











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Remark
| 1) Why was this study conducted? |
| This manuscript aims to present the surgical approach to abdominal vascular trauma following damage control principles. |
| 2) What were the most relevant results of the study? |
| The priority in a trauma laparotomy is bleeding control. Hemorrhages of intraperitoneal origin are controlled by applying pressure, clamping, packing, and retroperitoneal with selective pressure. After the temporary bleeding control is achieved, the compromised vascular structure must be identified, according to the location of the hematomas. The management of all lesions should be oriented towards the expeditious conclusion of the laparotomy, focusing efforts on the bleeding control and contamination, with the postponement of the definitive management. |
| 3) What do these results contribute? |
| Abdominal vascular trauma is a challenge for the trauma care team. During the surgical procedure, immediate bleeding control must be achieved and maintained throughout the procedure. The specific approach to the injured vessel and treatment should be carried out according to the physiological status. |
Introduction
Abdominal vascular trauma occurs in a small proportion of patients admitted to trauma centers. However, a third or a quarter of the patients who require a laparotomy will have a vascular injury. Unfortunately, preoperative identification is impossible in most cases. Therefore, surgeons must be prepared for its early intraoperative recognition to allow appropriate management. This includes temporary bleeding control techniques, identification of the probably injured vessel and the specific approach and management.
Often, recognition of exsanguinating intra-abdominal hemorrhage will lead to immediate surgical indication, with activation of damage control protocols and consideration of early aortic occlusion.
This paper illustrates the applications of damage control in the management of patients with abdominal vascular trauma. This article is a consensus that synthesizes the experience acquired during the last 30 years in the management of trauma, general surgery and critical care of the Trauma and Emergency Surgery (CTE) group of Cali, Colombia, made up of experts from Hospital Universitario del Valle "Evaristo García" and the Hospital Universitario Fundación Valle del Lili, with the Universidad del Valle and the Universidad Icesi, in collaboration with the Colombian Association of Surgery and the Panamerican Trauma Society, in conjunction with international specialists from the US, Europe, Japan, South Africa and Latin America.
Epidemiology
Branco et al. (1, analyzed 7,191,025 patients registered in the United States national trauma database (NTDB) between 2002 and 2014 and identified 165,393 (2.7%) with vascular trauma. Of these, 5287 (3.2%) had an inferior vena cava injury, and 4157 (2.5%) had an abdominal aortic injury. The proportion of patients with abdominal vascular injuries compared to all vascular injuries has increased over the years and appears higher in the civilian series compared to the military series. For example, de Debakey et al 2) and Rich et al. 3, reported 1.9% and 2.9% in World War II and Vietnam, respectively. Patel reported 11.6% in Afghanistan 4. Mattox, meanwhile, reported 33.8% in Houston 5 and Morales 21% in Medellín 6.
The finding of vascular injuries in laparotomy is common in patients with penetrating trauma compared to blunt trauma. Nicholas and colleagues reported the experience with laparotomy for gunshot wounds at the Grady Memorial Hospital in Atlanta and compared them with the one published in previous years by the Ben Taub General Hospital in Houston 7. Abdominal vascular lesions were present in 30% and 25% of the patients operated on in each hospital. In two series of abdominal trauma caused by firearms at the Hospital Universitario del Valle, abdominal vascular injuries were found in 12% of 381 patients 8,9.
In the grouped series analysis of selected civilian trauma, 4,890 injuries were identified in 3,599 patients 5,10-17).. When the group of patients requiring surgical management was considered, systemic venous lesions accounted for 48% of all lesions, portal system lesions 11%, and arterial lesions 41% (Table 1).
Table 1 Abdominal vascular trauma. Percentage of injured vessels in selected civilian series
| Author | Kashuk13 | Adkins10 | Mattox5 | Khoury14 | García24 | Asensio11 | Tyburski16 | Paul15 | Weale17 | Total n (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| City | Denver | Nashville | Houston | Beirut | Cali | L. A. | Detroit | Milwaukee | Pietermaritzburg | |
| Year | 1982 | 1985 | 1989 | 1996 | 1997 | 2000 | 2001 | 2010 | 2018 | |
| Patients, n | 123 | 93 | 1947 | 107 | 205 | 302 | 470 | 242 | 110 | 3,599 |
| Penetrating trauma (%) | 108 (88) | 75 (81) | 1,719 (88) | 101 (94) | 198 (97) | 266 (88) | 419 (89) | 167 (69%) | 98 (89) | 3151 (88) |
| Arteries (%) | ||||||||||
| Aorta | 15 | 5 | 13 | 8 | 14 | 21 | 15 | 10 | 7 | 554 (14) |
| Iliac | 15 | 26 | 12 | 18 | 20 | 20 | 22 | 16 | 13 | 623 (16) |
| Renal | 7 | 11 | 8 | 0 | 4 | 5 | 6 | 7 | 19 | 285 (7) |
| Mesenteric | 5 | 3 | 11 | 0 | 2 | 9 | 5 | 9 | 15 | 336 (9) |
| Celiac trunk/branches | 5 | 8 | 0 | 0 | 2 | 10 | 7 | 14 | 9 | 139 (4) |
| Others | 0 | 3 | 1 | 0 | 0 | 13 | 3 | 2 | 10 | 98 (3) |
| Veins (%) | ||||||||||
| Cava | 41 | 31 | 27 | 47 | 34 | 29 | 31 | 23 | 15 | 1,128 (29) |
| Iliac | 17 | 31 | 15 | 53 | 23 | 17 | 25 | 15 | 19 | 770 (20) |
| Renal | 7 | 6 | 0 | 3 | 13 | 11 | 7 | 5 | 19 | 175 (4) |
| Hepatic | 0 | 6 | 3 | 3 | 2 | 0 | 6 | 5 | 1 | 117 (3) |
| Others | 0 | 0 | 3 | 3 | 0 | 8 | 4 | 17 | 3 | 144 (4) |
| Portal system (%) | ||||||||||
| Portal V. | 7 | 3 | 10 | 0 | 4 | 5 | 8 | 7 | 2 | 294 (8) |
| Splenic V. | 1 | 1 | 0 | 0 | 1 | 4 | 2 | 4 | 0 | 43 (1) |
| SMV | 8 | 8 | 0 | 0 | 7 | 11 | 7 | 9 | 4 | 142 (4) |
| IMV | 2 | 6 | 0 | 0 | 3 | 3 | 1 | 2 | 3 | 42 (1) |
L.A. Los Ángeles. SMV Superior Mesenteric Vein. IMV Inferior Mesenteric Vein
The venous structures most frequently injured were the vena cava in 29% of the cases, the iliac veins in 20% and the portal vein in 8%. Regarding the arterial vessels, the iliac arteries were compromised in 16% of the patients, the aorta in 14%, and the superior mesenteric in 9% (Table 1).
The proportion of patients with vascular lesions managed with laparotomy, who require damage control procedures, fluctuates between 24% and 82%, depending on whether it is a general series or if it refers to a specific vessel and the specific characteristics from the hospital where the report comes from 1,11,15,18,19,20-22. Branco et al. published the analysis of the cases of vena cava or aortic trauma cases registered in the American College of Surgeons' national trauma database between 2002 and 2014. Damage control laparotomy was reported in 28% of the 3,061 cases operated with trauma to the inferior vena cava and 24% of the 1,178 cases to the abdominal aorta 1.
Indications
Identifying patients who benefit from damage control is often expeditious. The indication is evident when the patient exhibits signs of exsanguination (profound hypotension that does not respond to resuscitation with fluids and blood components) or an agonizing state with indication for resuscitative thoracotomy 23.
Identifying cases in which the hemodynamic status on admission is stable or the patient responds to resuscitation requires a little more acuity. In a multivariate analysis performed at our center, gunshot wounds, shock index, and altered Glasgow coma scale were identified as preoperative variables associated with a greater probability of requiring a damage control laparotomy (DCL). 24. On the other hand, to identify intraoperative predictors, metabolic acidosis with a base deficit ≥8, hypothermia with a temperature <35° C, hemoperitoneum of >1.5 L and a NISS >35 were found as variables associated with the requirement of damage control resuscitation 25. Injury of specific anatomical structures such as the suprarenal abdominal aorta, the retrohepatic vena cava, the portal vein and the injury of two or more vessels are more likely associated with the need for a DCL 21. Intraoperative persistent hypothermia, persistent need for vasopressors, or clinical coagulopathy are also indications for DCL 23 (Table 2).
Table 2 Indications for damage control laparotomy
| Indication | Value |
|---|---|
| Physiological Parameter | |
| Glasgow | <14 |
| Temperature | <35o C at the beginning of surgery |
| Arterial pH | <7.2 |
| Base Déficit | >8 mmol/L |
| Lactate | >5 mmol/L |
| Clinical pattern - Surgical finding | |
| Procedures | Requirement of resuscitative thoracotomy |
| Hemoperitoneum | >1.5 L |
| NISS | >35 |
| Vascular Injury | Retrohepatic Cava Lesion |
| Suprarrenal Abdominal aortic injury | |
| Portal vein injury | |
| Injury of two or more vessel | |
| Clinical Coagulopathy | INR >1.5 |
Initial approach and diagnosis
The initial approach is carried out in an organized and prioritized manner, following the ATLS principles. Identifying the need for a laparotomy is easier in cases of penetrating trauma, in which the presence of shock or an acute abdomen allows the identification of most surgical candidates. Patients with injury to multiple body segments present some difficulty when deciding the surgical approach. In these, ultrasound will allow the abdomen to be identified as the main source of bleeding.
In blunt trauma cases, the systematic search for occult bleeding sites, supported by imaging methods, will provide the opportunity to identify the abdomen as the cause of the bleeding and, in most cases, the surgical indication. The surgical indication in more than two-thirds of cases is hemorrhagic shock 11,12,16. Signs suggest intra-abdominal vascular structure involvement as the cause of shock occurs in less than 5% of patients 12.
Patients with surgical indication should continue resuscitation in the operating room to avoid unnecessary blood loss and delayed bleeding control resulting from attempts to achieve hemodynamic stability preoperatively 26. Laparotomy and expedited bleeding control are part of the resuscitation in these cases.
Subjects in an agonizing condition should undergo resuscitative thoracotomy. Refractory hypotension should consider performing an aortic occlusion, which can be done simultaneously with the initiation of a laparotomy through the insertion of a REBOA, or with instrumental clamping of the abdominal aorta 27. Recognition of the risk of massive bleeding and activation of the massive transfusion protocol is essential.
If the patient is hemodynamically stable, an abdominal computed tomography (CT) with arterial and venous phases should be performed to determine the extent of vascular lesions in the abdomen and any associated lesions it may have 28. The lesions identified in this group of patients are more likely to be susceptible to endovascular treatment or nonoperative management.
Surgical management (Figure 1)
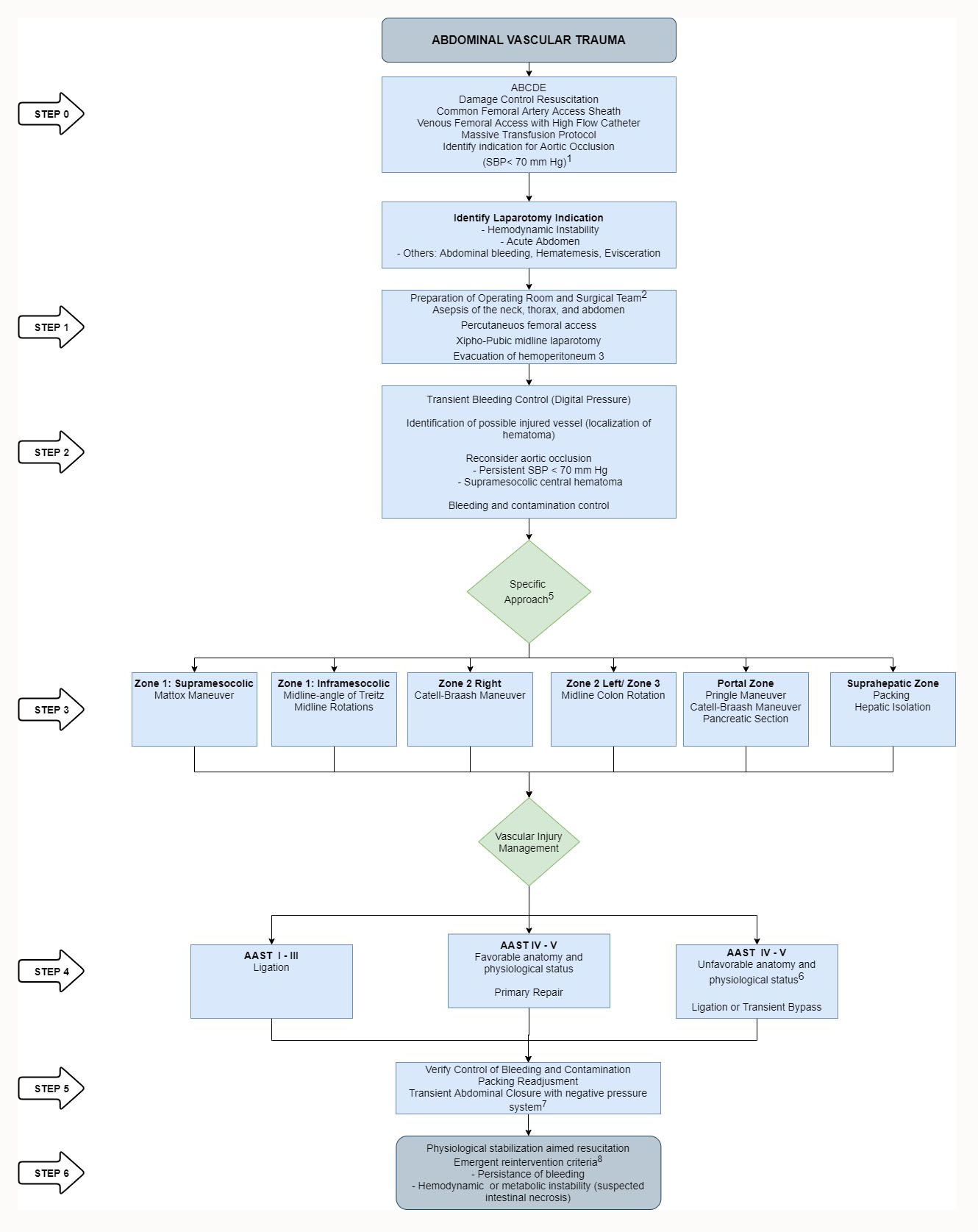
Figure 1 Surgical management of abdominal vascular trauma. 1. During the preoperative period the occlusion can be done using a Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA). 2. Element for prevention and management of hypothermia, rapid infusion, blood recovery, and autotransfusion, vascular access, procedures in different cavities and monitoring are included. 3. Consider autotransfusion. 4. Due to persistent hypotension or the need for proximal vascular control in arterial lesions. 5. According to the location of the hematoma, the site of bleeding, the trajectory of the wound and other injured organs. 6. List of vessels that can be ligated are in the Table 5. 7. Closure of the fascia or skin increases the risk of abdominal hypertension. 8. Non-emergent reoperation should be done as soon as hypothermia, coagulopathy, and perfusion are adjusted in patients with transient shunts or vascular ligation.
Step 0
Profound hypotension, defined as a systolic blood pressure <70 mm Hg, identifies the patient who benefits from therapeutic aortic occlusion 29. If the management group has implemented the use of the REBOA, it can be inserted by a parallel team while the main surgeon prepares and performs the laparotomy and control of the bleeding. However, delaying the bleeding control procedure due to insertion of the intravascular device may be associated with an increased likelihood of death 30.
Performing a thoracotomy before a laparotomy 31, for clamping the descending aorta was not associated with better outcomes and, on the contrary, causes additional trauma and creates an additional source of bleeding, so its routine use is not recommended 12,16.
Abdominal aortic occlusion in the diaphragmatic hiatus immediately after entering to the abdomen is preferable.
Step 1
When preparing for the management of severely traumatized patients, the hospital must have an available operating room that allows temperature regulation, has the elements for hemodynamic monitoring, the prevention and management of hypothermia, rapid infusion of warm fluids and blood components, as well as the surgical instrumentation required to access the different cavities, the management of vascular structures and the insertion of intravascular devices. In addition, prompt access to laboratory tests is essential to assess metabolic status and coagulation. Ideally, a cell salver device should be available.
In all cases, the patient is placed in the supine position and is prepared from the edge of the jaws and from side to side of the table. The abdomen is accessed through a xipho-pubic midline laparotomy. The cavity is quickly evacuated with the help of aspiration and laparotomy pads. The recovered blood can be transferred to the cell saver device. The presence of hollow viscera injury does not contraindicate the use of recovered blood for autotransfusion 32,33.
Loose pad placement in all four quadrants allows rapid identification of the bleeding source.
Step 2: Transitory control of bleeding
The priority in a trauma laparotomy is bleeding control. It should be considered that a vascular injury is not the only cause of exsanguinating abdominal bleeding, nor is it the most common. In a series of 60 patients with abdominal trauma from firearms and systolic pressure <70 mm Hg, major vascular injuries were the third leading cause of bleeding (20%), after liver (47%), and renal injuries (21%) 34.
Intraperitoneal hemorrhage is controlled by applying pressure, clamping, or packing. Retroperitoneal bleeding is temporarily controlled by applying pressure, which should be as selective as possible to allow exposure and management of the lesion (Figure 2). In addition to providing transient hemodynamic support, Aortic occlusion contributes to the reduction of distal bleeding to the site of occlusion (Figure 3).
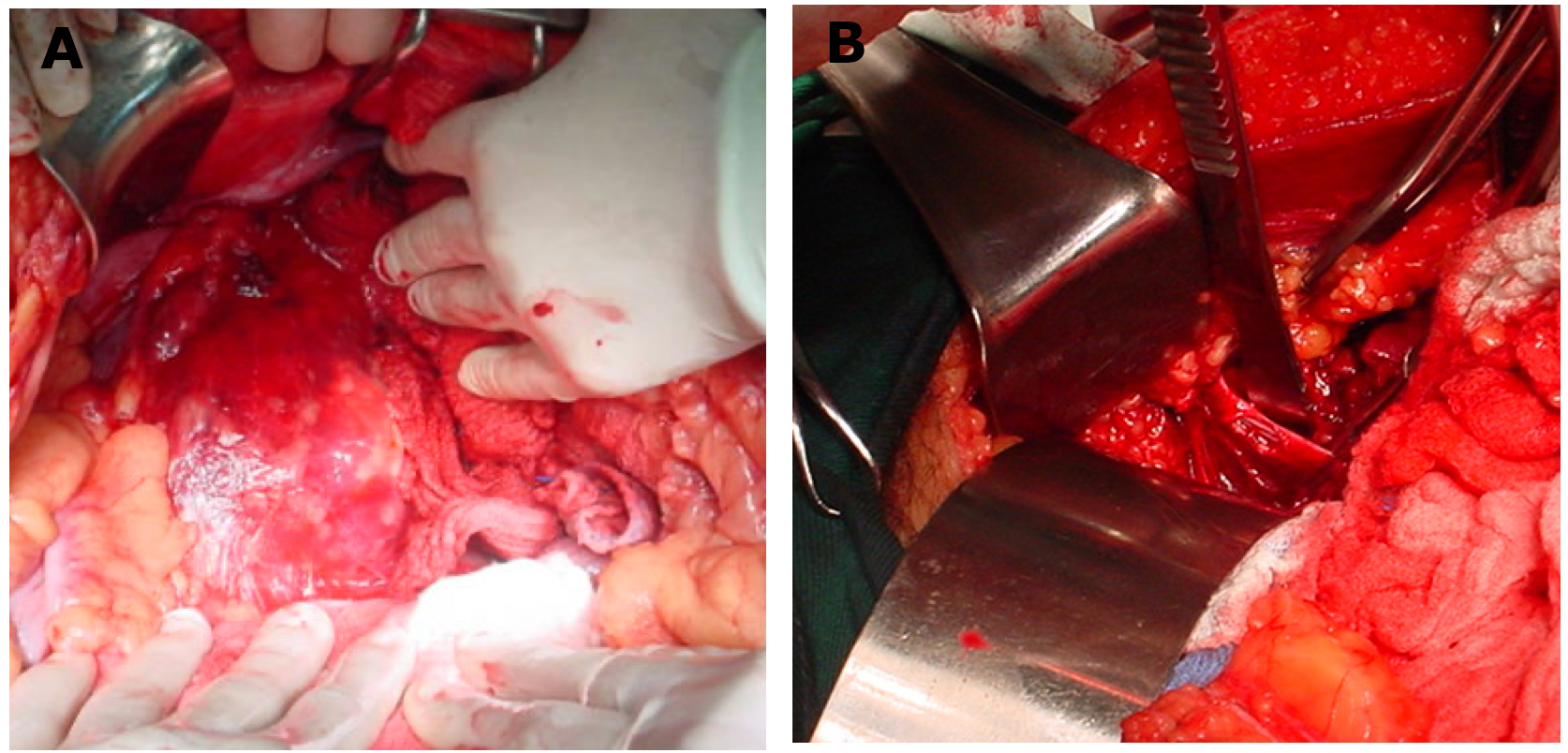
Figure 2 Penetrating trauma to the right iliac artery. A) Transient bleeding control with local pressure. B) Definitive vascular control with atraumatic clamps
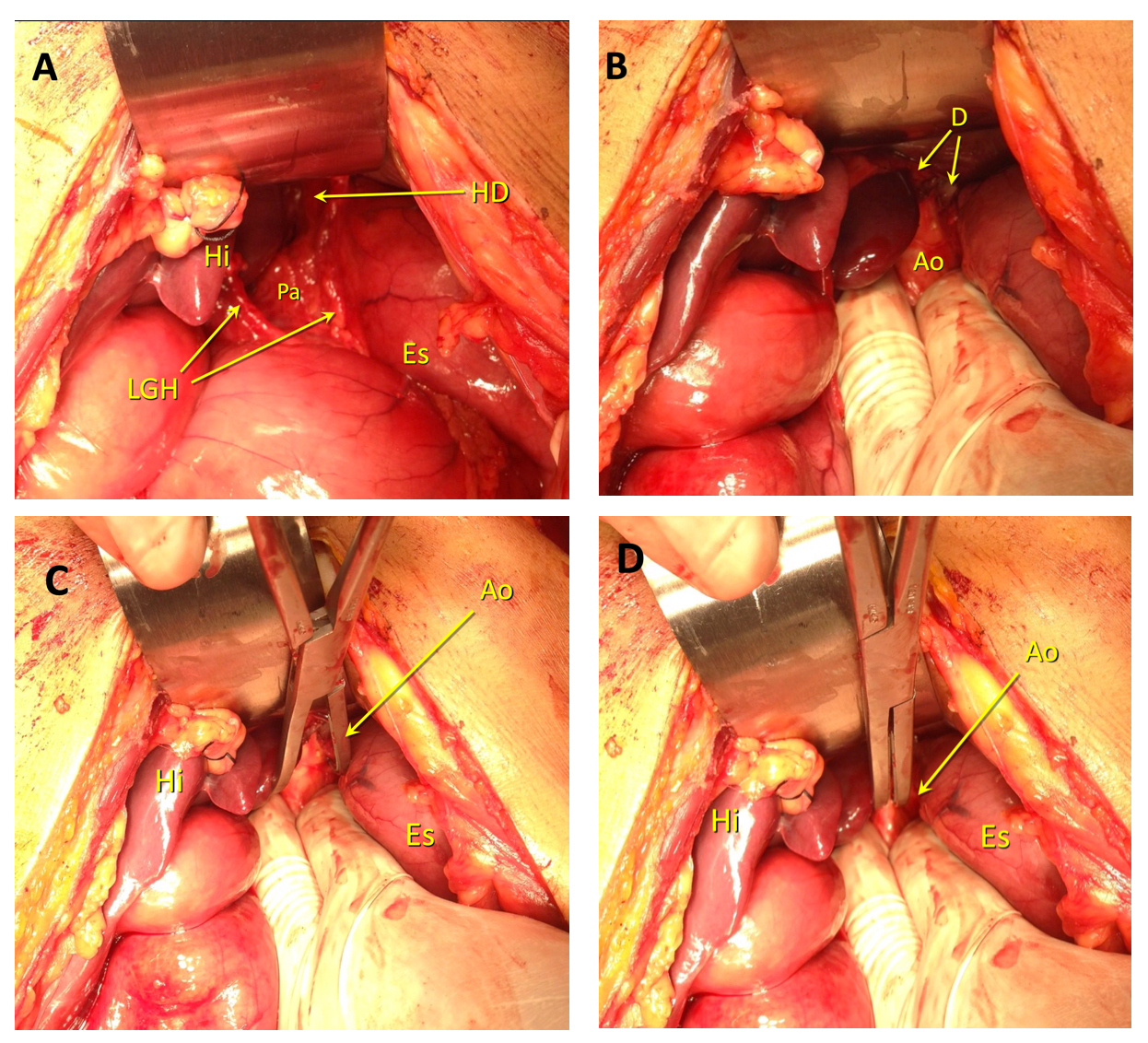
Figure 3 Clamping of the supraceliac aorta. A) Entering the lesser sac. The left hepatic lobe has been pushed back, the gastrohepatic ligament (Ghl) has been divided with a blunt maneuver with the index finger. The body of the pancreas (Pa) and the fibers of the diaphragmatic hiatus (DC) are observed. Li Liver. St stomach B) Guided by the pulsations of the aorta, the surgeon longitudinally dissects the fibers of the diaphragm at the hiatus (D). He surrounds the vessel on each side and clamps it between his index and middle fingers. Occasionally, some diaphragm fibers must be separated with an electrosurgical device. It is not recommended to completely surround the aorta during this maneuver. Ao Supraceliac Aorta. C) Aortic clamp placement. The surgeon keeps his fingers embracing the aorta. He advances the aortic clamp until he feels the resistance of the prevertebral fascia. D) Without removing the fingers, the clamp is closed, and the complete occlusion of the vessel is verified. HD. Hiatus day.
Step 3: Exposure of the injured vessel
After temporary bleeding control is achieved, the surgeon proceeds to identify the compromised vascular structure. This determines the specific approach to the definitive management. The location of the hematoma or site of active bleeding and involvement of other organs suggests the possible damaged structure 35. In penetrating trauma, the topographic location of the wound provides an additional hint.
The graph illustrates the location of the hematomas (Figure 4) and Table 3 lists the potentially injured structures in each location and their approaches.
Table 3 Classification of retroperitoneal hematomas, probable associated vascular structures, and recommended approaches.
| Location of the hematoma | Injured structure | Approach |
|---|---|---|
| 1A. Central supra-mesocolic | Suprarenal abdominal aorta | Medial mobilization of the viscera on the left side (Mattox maneuver) |
| Celiac trunk and branches | ||
| Superior mesenteric artery | ||
| Superior mesenteric vein | ||
| Proximal renal vessels | ||
| 1B. Central infra-mesocolic | Infrarenal aorta | Midline approach |
| Infrarenal cava | Mobilization of the viscera on the right side (Catell- Braash maneuver) | |
| Proximal iliac vessels | Mobilization of the left colon and the right colon | |
| 2A. Peri-renal, flank | Kidney | Cattell-Braasch maneuver |
| Distal renal vessels | Mobilization of the left colon and the right colon | |
| Supra-renal gland | ||
| 2B. Flank, pericolic | Infra-hepatic Cava | Cattell-Braasch maneuver |
| Juxta-renal Cava | Mobilization of the left colon and the right colon | |
| Infra-renal Cava | ||
| 3. Pelvic | Iliac vessels | Mobilization of the left colon and the right colon |
| 4. Portal | Portal Vein | Examination of the hepatic hilum |
| Common hepatic artery | Cattell-Braasch maneuver | |
| 5. Retro-hepatic | Retro-hepatic Vena Cava | Formal liver isolation |
| Hepatic veins | Intra-aortic (REBOA) and intracaval (REBOC) balloon catheters |
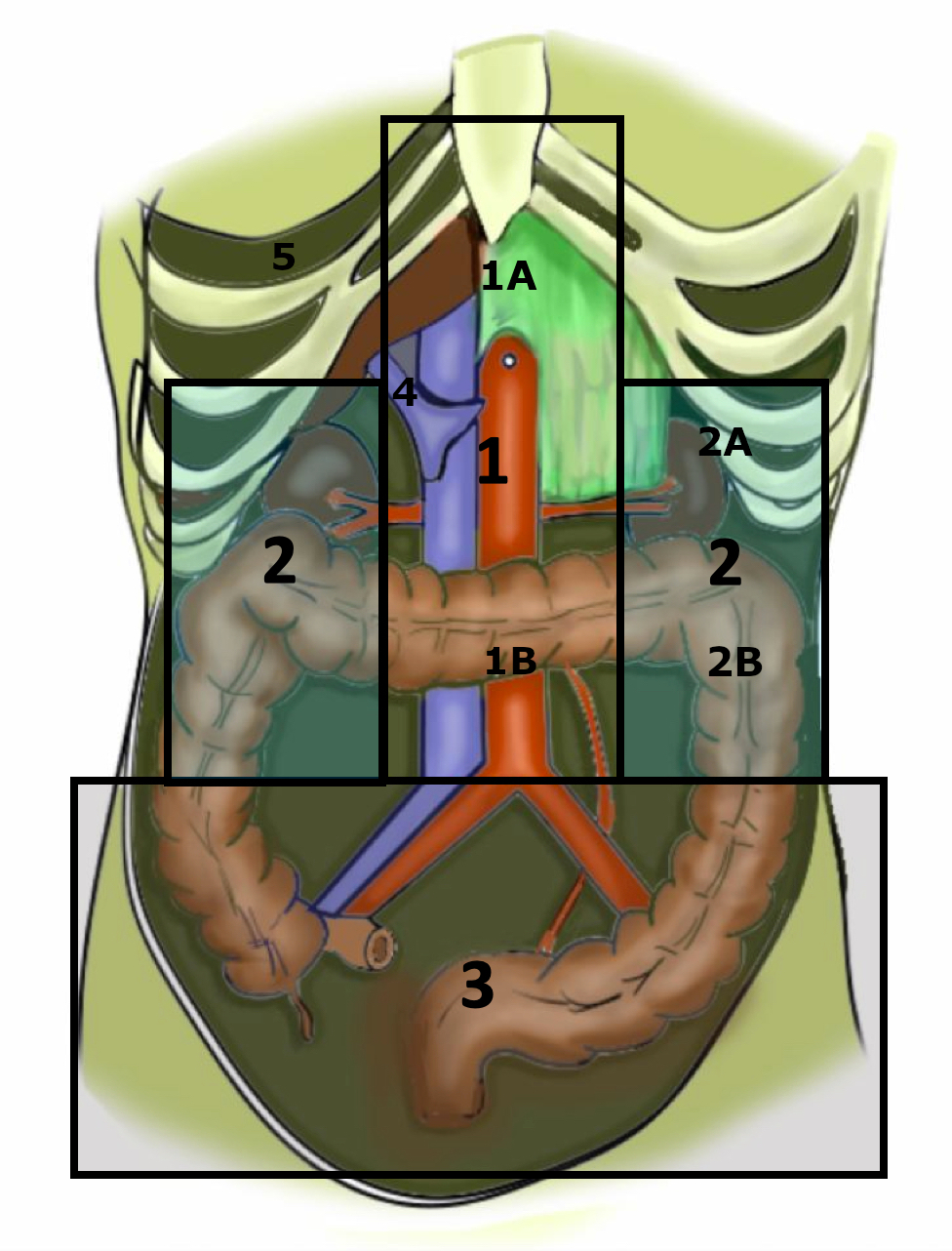
Figure 4 Location of retroperitoneal hematomas. 1. Central Medial 1A. Central supra-mesocolic.1 B. Central infra-mesocolic. 2. Flank. 2A. Peri-renal flank. 2B. Flank, pericolic. 3. Pelvic. 4. Portal. 5. Retro-hepatic
In relation to the classification popularized since the 1980s, some distinctions are added that are clear in the management of retroperitoneal vascular injuries in the context of penetrating trauma 35. Central hematomas are divided into supra and infra mesocolic due to the difficulties in exposure and the high lethality of the lesions of the suprarenal abdominal aorta and its visceral branches. Flank hematomas are differentiated into perirenal and pericolic, as stable perirenal hematomas should not be explored. Hematomas of the portal area and the retro-hepatic area are added, due to their particularities in terms of prognosis and surgical exposure. Table 3 relates the location of the hematomas, the vessels most frequently associated with each location, and the maneuvers suggested according to the suspected injury.
Asensio et al. 11, reported the presence of retroperitoneal hematomas in 91% of patients with abdominal vascular trauma managed at their institution. The location was central in 50% of the cases (supramesocolic 20%, infra mesocolic 30%), the flanks in 18% and pelvic in 32%. Additionally, 13% of patients had multiple zones of involvement.
The surgeon must select an approach that allows proximal and distal control to the injury, without compromising bleeding control, to perform the surgical repair after the proximal and distal occlusion (Figure 2) attempting to repair a vascular injury without achieving control results in unnecessary blood loss, which is unacceptable in a critically hypovolemic patient.
Step 4: Management of vascular injury
The prompt decision to perform damage control in patients who is indicated is of crucial importance. Prolonging surgery unnecessarily, attempting the definitive management of the lesions in an individual with depletion of its physiological reserve, is associated with a higher probability of death 36.
Frequent communication with the anesthesiologist will allow the surgeon to identify and follow the alterations that reveal the profound metabolic, hemodynamic, or coagulation alteration that forces the conversion towards a damage control procedure if the decision has not been taken previously.
The management of all lesions should be oriented towards the expeditious conclusion of the laparotomy, focusing efforts on the bleeding control and contamination, with the postponement of definitive management. Their management includes ligation, transient bypass, and packing of selected low-pressure vessels and bleeding surfaces regarding vascular injuries. In general terms, grade I to III injuries should be ligated, while IV and V injuries should be considered for repair (Table 4).
Table 4 Organic Injury Severity Scale (OIS) of the American Association for Trauma Surgery (AAST)
| Grade | Vessel |
|---|---|
| I | Innominate branches of superior mesenteric artery or superior mesenteric vein |
| Innominate branches of inferior mesenteric artery or inferior mesenteric vein | |
| Phrenic artery or vein | |
| Lumbar artery or vein | |
| Gonadal Artery or Vein | |
| Ovarian Artery or Vein | |
| Other small arterial vessels or innominate venous structures that require ligation | |
| II | Common hepatic artery, right or left |
| Splenic artery or vein | |
| Right or left gastric arteries | |
| Gastroduodenal Artery | |
| Trunk of the Inferior Mesenteric Artery or Superior Mesenteric Vein | |
| Named primary branches of the mesenteric artery (for example, ileocolic artery) or mesenteric vein | |
| Other abdominal vessels requiring ligation or repair | |
| III | Trunk of the superior mesenteric vein |
| Renal Artery or Vein | |
| Iliac Artery or Vein | |
| Hypogastric artery or vein | |
| Infrarenal Vena Cava | |
| IV | Trunk of the Superior Mesenteric Artery |
| Celiac trunk | |
| Vena Cava, suprarenal and infrahepatic | |
| Infrarenal Aorta | |
| V | Portal Vein |
| Extra Parenchymal Hepatic Vein | |
| Vena Cava, retrohepatic or suprahepatic | |
| Suprarenal aorta, subdiaphragmatic |
* Applies to extra parenchymal vessels. If the wound is located 2 cm proximal to the organ, the injury belongs to the organ. ** A point is added for Grade III and IV wounds if the injury involves more than 50% of the vessel. *** One point is subtracted for Grade IV and V wounds if the injury is less than 25% of the vessel circumference
The specific management of the most important vascular lesions is discussed below.
Aorta: Wounds to the suprarenal abdominal aorta and its visceral branches are usually presented by intra-abdominal exsanguination, with an operative finding of a central supramesocolic hematoma. Given this finding, proximal control should be carried out by performing a left medial visceral rotation (Mattox maneuver) 37,38 (Figure 5). Approaching the injury directly through the hematoma through the lesser sac or the transverse mesocolon is not very productive and is associated with prohibitive mortality. In some cases, when the hematoma is extremely voluminous or the patient is In Extremis, a left thoracotomy may be performed to clamp the aorta. Occasionally, proximal control may be performed with a REBOA deployed in zone I, which greatly facilitates exposure and reduces surgical trauma. In any case, it must be taken into consideration that occlusion of the supra-celiac aorta for more than 30 minutes causes severe ischemia and reperfusion, which is unlikely to survive. In these cases, the surgeon must consider partial or intermittent occlusion strategies and implement the most selective control in lesions of the visceral branches of the aorta. Exposure of the aorta to this level is completed by severing the fibers of the cross of the diaphragm and dissecting and ligating the lymphatic and nerve plexuses, which are very firm and surround it completely. Distal control is performed by dissection and clamping of the iliac vessels. After identifying the anatomical location of the wound, a more selective control and clamping is carried out. The repair to be made will depend on the clinical condition of the patient and the anatomical damage 38. Aortic injury caused by sharps weapons or low-velocity projectiles can be directly repaired by suturing. Other wounds will need to be repaired with a synthetic patch or graft (Figure 6A).
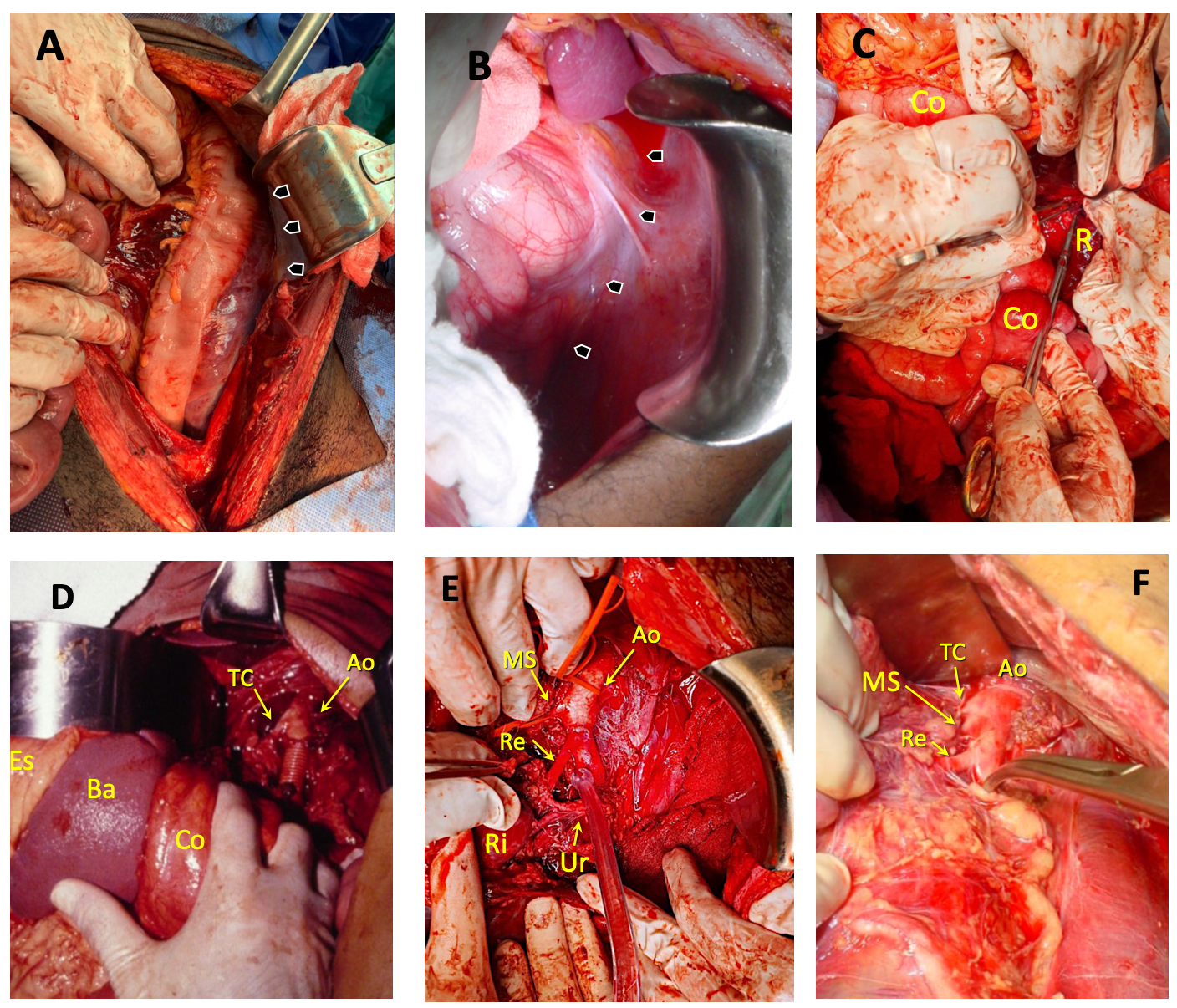
Figure 5 Mattox maneuver. A) Identification of the peritoneal reflection line of the descending colon, where the avascular plane that allows access to the retroperitoneum will be dissected. B) Identification of the peritoneal reflection line of the splenic flexure of the colon, spleen and stomach, to perform the medial rotation of these organs. C) By sharp and blunt dissection, the descending colon, the splenic flexure of the colon (Co), the spleen, and the stomach are mobilized medially. As it is advanced posteriorly in the retroperitoneum (R), the pancreas and kidney are mobilized. D) The lesion was located between the celiac trunk (CT) and the superior mesenteric artery. In addition to medial rotation of the viscera, the exposure required sectioning the fibers of the diaphragm and completely dissecting the firm plexus surrounding the aorta and the origin of its branches. Ao Aorta, St stomach, Spl spleen. E) Lesion located in the aorta (Ao) above the left renal artery (Re). SM superior mesenteric artery, K Kidney, Ur ureter. F) Exposure of the supraceliac and visceral aorta (Ao). A lesion of the celiac trunk (CT) has been managed with ligation. The remnants of the plexus surrounding the aorta can be seen. MS superior mesenteric artery, Re left renal artery.
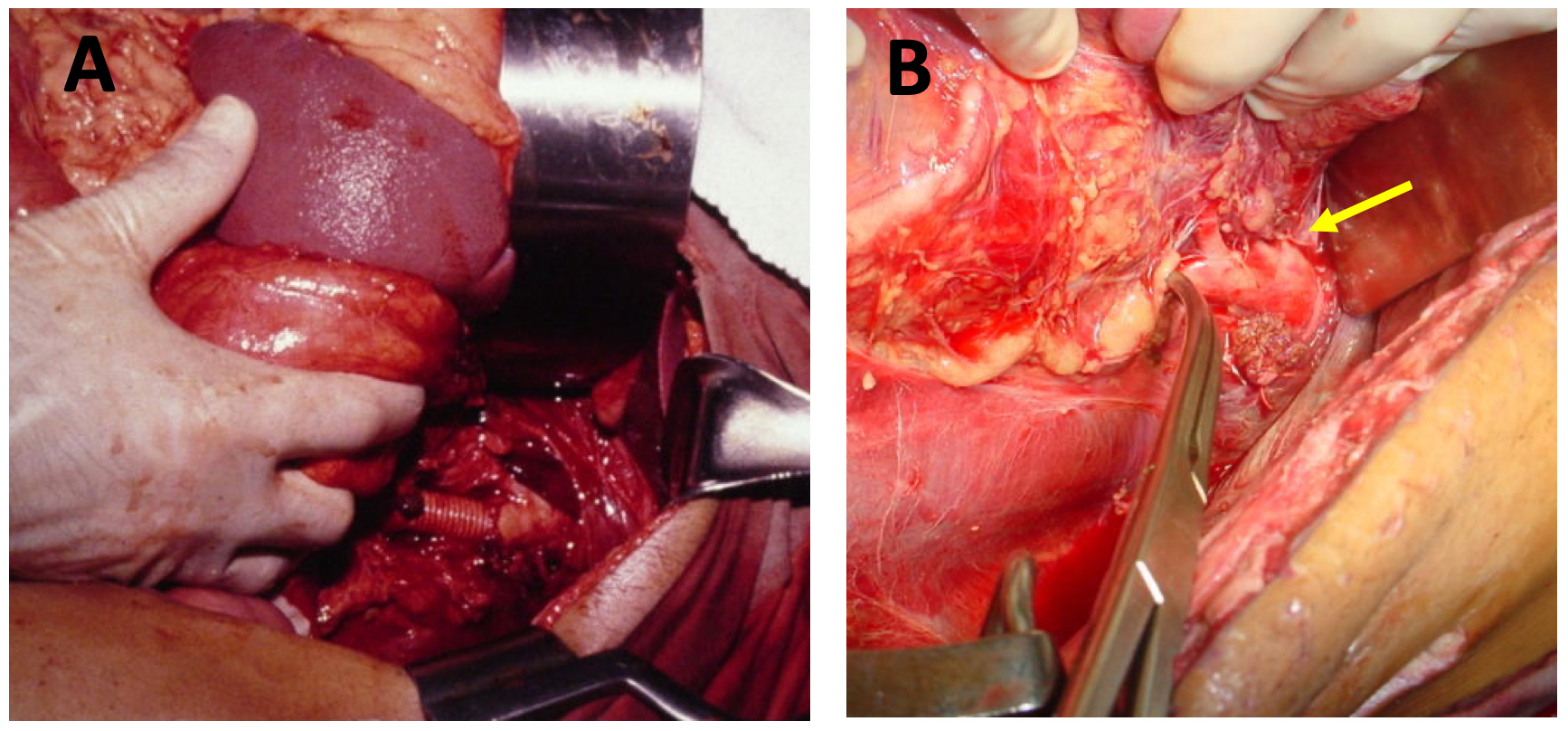
Figure 6 Injury to the suprarenal aorta and its branches. A) Injury between the inferior mesenteric artery and the renal artery. Note the medial rotation of the viscera on the left side. The injured segment has been replaced by a dacron graft. B) Celiac trunk injury. Note the medial rotation of the viscera on the left side. The injured vessel was handled with ligature (yellow arrow).
The coeliac trunk and its branches can be ligated with a low risk of ischemic complications (Figure 6B). In extreme situations, the superior mesenteric artery or vein can be ligated since the probability of survival depends more on the hemodynamic status of the patient than on the ligation or repair of the vessel (Table 5). Under extreme conditions, if circumstances permit, vascular continuity can be maintained with a transient bypass in the aorta or superior mesenteric artery 39.
Table 5 Vessels that can be ligated in the management of abdominal trauma
| Low risk of complications |
| Veins |
| Infra-renal cava |
| Iliacs |
| Left kidney |
| Inferior mesenteric |
| Splenic |
| Arteries |
| Celiac trunk |
| Liver |
| Inferior mesenteric |
| Internal Iliaca |
| In special circumstances |
| Portal Vein |
| Infra-hepatic vein cava |
| Superior mesenteric artery |
| Superior mesenteric vein |
Infrarenal aortic wounds present as a midline hematoma. Depending on the specific location of the lesion and the size of the hematoma, proximal control may be performed with a more limited mobilization of the viscera on the left side (Figure 7), through the midline or utilizing a Catell-Braasch maneuver. Repair of the injury follows the principles mentioned 40,41.
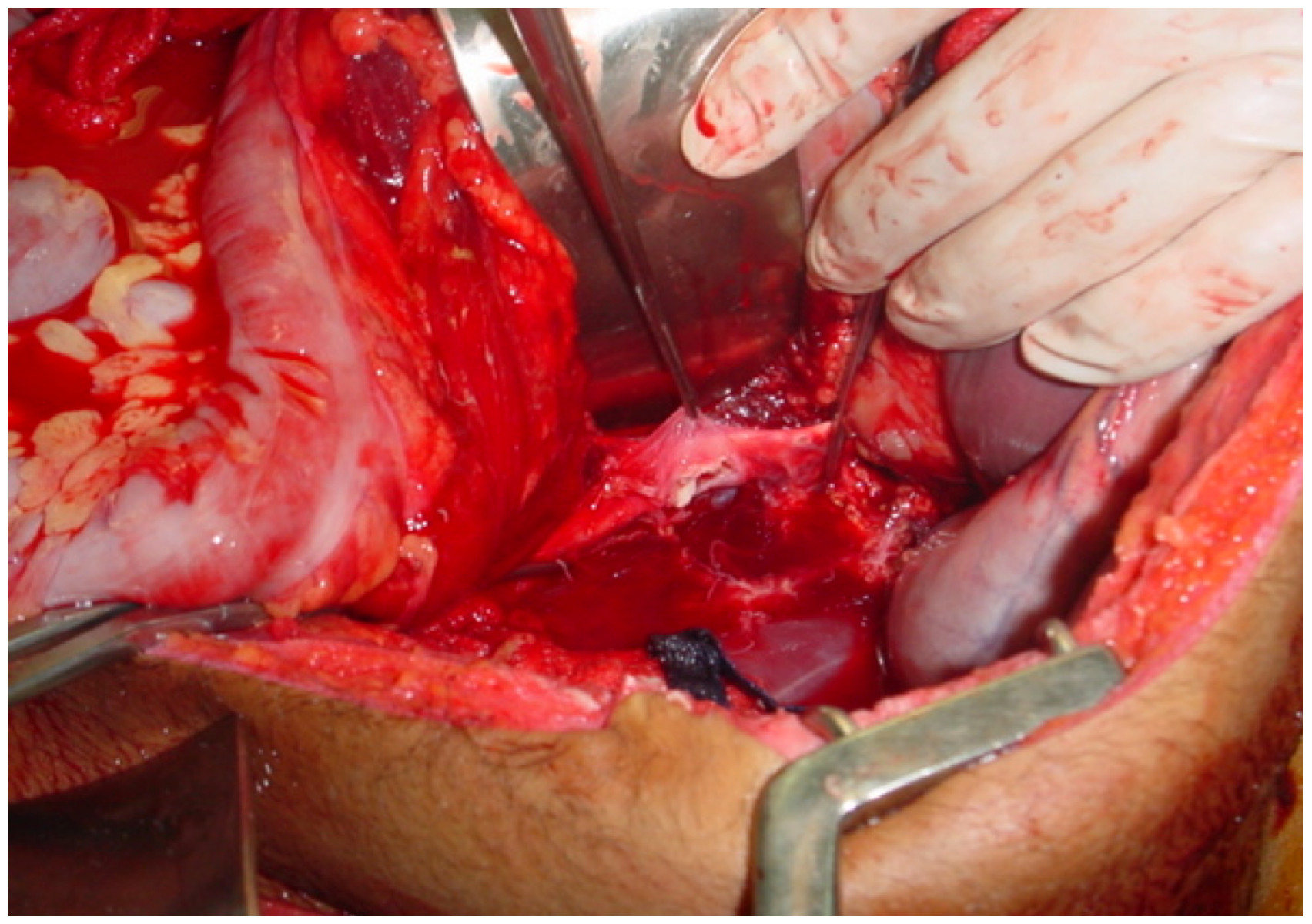
Figure 7 Exposure and control of an infrarenal aortic injury with medial mobilization of the left colon.
Inferior Vena Cava (IVC): Wounds to the infra-hepatic, juxta-renal, and infra-renal segments of the vena cava present as a central or right lateral hematoma or hemorrhage 42-44.
Proximal control of the vessel is performed with medial mobilization of the viscera on the right side (Catell-Braash maneuver) (Figure 8), while maintaining digital compression on the injury site, thereby achieving temporary hemorrhage control. The extent of exposure is determined by the location of the wound and the size of the hematoma. Proximal and distal controls can be accomplished with forceps, swabs or even with the assistant's own fingers. Juxtarenal injuries will often require dissection and occlusion of the renal veins. Lateral clamping with Satinsky forceps will allow repair of the lesion in selected cases.
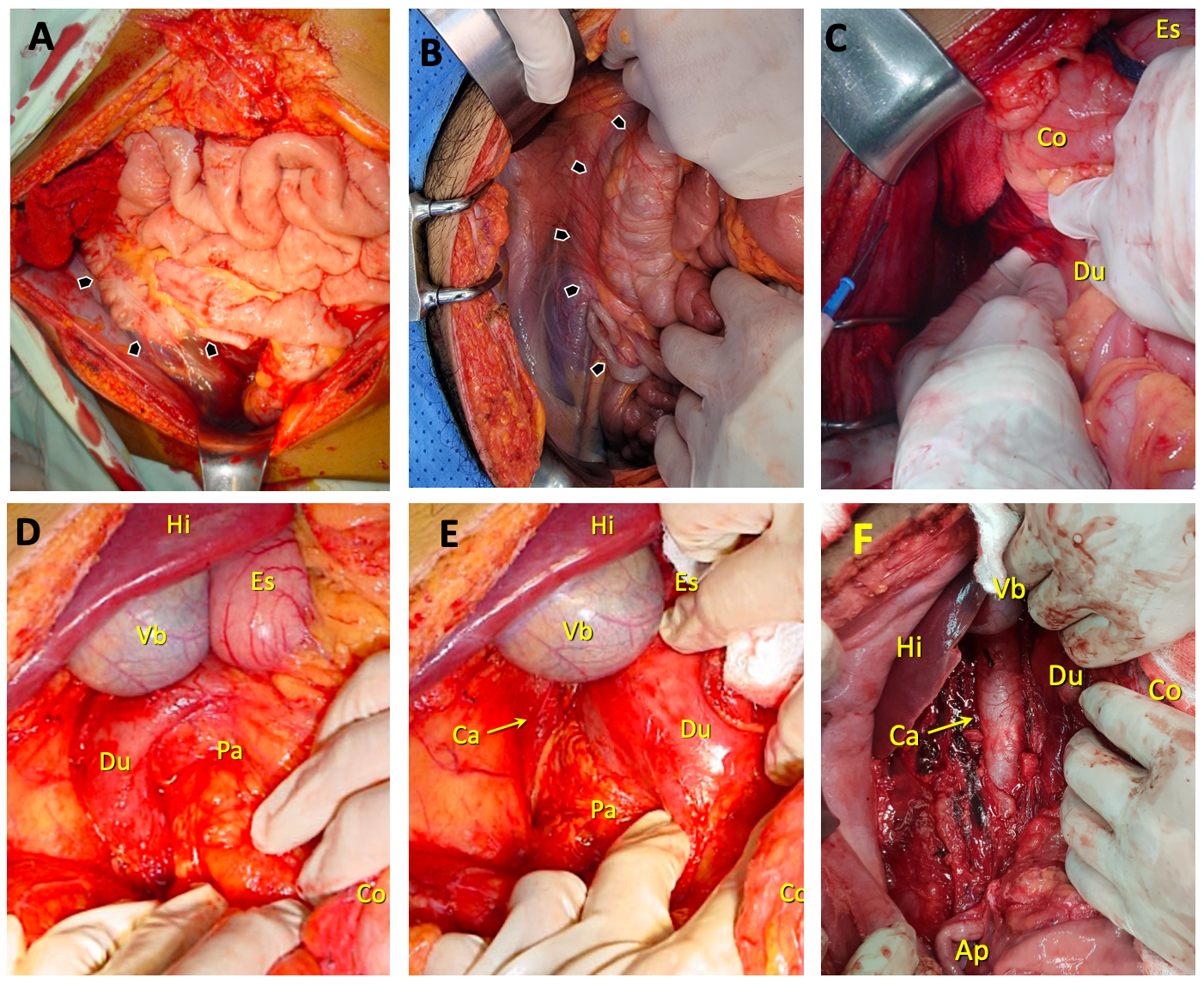
Figure 8 Catell Braasch maneuver. A) Hematoma in zones 2 and 3 on the right side. The arrows indicate the peritoneal reflection, where the incision would be made to access the retroperitoneum. The possibility of surrounding the cecum and directing the incision at the base of the mesentery is indicated, allowing the elevation of the right colon and the small intestine, to expose in addition to the vena cava, the right iliac vessels and the infra-renal aorta. B) Identification of the peritoneal reflection line of the ascending colon. C) The surgeon has mobilized the hepatic flexure of the colon (Co) and is entering the retroperitoneum posterior to the duodenum (Du). St Stomach D) Mobilization of the hepatic flexure of the colon (Co) and exposure of the first three duodenal portions (Du) and the head of the pancreas (Pa). Li liver, Gb gallbladder, St stomach. E) Mobilization of the duodenum (Du) and the head of the pancreas (Pa), to expose the suprarenal vein cava (Ca). Li liver, Gb gallbladder, St stomach. F) Mobilization of the right colon (Co) and duodenum (Du), to expose the entire vena cava (Ca). Li liver, Gb gallbladder, Ap caecal appendix.
The existence of a posterior (mirror) injury will force the surgeon to broaden the anterior wound to repair it from the inside or to carefully rotate the vessel to expose it from behind without injuring the lumbar tributaries. Medial rotation of the right kidney will expose the posterior side of the juxtarenal cava. Other treatment methods include reconstruction with a venous or peritoneal patch and, rarely, anastomosis or insertion of a graft. In the damage control setting, ligation can expeditiously resolve the injury 19 (Figure 9).
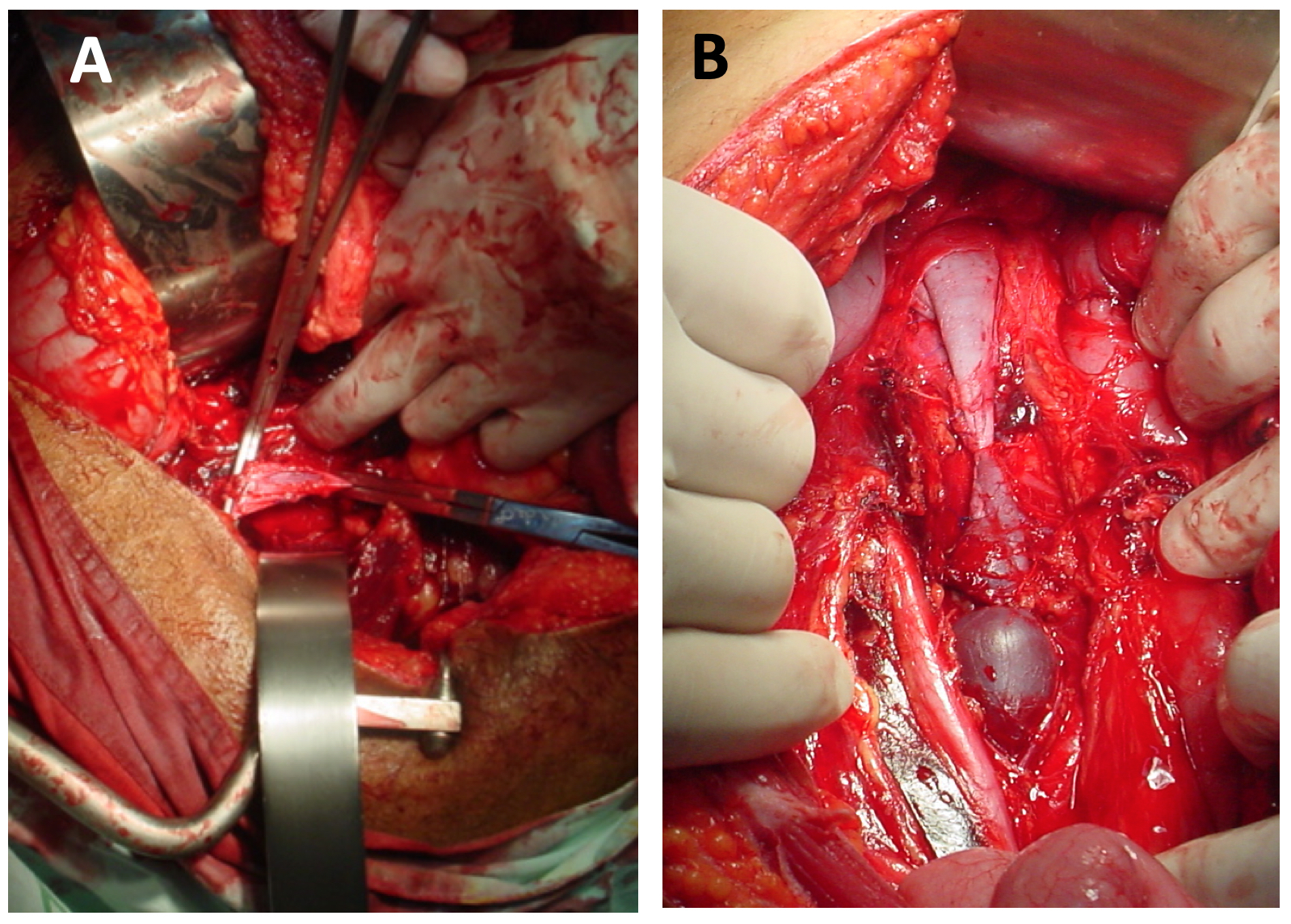
Figure 9 Trauma of the infrarenal vena cava. A) Exposure of the vein with medial mobilization of the right colon. B) Infrarenal vena cava ligation.
Its use has been reported in percentages as low as 5% and as high as 63%. For example, in an analysis of 1,316 patients with IVC injuries registered in the United States National Trauma Database (NTDB), ligation was reported in 34% of cases 45.
Matsumoto et al., compared 310 patients with injury to the IVC in which ligation was performed, with an equal number of repaired cases, matched for the probability of being ligated, identified in the NTBD. Patients treated with ligation had greater severity of trauma and greater physiological deterioration. After matching, they found mortality to be similar, with increased risk of extremities compartment syndrome, thromboembolic events, pneumonia, and longer ICU and hospital stay in those with ligation 45. Byerly et al., selected the isolated IVC trauma cases from the NTDB and compared 104 ligated patients with 339 repaired patients. The multivariate analysis found that ligation was not associated with a higher risk of death or amputation but with a higher probability of acute kidney injury, venous thrombosis, and fasciotomy 46. The usual recommendation in wounds of the infrahepatic segment is to avoid its ligation. There are isolated reports of survival after ligation 47,48. This is preferable to death due to prolonged repair attempts.
The decision to ligate the vessel, resembling the decision to perform damage control, should be made promptly. When taken as a last resort, loss of time and blood occur, with greater physiological derangement and a considerable increase in the risk of death.
Injury to the suprahepatic vessels or the retrohepatic vena cava presents as a severe hemorrhage in the suprahepatic location or as a hepatic wound with dark bleeding that persists despite clamping of the hilum 49. When a stable hematoma is present or bleeding is controlled with packing, the surgeon should avoid any effort to mobilize the liver to expose and repair the injured vessel 50. In a second stage, a surgical team that includes a hepatic surgeon returns to the operating room after the patient has been stabilized and the perfusion, hypothermia and coagulopathy alterations have been corrected. Occasionally the removal of the packing is performed in several sequential procedures, allowing the healing of the vascular lesion without a surgical repair (Figure 10). In these cases, imaging of the patient and endovascular treatment is also possible.
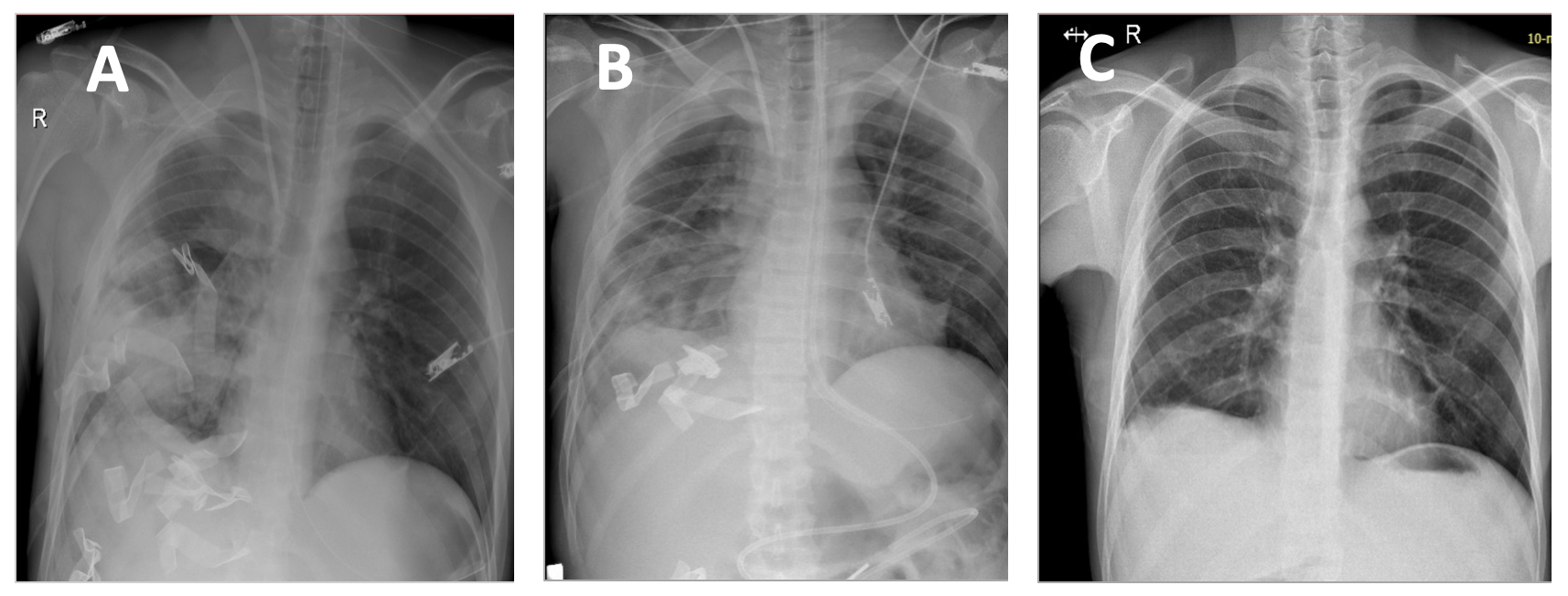
Figure 10 Patient with exsanguinating suprahepatic hemorrhage and injury to the right lower lobe. Wound in the suprahepatic area (segment IV) with hemorrhage that was not controlled with clamping of the hepatic hilum. Due to the need to resolve the intrathoracic bleeding, the surgeon packed the liver injury achieving control of the hemorrhage. A) Chest X-ray, Day 1. Laparotomy pads are observed on the chest and abdomen. B) Chest X-ray, Day 3, After chest unpacking and closure and partial abdominal unpacking. C) Chest X-ray, Day 10, after completing abdominal unpacking and closing the fascia.
If perihepatic packing is unsuccessful, one group member applies pressure to the injury to temporarily achieve bleeding control, while the rest of the team performs hepatic vascular exclusion as vascular control. This can be carried out by placing a REBOA in zone I and an intra-cava balloon (REBOC), inserted through the right femoral vein, taking it to the retrohepatic vena cava and make the total isolation by endovascular methods 51,52. If this resource is not available, liver isolation is performed with a Pringle maneuver, occlusion of the supra celiac aorta, occlusion of the infrahepatic inferior vena cava, and control of the inferior intrathoracic cava through a sternotomy or thoracotomy. Only under these conditions is possible to perform a repair with suture of the retrohepatic vena cava, or proximal and distal ligation of the vessel or a transfixing suture of a suprahepatic vein (Figure 11).
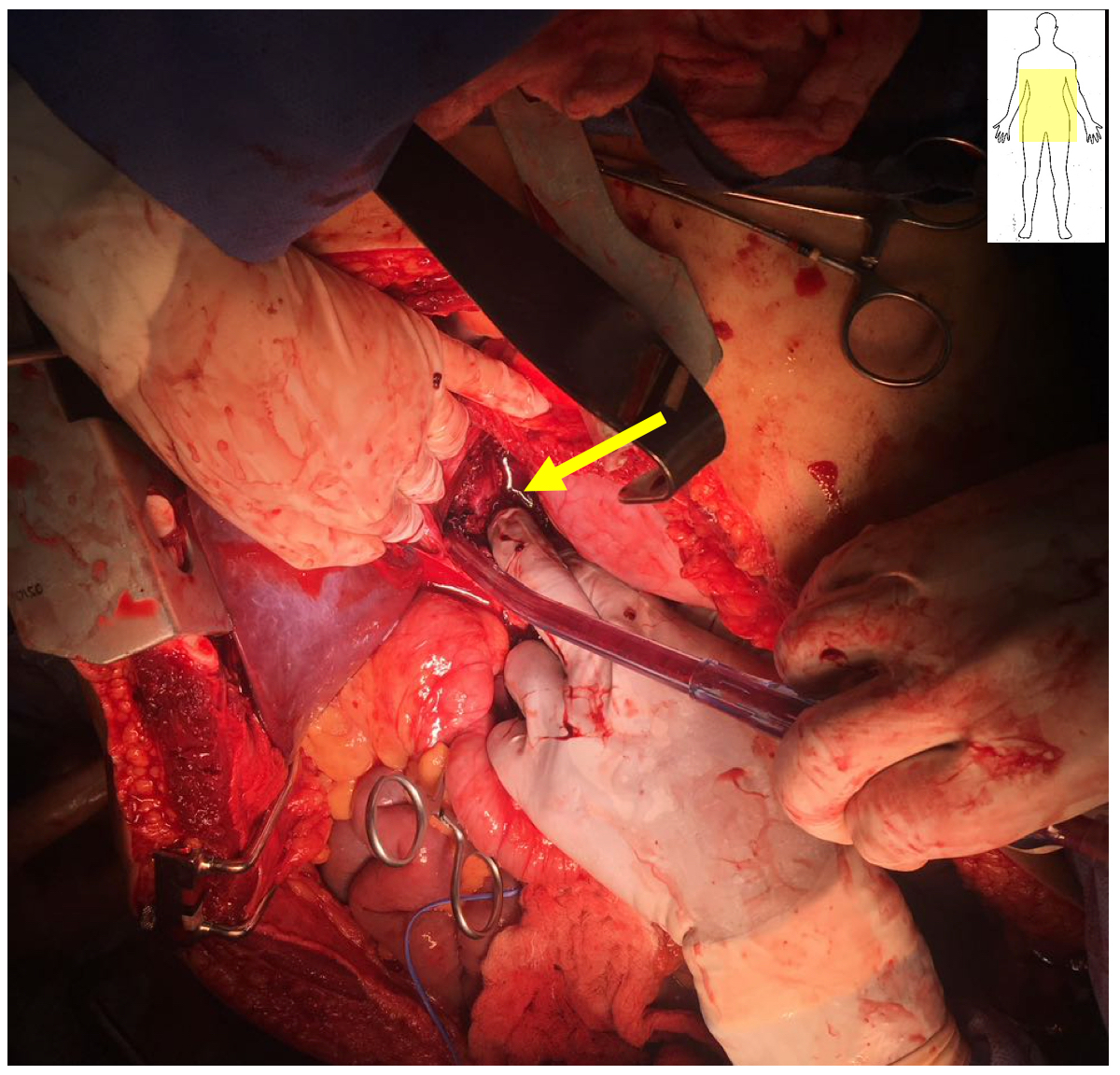
Figure 11 Wound on the medial area of the retrohepatic cava. Hepatic exclusion was performed by intravascular occlusion of the aorta in zone 1, of the vena cava in its retrohepatic portion, and clamping of the hepatic hilum. The left liver lobe has been mobilized to the right and the surgeon's finger controls the bleeding, in preparation for its suture (arrow)
The use of atrio-cava or cavo-atrial shunts is successful in the hands of some groups 53-55. However, its execution is time-consuming and, in the experience of most surgeons, mortality does not change. Therefore, the approach with hepatic exclusion as described is preferred 56. The use of a centrifugal pump to preserve the venous return of the lower half of the body while the injury is being repaired has been reported, but the availability of these devices is limited 57,58.
Iliac vessels: Iliac vessel trauma usually presents as a lateral pelvic hematoma. Less frequently as a flank hematoma. Proximal vascular control requires mobilization of the right or left colon, and occasionally distal repair requires dissection of the common femoral vessels in the thigh 59. Injuries to the internal iliac are almost always managed with ligation, whereas injuries to the common iliac and external iliac are preferred to preserve blood flow to the lower extremity, which in damage control situations, temporary shunts are usually used 39,60 (Figure 12).
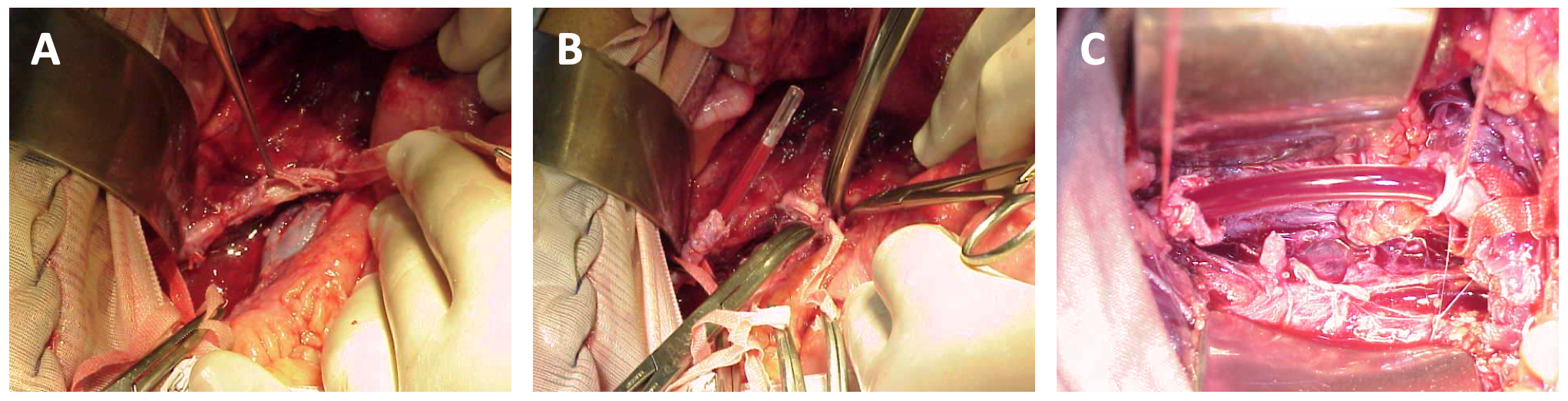
Figure 12 Placement of a temporary shunt in a lesion of the right iliac artery. A). Proximally and distally repaired artery. B) The graft (LeVin 16 Fr probe segment) has been installed sideways. C) The graft has been completely installed. Notice the firm ties that fix it. Courtesy Dr. Diego Rivera.
Porta Vein: Porta vein injuries may manifest as bleeding in the area of the hepatic hilum or as a hematoma in right zone II 35. In the first scenario, the clamping of the hepatic hilum achieves control of the hemorrhage. In the second, the Catell-Braasch maneuver with medial rotation of the duodenum and the head of the pancreas may be insufficient. Therefore, the section of the neck of the pancreas may be necessary. Lateral repair is reserved for small injuries in stable patients. However, ligation, when it is not left as a last resource, can be life-saving in unstable subjects. Stone et al. reported a reduction in mortality from 87% to 20% when they changed their decision to ligate the portal vein as the last choice procedure after failed attempts, to a first-line procedure in the group of unstable patients 61 and Pachter reported a low incidence of portal hypertension after vessel ligation for traumatic injuries 62. More recently, Sabat et al. (63, compared 103 patients with traumatic portal vein injuries managed with ligation with 304 individuals treated with a repair. The treatment method was not associated with higher mortality, while race, the severity of the trauma, presence of coma on admission, and coexistence of another vascular lesion were associated with a higher risk of death. Bowel complications and hospital stay were similar in both groups.
The principles of management of superior mesenteric vein injuries are similar to those described for the portal vein (Figure 13, Table 5).
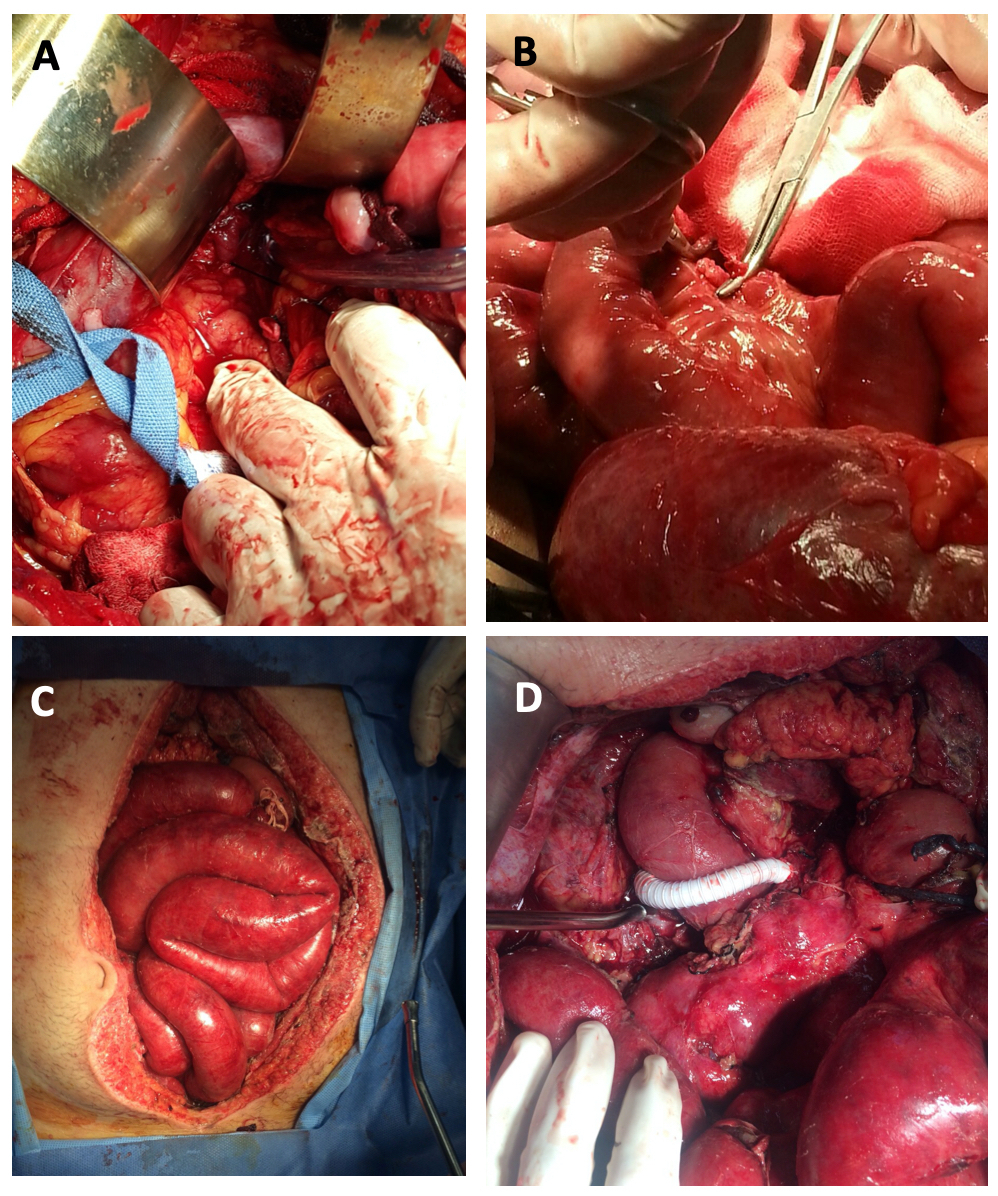
Figure 13 Blunt trauma with multiple intestinal and mesentery injuries. Severe instability requiring aortic clamping. A). Ligated distal end of the superior mesenteric vein. B) Proximal stump ligated. C) Day 5. Six reoperations were require due to progressive necrosis of the small intestine. Massively swollen and congestive intestine. D) A mesenteric-caval bypass was performed. After this the intestinal congestion resolved and the intestine could be anastomosed in subsequent procedures.
Step 5. Temporary cavity closure
After managing the vascular lesion and controlling the sources of contamination, the surgeon verifies the absence of active bleeding and readjusts the laparotomy pads. He then proceeds to perform the unconventional closure of the abdominal cavity.
Closure of the fascia or skin with sutures or towel clamps is not recommended as it increases the risk of abdominal hypertension and compartment syndrome 64. The suggested method is one that allows to increase the volume of the abdominal cavity and, if possible, that uses the principle of negative pressure because it simplifies nursing care, allows monitoring of persistent bleeding and potentially favors closure of the fascia 65,66.
There are doubts about exacerbation of bleeding with negative pressure systems. The authors' observations demonstrate that pressure is not transmitted beyond the site where the pads or foams are placed 67. In addition, the experience of those who handle a certain volume of trauma patients allows to safely suggest the use of negative pressure devices from the first procedure.
Step 6. Reoperations and vascular reconstruction
The group of patients with vascular injuries treated with damage control procedures often require emergency reoperations due to persistent bleeding or ischemic complications.
If this is not the case, patients should be reoperated as soon as hypothermia, coagulopathy and hemodynamic alterations have been restored to reconstruct the arterial vessel if a temporary bypass was used and to verify intestinal viability in the patients managed with ligation of the portal vein or superior mesenteric vessels.
Prognosis
The prognosis of patients with abdominal vascular trauma depends mainly on the injured structure. It is also affected by the number of vessels involved and by the presentation of the lesion as a contained hematoma or as an active hemorrhage 68. Different series show that the suprarenal abdominal aorta and the retrohepatic cava segments have the highest mortality, which exceeds 70% in most reports 11,38,40,42,43,69,70.
Vessel injury with an AAST 3 or 4 classification have intermediate mortality, whereas group 1 and 2 lesions have low mortality that depends on the involvement of other structures 5,11,17. Mortality increased in proportion to the number of injured vessels and compromised organs 11,15,16. Indicators of the severity of the physiological derangement caused by the hemorrhage and the higher transfusion requirement were also associated with a higher probability of death.
The type of repair performed was not associated in general terms with the probability of death. However, some procedures such as inferior vena cava ligation were more likely to have compartment syndrome of the extremities, venous thrombosis, pulmonary embolism, and pneumonia 46,45.
The early decision to perform damage control and the frequent use of techniques to abbreviate the surgical procedure were associated with a drastic reduction in mortality in patients with damage control for abdominal vascular trauma managed by the authors 36. In addition, early use of REBOA, placed by a parallel group to those performing the procedures to achieve bleeding control, was associated with a better chance of survival in critically ill patients with penetrating torso trauma 27.
Discussion
Mortality from abdominal vascular trauma has not changed in the last 40 years. Consideration of strategies such as damage control resuscitation, reduction of preoperative time intervals, resuscitation of the patient in the operating room, expeditious implementation of endovascular management techniques such as REBOA and REBOC, and the incorporation of hybrid therapies should allow for the survival of patients otherwise sentenced to death. The surgeon must be prepared to decide early damage control that results in a determinant of improved survival and reduced morbidity. The preparation of the team in charge of treating the patient, aimed at preventing complications such as hypothermia and coagulopathy, intraoperative monitoring, not only of the hemodynamic variables but also of the metabolic and coagulation status, will also contribute to improving the results. The intraoperative performance of the surgeon should include the automation of the recognition of the abdominal vascular injury and the implementation of the sequence that should include the transitory bleeding control, the specific approach according to the suspected injury and the appropriate repair regarding the physiological status will also contribute to optimizing the result.
Without wasting time on non-essential maneuvers, an exit from the abdominal cavity is also part of optimal surgical care. Postoperative management aimed at restoring the patient's physiological variables and detecting complications to receive immediate treatment is the essential complement to a well-performed surgical treatment.
Conclusion
Abdominal vascular trauma challenges and tests the trauma care team. During the surgical procedure, immediate bleeding control must be achieved and maintained throughout the procedure. In addition, the specific approach to the injured vessel and treatment should be carried out according to the physiological status.

