatment to achieve a prompt complete visual recovery.
Clinical case
We present the case of a 40-year-old male patient who came to the emergency department with a 14-day history of visual acuity alteration. As a previous history, the patient suffered from acute myeloid leukemia with diagnosis at the age of 5 years and was treated with high doses of anthracyclines after several recurrences. He underwent his father's HLA-incompatible allogeneic transplant, requiring high doses of cyclophosphamide, cytarabine, and total body radiation therapy. As a sequel of this treatment, he presented severe hypogonadism and decreased lung capacity. Six years before being attended in our hospital, he was diagnosed with normal functioning multinodular goiter, cervical Schwannoma and hepatitis C genotype 1b, F1 virus and received no treatment. The patient had no previous ophthalmological interesting history.
A routine endocrinology analysis detected hypertriglyceridemia 638 mg/dL (30-150 mg/dL) but the patient refused pharmacological treatment. Three years later, the value increased to 1,184 mg/dL, remaining fully asymptomatic with no treatment.
In this occasion, the patient is cared for in our service due to decreased visual acuity, headache and abdominal pain in the previous two weeks. The anamnesis revealed unhealthy dietary habits with frequent intake of carbonated drinks and dairy products. An intensely lipemic serum was obtained after blood extraction, in a way that the initial evaluation of biochemical analytical parameters was not achievable. Secondary processing of the sample, after the addition of 1,1,2 Trichlorotrifluoroethane, allowed to obtain the following results: 11,930 mg/dL triglycerides (30-150 mg/dL), 10,268 mg/dL chylomicrons, 1,490 mg/dL cholesterol (150-250 mg/dL), 304 mg/dL glucose (70-110 mg/dL) and 86 U/L amylase (1-100 U/L). Abdominal ultrasound and cranial and abdominal computerized axial tomography were performed, with normal results, except for some discrete inflammatory changes present in the pancreatic tail, compatible with acute allithiasic pancreatitis.
The symptom that most concerned the patient was the decrease in visual acuity, in the absence of intraocular pain even with ocular movements. The ophthalmological examination did not show xanthomas or xanthelasmas, and confrontational campimetry and oculomotor cranial nerve examination were normal. Visual acuity was estimated in right eye (0.8/1) and the left eye (0.5/1). Fundoscopy showed creamy retinal vessels with opalescent whitish appearance over a salmon-colored fundus, without associated papilledema, compatible with lipemia retinalis (Figures 1 and 2).
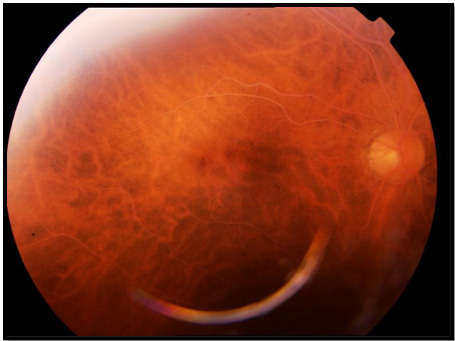
Figure 1 Retinography of the right eye: findings of whitening of all retinal vessels on a salmon-like fundus, compatible with severe lipemia retinalis (Vinger and Sachs Grade III).

Figure 2 Retinography of the left eye: whitening of all retinal vessels on a salmon-like fundus, compatible with severe lipemia retinalis (Vinger and Sachs Grade III).
The patient was hospitalized with a diagnosis of lipemia retinalis, acute pancreatitis secondary to severe hypertriglyceridemia, and incipient diabetes mellitus. During the stay, the patient remained stable and oligosymptomatic with serum therapy and analgesic, dietary, antidiabetic (insulin glulisine and rapid insulin) and lipid-lowering treatment (atorvastatin 40 mg/24 hours, Fenofibrate 200 mg/12 hours).
In the course of hospitalization, gradual decrease in triglyceride levels was detected, and visual acuity was recovered to almost 100% of its previous situation. Prior to medical discharge, an ophthalmological evaluation was performed and revealed positive clinical evolution and almost total disappearance of lipemia retinalis and complete recovery of visual acuity. In this way, 12 days after medical discharge, plasma triglyceride levels decreased to values of 529 mg/dL (30-150 mg/dL). Subsequently, ophthalmological follow-up after one- and two-months posterior to discharge, proved completely disappearance of lipemia retinalis. Six months later, the assessment was made by telephone contact, and the patient referred complete visual acuity; additionally, the endocrine progression was satisfactory after appropriate diet and with lipid-lowering and hypoglycemic treatment.
Discussion
Loss of visual acuity is a condition doctors must frequently deal with. Physical examination remains essential to achieve diagnosis in this kind of patients in those situations in which chylomicrons, such as triglyceride-rich lipoproteins levels, show very high levels, whenever no complementary tests are available to detect them, or results are delayed because of the need for dilution and sample processing to reach a final result. Lipemia retinalis is a nosological entity of simple diagnosis through direct visualization of the eye fundus, which will guide us to severe hypertriglyceridemia. An early diagnosis of this dyslipidemia can avoid ominous complications such as acute pancreatitis.
Loss of visual acuity in dyslipidemic patients is a rare clinical situation, but if it occurs, it will force us to urgently visualize the eye fundus. Once initial diagnosis by visual evaluation is performed, a differential diagnosis with several pathologies is mandatory. This includes leukemia, in which veins are pale red and the arteries are pale yellow, whereas in lipemia retinalis, the arteries and veins display the same color and can only be differentiated by caliber, being veins larger in diameter. A differential diagnosis should also be made with diabetic retinopathy, a condition that shows sclerosis of the retinal vessels, intravascular calcifications of the retinal vessels secondary to renal failure and hyperparathyroidism, whose main finding is detachment of the retina, occlusion of the vein or central artery of the retina, hypertensive retinopathy, and diffuse choroidal hemangioma, whose characteristic tomato sauce-like eye fundus may resemble the salmon fundus of those patients with lipemia retinalis.
On a superficial examination, retinal vasculitis should also be considered in the differential diagnosis; however, it is usually segmental and associated with perivascular infiltrates and signs of intraocular inflammation on examination. All these signs are absent in lipemia retinalis 1.
As previously described, visual acuity in patients with lipemia retinalis is not usually affected in the initial stages. However, it can be significantly reduced in more advanced stages 1,2,7,8. This suggests that real incidence may be underestimated. The presence of lipemia retinalis associated with other comorbidities such as diabetes mellitus, arterial hypertension and occlusion of the central retinal vein can cause a more intense loss of visual acuity. Persistent lipemia retinalis secondary to the absence of systemic lipid-lowering treatment can lead to massive lipid exudation with irreversible loss of vision 2.
Hypertriglyceridemia, considered as the elevation of serum triglyceride levels (higher than 150 mg/dL), is a very common pathology in the adult population, with a prevalence that reaches 30% 2,6. In addition to the possible long-term cardiovascular consequences, the immediate importance that a substantial elevation of triglycerides may have is related to the possibility of a sustained accumulation of circulating chylomicrons secondary to saturation of lipoprotein lipase. Acute pancreatitis and lipemia retinalis2 are among the complications that severe hypertriglyceridemia can produce in patients with levels higher than 2,000 mg/dL. Vinger and Sachs 3 described different grades of lipemia retinalis depending on triglyceride levels. Grade I (mild lipemia retinalis): white and creamy appearance of the peripheral vessels of the retina. Grade II (moderate lipemia retinalis): whitish, creamy vessels that extend into the optic disc. Grade III (severe lipemia retinalis): salmon-colored retina with all vessels showing a milky color.
Although a correct differential diagnosis must be made, the appearance of lipemia retinalis implies a significant increase in chylomicron and, consequently, triglyceride serum levels, being so a pathognomonic sign of this condition 1. However, not all patients with these characteristics develop this semiology, thus demonstrating that other factors might interfere, such as hematocrit and the difference in translucency of the retinal and choroidal vessels 2.
Our patient developed a significant decrease in visual acuity, probably due to the high triglyceride levels that he previously presented at the time of the onset of symptoms. Once lipid-lowering treatment was started, visual acuity and direct ophthalmoscopy progressively normalized. Patients with this clinical behavior have an excellent posterior ophthalmological prognosis 1.
Although systemic treatment is necessary in order to control the effects of hypertriglyceridaemia, there is no specific ophthalmological treatment for lipemia retinalis itself 1. According to the clinical guidelines for the management of hyperchylomicronemia, the ideal situation would be the achievement of triglyceride concentrations lower than 150 mg/dL. However, in daily practice, this is not realistic, so it is recommended as the main objective to maintain triglyceride concentrations below 500 mg/dL 9,10.
Some oral hypoglycemic agents, such as metformin, have beneficial effects in lowering plasma triglyceride levels 9. That is the reason why, in addition to high blood glucose levels, this treatment was introduced at medical discharge.
It is interesting to highlight the history of acute myeloid leukemia that the patient initiated at 5 years of age, when he received high doses of chemotherapeutic antineoplastic drugs and total body radiotherapy. One of the secondary causes of hyperchylomicronemia is total body radiation after neoplastic processes, as well as a previous history of immunosuppressive treatments 9,11. This predisposition was favored by unhealthy dietary habits that contributed to the development of the clinical process.
At present day, the patient remains under lipid-lowering and hypoglycemic treatment and correct dietary habits, as well as healthier life practices, presenting acceptable analytical parameters and being assessed in periodically outpatient endocrinology consultations with good adherence. The patient refers and shows satisfaction with the medical procedure carried out, as well as the quality of life that he now presents.
Conclusion
We want to conclude by emphasizing the relevance of how a classic sign such as lipemia retinalis can contribute to the adequacy in the diagnosis of hyperchylomicronemia / hypertriglyceridemia, and therefore to the limitation of the severity of its complications. Frequently, simple anamnesis and basic physical examination can accelerate the times in the accurate diagnosis of this clinical process and, therefore, improve its prognosis by reducing the error rate and the severity of its complications 12.

