











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Remark
| 1) Why was this study conducted? |
| This study was conducted to evaluate the quality of English and Turkish YouTube videos about chronic prostatitis and to investigate whether they can be used as a reliable source of information. |
| 2) What were the most relevant results of the study? |
| We found that while videos of health professionals were more reliable and had higher quality, videos of non-professional in health had better ratings, similar to findings in the literature. |
| 3) What do these results contribute? |
| Health associations should pay more attention to medico-legal considerations and organize training programs on creating compelling social media content with greater reliability and quality, which is likely to be viewed and rated more often. With more reliable, higher-quality videos that fit YouTube's algorithm, spreading misinformation and fake news on this topic could be easily blocked. |
Introduction
The increased use of smartphones worldwide has made the Internet an indispensable tool in people's lives. The Internet is the first choice for seeking information, especially about health topics, as it is easy to use and free access to wi-fi networks is widely available. Social media platforms like YouTube, Facebook, and Instagram, called Web 2.0, help people to learn if they have a disease and, if yes, what the prognosis is and what the treatment options are. Further, they can easily learn other patients' testimonials. One of the most searched health topics in urology has been andrological problems. It was found that the most viewed YouTube videos were about premature ejaculation and erectile dysfunction 1. Men's andrological problems cannot be discussed easily with friends, families, or doctors of the individuals because many of these problems are identified as embarrassing issues. Because of this stigma, men usually turn to YouTube videos instead of health professionals.
Two recent reviews discussed the YouTube videos about andrological problems 2,3. The topics included were male infertility, Peyronie's disease, premature ejaculation, erectile dysfunction, prostate cancer, benign prostate hyperplasia, delayed ejaculation, and male hypogonadism. Chronic Prostatitis, as a subtype of chronic pelvic pain syndrome, was not included because there has not previously been a discussion on the YouTube videos about chronic prostatitis in the literature. As a result, in this study, we wanted to research the characteristics, content quality, and reliability of YouTube videos on chronic prostatitis.
Material and Methods
This cross-sectional study did not require institutional ethical committee approval because it examined YouTube videos that were free for use on the Internet. No human participants or animals were included in this study.
A video search of the YouTube online library (https://www.youtube.com) was performed on 15/10/2023 using the keywords' kronik prostatit' and then 'chronic prostatitis' for Turkish and English videos, respectively. The search was performed using the YouTube default settings (i.e., YouTube default option that uses a complex algorithm based on factors such as view count, upload date, rating, comments, bookmarks, and user age) after the cookies had been deleted from the computer's operating system. The results were then listed according to relevance.
The first 100 Turkish and English videos ranked by relevance were viewed for information on chronic prostatitis. We limited our review to the first 100 videos because 95% of users only watch the first 60 videos found by reports 4-6. After the search results were recorded in a playlist, the 200 videos were reviewed within one week by two independent urologists. Each reviewer accessed the video list by clicking on the library link address that had been shared with them. Videos deemed irrelevant had non-Turkish or English content, were duplicated, and those without audio and any <2 minutes in length were excluded.
For each video, the variables recorded for analysis were the video source/uploader, video content, video length, time since upload, number of views, view ratio (number of views/day), number of likes, like ratio (like*100/[-like+dislike]), and (x) video power index, which is an index of video popularity based on the number of views and likes 7 calculated using the formula: like ratio*view ratio/100.
Video source/uploaders were categorized as urologists, non-urologist health professionals, video channels of urology associations, patients, TV programs, and health video channels with an unknown editor. We then grouped urologists, non-urologist health professionals, and video channels of urology associations as 'health professions' and patients, tv programs, and health video channels with an unknown editor as 'non-professional in health'.
The modified DISCERN, Journal of the American Medical Association (JAMA), and Global Quality Scale (GQS) scoring systems were used to assess video reliability. The modified five-item DISCERN tool has been widely used to examine the reliability of YouTube videos 7,8. This scale has five questions with yes/no answers, and each "yes" answer is scored as 1 point, giving a maximum of 5 points 9. The JAMA scoring system is a quality assessment tool used to evaluate information from health-related websites 7,8. It has four criteria, each with a possible score of 1. The GQS is a 5-point rating scale for Internet videos (lowest score, 1 point; highest score, 5 points). This scale measures the videos' quality, flow, and ease of use. A GQS score of 1 or 2 points indicated low quality, 3 points moderate quality, and 4 or 5 points high quality 7,8. In general, the JAMA score evaluates the reliability of a video, whereas the GQS score evaluates the educational quality 8,9.
The agreement between the two independent urologists rating and analyzing the videos was good, with kappa coefficients of 0.72, 0.85, and 0.73 for the modified DISCERN, JAMA, and GQS scales, respectively.
Descriptive statistics were applied to the data using minimum, maximum, frequencies and percentages. The normal distribution of numerical variables was assessed with the Shapiro-Wilk test. The comparison of the numerical variables in the two groups used the independent two-group t-test or the Mann-Whitney U test. The comparison of categoric variables used the chi-square or Fisher's Exact test. The percentage agreement between scores and the kappa coefficient was used to calculate interrater reliability. A kappa coefficient of 0.75-1.00 is considered excellent, 0.60-0.74 good, 0.40-0.59 fair, and <0.40 poor 10. The data were analyzed using the Statistical Package for Social Sciences (SPSS 20.0 for Windows, Chicago, IL, USA). Statistical significance was defined as p <0.05.
Results
The first 100 Turkish videos were examined, and found that 65 videos (65%) met the inclusion criteria (Figure 1A). Of the 65 videos, 58 and 7 were uploaded by health professionals and non-professional in health, respectively (Table 1). Forty videos (61.5 %) could be classified as low demand because of the low Video Power Index score, DISCERN, JAMA, and GQS values. It was found that any Turkish Health Association had uploaded a video about chronic prostatitis. While only six videos were patient testimonials, almost half of the videos by health professions (videos of health professionals) (43.1%) were interviews between the patient and the doctor who was the owner of the YouTube channel, which did not have any recognition YouTube plaque at the research time. (Table 2). In these videos, the urologist asked his patients some questions to learn and share his experience. The patient then answered the questions, and the urologist stopped the conversation and explained the patient's statements in technical language. The identity of the patients was hidden during the recording. The videos by non-professional in health (videos of non-professional in health) had a statistically significant longer duration and a lower like ratio than videos of health professionals (respectively p= 0.005, p= 0.041) (Table 3). However, the two groups had no significant differences between the views, like counts, Video Power Index, DISCERN, JAMA, and GQS values.
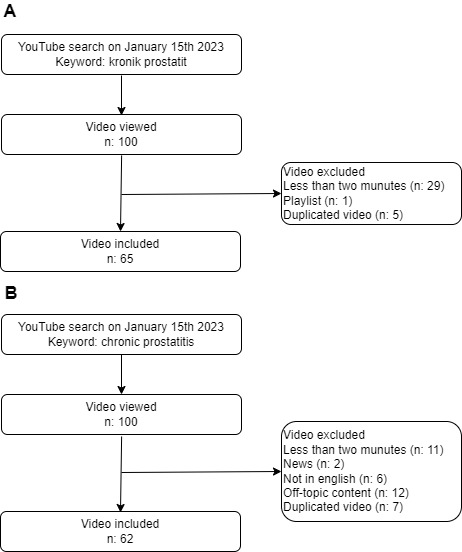
Table 1 Types of YouTube videos about of cronic prostatitis by language.
| Video makers | Turkish | English | Total | |
|---|---|---|---|---|
| Healthcare profession (n. %) | Urologist | 56 (86.2) | 22 (35.5) | 98 |
| Non-Urologist Health Professional | 2 (3.1) | 13 (21) | ||
| Urology Society Channel | 0 (0) | 5 (8.1) | ||
| Total | 58 | 40 | ||
| Non-professional in health (n. %) | Patient | 6 (9.2) | 10 (16.1) | 29 |
| TV program | 1 (1.5) | 2 (3.2) | ||
| Unknown Channel | 0 (0) | 10 (16.1) | ||
| Total | 7 | 22 | ||
| Total | 65 | 62 | 127 |
Table 2 Contents of YouTube videos about of chronic prostatitis by language.
| Turkish | English | Total | Between | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Video content (n. %) | HP (n=58) | NP (n=7) | p | HP (n=40) | NP (n=22) | p | HP (n=98) | NP (n=29) | p | p HPTurkish-HPEnglish | p NPTurkish-NPEnglish |
| Diagnosis | 5 (8.6) | 0 (0) | 0.029* | 2 (5) | 2 (9.1) | 0.305* | 7 (7.1) | 2 (6.9) | 0.002* | <0.001* | 1.000* |
| Etiology | 6 (10.3) | 0 (0) | 2 (5) | 1 (4.5) | 8 (8.2) | 1 (3.4) | |||||
| Treatment methods | 8 (13.8) | 2 (28.6) | 16 (40) | 4 (18.2) | 24 (24.5) | 6 (20.7) | |||||
| Patient Interview | 25 (43.1) | 0 (0) | 10 (25) | 0 (0) | 35 (35.7) | 0 (0) | |||||
| All | 14 (24.1) | 5 (71.4) | 10 (25) | 15 (68.2) | 24 (24.4) | 20 (69) | |||||
HP: Healthcare profession NP: non-professional in health
* Fisher's Exact Test
The first 100 English videos were examined, and 62 (62%) met the inclusion criteria (Figure 1B). Of the 62 videos, 40 and 22 were uploaded by health professionals and non-professional in health, respectively (Table 1). Thirty-four videos (54.8 %) could be classified as low demand because of the low Video Power Index score, DISCERN, JAMA, and GQS values. Five videos (8.1%) were uploaded by the video channels of Health Associations (Table 2). 10 videos (25%) were urologist-patient interviews, and these had been uploaded by the same Turkish urologists who had uploaded videos of the same concept videos in Turkish. English was used in these videos because the patients were not of Turkish origin. Although videos of health professionals were found to have greater DISCERN and JAMA values (p= 0.021, p= 0.024), videos of non-professional in health had more views and a greater view ratio and Video Power Index than videos of health professionals (p= 0.020, p= 0.044, p= 0.037) (Table 3). The two groups had no significant differences in like counts and the like ratio.
Table 3 Analysis of YouTube videos about of chronic prostatitis characteristics by language.
| Turkish | English | Total | Between | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| median (min-max) | HP (n=58) | NP (n=7) | Total (n=65) | p | HP (n=40) | NP (n=22) | Total (n=62) | p | HP (n=98) | NP (n=29) | Total (n=127) | p | p HPTurkish-HPEnglish | p NPTurkish-NPEnglish | p TotalTurkish - Total English |
| Views (n) | 3069 (126-310969 | 20599 (1111-250456) | 3288 (126-310969) | 0.063* | 6153 (149-73692) | 15387 (313-207769) | 8703 (149-207769) | 0.020* | 3440 (126-310969) | 15625 (313-250456) | 4825 (126-310969) | 0.001* | 0.638* | 0.646* | 0.193* |
| Likes (n) | 33 (0-2100) | 184 (12-4000) | 37 (0-4000) | 0.081* | 49.5 (1-1000) | 105 (6-1700) | 57 (1-1700) | 0.079* | 38 (0-2100) | 126 (6-4000) | 46 (0-4000) | 0.007* | 0.795* | 0.760* | 0.356* |
| Dislikes (n) | 0 (0-134) | 17 (0-162) | 2 (0-162) | 0.005* | 4 (0-54) | 4 (0-67) | 4 (0-67) | 0.373* | 2 (0-134) | 6 (0-162) | 2 (0-162) | 0.005* | 0.027* | 0.173* | 0.037* |
| Time Since Upload (day) | 467 (67-3112) | 41752 (487-1817) | 489 (67-3112) | 0.021* | 862 (96-3250) | 1162.5 (122-4620) | 896 (96-4620) | 0.317* | 625 (67-3250) | 1304 (122-4620) | 670 (67-4620) | 0.008* | 0.007* | 0.899* | 0.007* |
| Duration (second) | 339.5 (80-1247) | 750 (223-1020) | 350 (80-1247) | 0.054* | 393.5 (123-4678) | 552.5 (125-3604) | 450.5 (123-4678) | 0.366* | 349 (80-3250) | 557 (125-3604) | 397 (80-4678) | 0.019* | 0.327* | 1.000* | 0.120* |
| Like Ratio (like/like+dislike) | 0.99 (0-1) | 0.93 (0.86-1) | 0.99 (0-1) | 0.041* | 0.978 (0.56-1) | 0.96 (0.70-1) | 0.98 (0.56-1) | 0.944* | 0.987 (0-1) | 0.961 (0.703-1) | 0.98 (0-1) | 0.120* | 0.124* | 0.081* | 0.212* |
| View Ratio (view/day) | 9.93 (0.13-167) | 11.68 (1.33-392.56) | 9.93 (0.13-392.56) | 0.539* | 4.86 0.25-88.86) | 12.29 (0.71-379.1) | 6.535 (0.25-379.05) | 0.044* | 7.995 (0.134-167.008) | 11.68 (0.71-392.56) | 8.45 (0.13-392.56) | 0.064* | 0.059* | 0.878* | 0.342* |
| Video Power Index (like ratio*view ratio/100) | 0.85 (0-1.57) | 0.11 (0.01-3.77) | 0.09 (0-3.77) | 0.597* | 0.041 (0.01-0.87) | 0.12 (0.005-3.65) | 0.06 (0.01-3.64) | 0.037* | 0.074 (0-1.57) | 0.107 (0.005-3.772) | 0.08 (0-3.77) | 0.059* | 0.046* | 0.919* | 0.320* |
| DISCERN (1-5) | 1 (0-5) | 1 (0-1) | 1 (0-5) | 0.465* | 2.5 (1-5) | 1 (0-5) | 2 (0-5) | 0.021* | 2 (0-5) | 1 (0-5) | 2 (0-5) | 0.300* | <0.001* | 0.028* | <0.001* |
| JAMAS (1-4) | 1 (0-2) | 1 (0-1) | 1 (0-2) | 0.812* | 2 (1-4) | 1 (0-4) | 2 (0-4) | 0.024* | 1 (0-4) | 1 (0-4) | 1 (0-4) | 0.850* | <0.001* | 0.035* | <0.001* |
| GQS (1-5) | 1 (0-5) | 1 (0-1) | 1 (0-5) | 0.432* | 3 (1-5) | 1 (0-5) | 3 (0-5)) | 0.082* | 2 (0-5) | 1 (0-5) | 2 (0-5) | 0.382* | 0.002* | 0.021* | 0.001* |
HP: Healthcare profession NP: non-professional in health
*Mann Whitney U
Two hundred videos were examined, and 127 videos were included (Table 1). Health professionals uploaded 98 and 29 videos and non-professional in health (Table 2). Seventy-four videos (58.2 %) could be classified as low demand because of the low score of the Video Power Index, DISCERN, JAMA, and GQS values. Videos of non-professional in health were found to have greater total views, like (p= 0.001, p= 0.007) (Table 3). The two groups had no significant differences between the like ratio, Video Power Index , DISCERN, JAMA, and GQS values. When subgroups were examined, the Turkish videos of health professionals had greater Video Power Index (p= 0.046), while the English videos of health professionals had greater DISCERN, JAMA, and GQS values (p <0.001, p <0.001, p= 0.002).
When the total of Turkish and English videos was evaluated, there was no statistical significance in the view count, Video Power Index, and the like and view ratio. The English YouTube videos had significantly more value in DISCERN, JAMA, and GQS than the Turkish YouTube videos (respectively p <0.001, p <0.001, and p= 0.001)
Discussion
Chronic prostatitis is a subgroup of chronic pelvic pain syndrome and one of the undebated men's health problems. Although videos about chronic prostatitis on YouTube are one of the information source options, there has been no report about the characteristics, content quality, and reliability of YouTube videos about chronic prostatitis in the literature. However, YouTube videos primarily about bladder pain syndrome, also known as “Chronic pelvic pain syndrome”, have been evaluated and published with the search terms' bladder pain syndrome', "painful bladder syndrome," and "interstitial cystitis" 11,12. This study is the first to analyze YouTube videos' characteristics, content quality, and reliability about chronic prostatitis.
Although most of the Urological Associations have YouTube channels, we found that these urological association channels have uploaded no YouTube videos about chronic prostatitis for urologists or patients. Interestingly, however, a different type of video concept was detected, which has not been mentioned in the literature before, according to our knowledge. In this concept, the urologist interviews a patient diagnosed and treated by the urologist earlier. In the video, the YouTube viewers could not see the patient's face; they could only hear his voice. During the conversation, the patient talked about his chronic prostatitis experience. When the urologist needed to add some information, the urologist interrupted the conversation and turned to talk with the camera. The urologist repeated the patient sentences using the urological terms. The patient then re-started his speech, and the video continued in this manner. Finally, the patient mentioned the treatment method of this urologist and the benefits of this treatment. The urologist finished the video describing his treatment method. The same urologists uploaded these videos and if the patients were not of Turkish origin, the conversation was in English. Although there was no specific statistical data about this subtype of health professionals' videos, we found that these videos had greater view counts, like ratios and Video Power Index, compared to YouTube videos created with the usual concepts (unpublished data). One of the reasons for the Popularity of these videos was that the language used in the video was clear and accessible.
This study is the second study that compared YouTube videos between different languages. The first study was reported by Pratsinis et al. in 2021 13. In this report, the four most spoken languages at Europe (English, French, German, and Italian) and the three most common urological conditions (treatment of benign prostatic hyperplasia, prostate cancer, and urinary stone disease) were chosen, and a total of 240 videos were evaluated. The authors found that all videos had a low to moderate quality of content regardless of the language. Our study found that although there were no statistical differences in views and ratings in the two language group videos, English YouTube videos had higher quality than Turkish videos. As a result, it could be said that the Turkish health professions should pay more attention to making high-quality videos about chronic prostatitis.
Despite the ease of access and use, which are the benefits of YouTube videos, these videos can easily spread misinformation because YouTube has no editorial process. Especially during the pandemic, fake news and misinformation quickly spread worldwide, leading to widespread myths and serious misunderstandings. It is well-known that although YouTube could not be classified as a reliable health information source for patients 14, this video-sharing platform is one of the most used health information sources 15. YouTube viewers use this platform to find out about their health problems and learn about the experiences of others 16. According to our findings, almost half of the YouTube videos were in low demand, but the YouTube channels we evaluated did not have a recognition plaque, so it could be said that misinformation about chronic prostate did not find a chance to spread easily. Due to the popularity of YouTube videos, health professionals should upload more than non-professional in health. The differences between health professionals and non-professional in health should not only be in the number of videos but videos of health professionals should be more reliable, have higher quality, be easy to understand and be effective in-patient decision support, but there has been no mention of how to create effective YouTube videos in these guidelines.
This present study had several limitations. First, we only used 'kronik prostatit' for Turkish videos and 'chronic prostatitis' for English videos as a keyword. Although chronic prostatitis has other synonyms, we preferred to use these two keywords to search only for videos about chronic prostatitis. With the two keywords, we did not need to exclude other irrelevant videos and only evaluated relevant content. Second, we used validated scores to exclude reviewer bias. Then, we analyzed the agreement between the two independent reviewers with kappa coefficients and found that the agreement between them was consistent. Third, we used the modified DISCERN, JAMA, and GQS to evaluate the videos' quality and reliability but did not evaluate understandability with any validated tool, such as the Patient Education Materials Assessment Tool for audio-visual content. Fourthly, the study did not include shorts, live streams, or streamings, as well as new and very popular feature content. Fifthly, we did not have data on whether the channels monetized their accounts through content that could be related to the reliability and quality of videos. Finally, although YouTube content is known to change over time, our search was performed on a specific date; as such, any later search may yield slightly different results.
Conclusion
We found that while videos of health professionals were more reliable and had higher quality, videos of non-professional in health had better ratings, similar to findings in the literature. Health associations should pay more attention to medico-legal considerations and organize training programs on creating compelling social media content with greater reliability and quality, which is likely to be viewed and rated more often. Furthermore, they should create and upload more social media posts and videos and encourage health professionals to share these instead of content that the health professionals themselves may make where they lack sufficient knowledge to create effective posts. With more reliable, higher-quality videos that fit YouTube's algorithm, spreading misinformation and fake news on this topic could be easily blocked.

