










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Ciencias de la Salud
versión impresa ISSN 1692-7273versión On-line ISSN 2145-4507
Rev. Cienc. Salud v.9 n.1 Bogotá ene./abr. 2011
The Role of Kinaesthetic Motor Imagery in Promoting Activation of the Lumbrical Muscles in the Hemiparetic Hand:
a Randomised Controlled Study
El papel de la imagen cinestésica motora en la promoción de la activación de los músculos lumbricales en la mano hemiparética:
un estudio controlado aleatorizado
O papel da imagem cinestésica motora na promoção da ativação dos músculos lombricais na mão hemiparética:
um estudo controlado aleatorizado
Jonathon O'Brien 1, R. Martyn Bracewell 2, Juan Alberto Castillo-Martínez 3
1 Bangor University, School of Psychology. Adeilad Brigantia, Penrallt Road, Gwynedd, LL57 2AS.
2 Bangor University, School of Psychology, Adeilad Brigantia, Penrallt Road, Gwynedd, UK, LL57 2AS; The Walton Centre NHS Foundation Trust, Lower Lane, Fazakerley, Liverpool, UK, L9 7LJ.
3 Universidad del Rosario. Calle 14, No. 6-25, Bogotá, Colombia.
Recibido: Diciembre 4 de 2009 • Aceptado: Noviembre 27 de 2010
Para citar este artículo: O'Brien J, Castillo-Martínez JA, Martyn-Bracewell R. The role of kinaesthetic motor imagery in promoting activation of the lumbrical muscles in the hemiparetic hand: a randomised controlled study. Rev. Cienc. Salud 2011; 9 (1): 5-16.
Abstract
The objective of the investigation who gave as result this work was to investigate the effectiveness of kinaesthetic motor imagery in the activation of the hemiplegic hand muscles following stroke. The experiment consisted of two random groups. Movements were measured after treatment. The participants were ten patients with hemiplegic hands (men who mean age was 74.4 years; mean time since stroke 3.05 months). All patients received three sessions of physical treatment based on an identical treatment protocol. Five patients were randomly assigned to an experimental group practising kinaesthetic motor imagery of a grasp using the 'lumbrical action' (experimental group). The others five (control group) followed a relaxation script. All the patients were then asked to grasp an object using the 'lumbrical action'. The grasps were recorded using an optoelectronic motion capture system. The magnitude of the extension of the index finger and the correlation of the angular displacement of the proximal phalangeal joints and the metacarpophalangeal joints were calculated. The movement time for the whole grip was calculated. The experimental group demonstrated higher extension in the index finger (p = < 0.01) and they had a higher correlation coefficient (0.99) than the control group (0.77) for the displacement of the proximal interphalangeal joint and the metacarpophalangeal joints. The movement time for the experimental group was faster, although the difference was not significant.
Key words: stroke, hemiplegia, hand, motor imagery.
Resumen
El objetivo de la investigación que dio como resultado este trabajo fue indagar sobre la eficacia de la imagen motora kinestética para facilitar el movimiento de los músculos lumbricales hemipléjicos debido a la enfermedad cerebro-vascular. El diseño consistió en un experimento en el que participaron dos grupos elegidos aleatoriamente, los cuales se sometieron a mediciones a sus movimientos después de un tratamiento prediseñado. Los participantes fueron diez pacientes con manos hemipléjicas (hombres de edad promedio: 74.4 años; tiempo de evolución promedio del evento: 3.05 meses). Todos recibieron tres sesiones de tratamiento físico basado en un protocolo idéntico. Cinco pacientes seleccionados aleatoriamente (grupo experimental) practicaron imagen motora kinestética de un agarre usando 'la acción lumbrical'. Los otros cinco pacientes (grupo de control) siguieron un guion de relajación. A todos los pacientes se les pidió apretar un objeto usando el agarre de 'la acción lumbrical'. Los agarres fueron grabados usando un sistema de captura-movimiento optoelectrónico. Se calculó la magnitud de la extensión del índice y la fuerza de la correlación del desplazamiento de la articulación metacarpos falángicos e inter-falángicos próximos. El tiempo de movimiento fue calculado para el agarre. El grupo experimental mostró extensión en el índice más alto (p = < 0.01) y tuvo un coeficiente de correlación superior (0.99) que el grupo de control (0.77) para el desplazamiento angular de las articulaciones metacarpo-falángicas e inter-falángicas próximas. El tiempo del movimiento para el grupo experimental fue más rápido, aunque la diferencia no fue significativa.
Palabras clave: enfermedad cerebro-vascular, hemiplejia, mano, imagen motor.
Resumo
O objetivo da pesquisa que deu como resultado este trabalho, foi indagar sobre a eficácia da imagem motora cinestésica para facilitar o movimento dos músculos lombricais hemiplégicos devido à enfermidade cérebro-vascular. O desenho consistiu em um experimento no que participaram dois grupos elegidos aleatoriamente, os quais se submeteram a medições de seus movimentos depois de um tratamento pré-desenhado. Os participantes foram dez pacientes com mãos hemiplégicas (homens de idade em média de 74.4anos; tempo de evolução em média do evento: 3,05 meses). Todos receberam três sessões de tratamento físico baseado em um protocolo idêntico. Cinco pacientes selecionados aleatoriamente (grupo experimental) praticaram imagem motora cinestésica de um agarramento da "ação lombrical". Os outros cinco pacientes (grupo de controle) seguiram um roteiro de relaxamento. A todos os pacientes se lhes pediu apertar um objeto usando o agarramento da "ação lombrical". Os agarramentos foram gravados usando um sistema de captura-movimento optoeletrônico. Calculou-se a magnitude da extensão do índice e a força da correlação do deslocamento da articulação metacarpofalângica e interfalângica próximas. O tempo de movimento foi calculado para o agarramento. O grupo experimental mostrou extensão no índice mais alto (p = < 0.01) e teve um coeficiente de correlação superior (0,99) ao grupo de controle (0,77) para o deslocamento angular das articulaçães metacarpofalângicas e intefalângicas próximas. O tempo do movimento para o grupo experimental foi mais rápido, ainda que a diferença não foi significativa.
Palavras chave: enfermidade cérebro-vascular, hemiplegia, mão, imagem motora.
Introduction
The ability to actively extend the fingers is a strong predictor of upper limb recovery in post stroke hemiparesis (1, 2). However isolated finger extension is not a sufficient condition for recovery of manual dexterity. This requires, in addition, co-ordinated action of the metacarphalangeal (MCP) and proximal interphalangeal (PIP) joints (3). The co-ordination of extension of the PIP with simultaneous flexion of the MCP is known to be underpinned by the action of the hand lumbrical muscles (4). This group is unique in that one contraction produces both extension at the PIP and flexion at the MCP, making it crucial for dextrous movement (5). We therefore decided to focus on the lumbricals during hand rehabilitation following stroke.
In this study the effectiveness of motor imagery training in facilitating activation of the hand lumbrical muscles in post-stroke hemiparesis was explored. Motor imagery training has been defined as the mental rehearsal of an action without actually executing that action (6). It is considered to be a cognitive process dependent on the mechanisms of working memory (7, 8). It has been shown to be effective in training an action involving an intrinsic foot muscle (9) and in increasing force production in an intrinsic hand muscle (10). Controlled studies have also demonstrated absolute (11) and statistically significant differences (12, 13) in upper limb function in stroke patients using the technique alongside physical treatment.
Motor imagery can utilize different sensory modalities (14, 15, 16). In the present study kinaesthetic motor imagery (KMI) was used. KMI is based on imagining the sensations of movement which would be derived from the muscle spindles, Golgi tendon organs, and receptors in the joints and skin (17). To the best of our knowledge, the role of KMI in promoting focused activation of the lumbrical muscles in the hemiparetic hand has not yet been investigated.
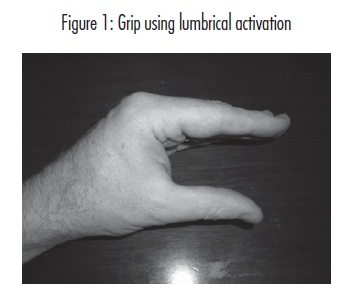
We assumed that a grip underpinned by lumbrical activation would be distinguished by extension of the PIP joint alongside flexion of the MCP. This is illustrated in figure one.
We then hypothesised that practise of this grip with the hemiparetic hand following KMI training would: 1) facilitate greater extension in the index finger PIP joint; 2) lead to stronger correlation of MCP and PIP angular displacement in the same index finger. Finally, because evidence has linked impaired interjoint coordination to reduced velocity in upper limb hemiplegia(18) we hypothesised that improved MCP-PIP co-ordination following KMI would facilitate shorter movement time (MT) for the whole grasping movement.
Methods
Participants
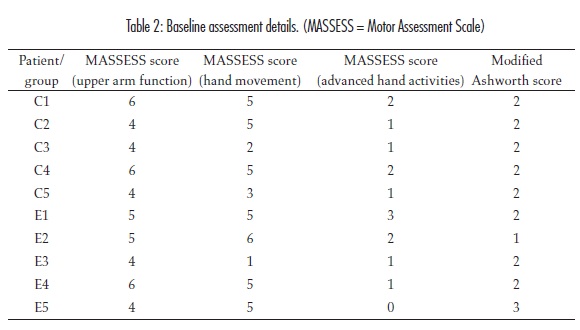
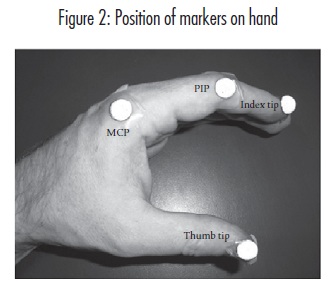
Hospitalized and ambulatory patients with stroke were recruited from two university hospitals in Bogotá. Exclusion criteria were: 1) The stroke occurred more than six months prior to the study commencing; 2) Cognitive deficit, evidenced by inability to follow instructions during administration of the baseline tests; 3) Scoring more than three on the Modified Ashworth Scale (MAS); 4) Scoring less than one on the Motor Assessment Scale hand movement test; 5) Over eighteen years of age. Ten patients with hemiparetic hands were recruited (five male, five female; ages 57-92, mean age [SD], 74.4 [10.3]; mean time after stroke [SD], 3.05 months [1.8]). Demographic and baseline assessment details are given in tables one and two respectively.
Instruments
A baseline assessment of upper limb function was conducted using the Motor Assessment Scale. This scale has been shown to demonstrate both reliability (19) and validity (20) Assessment is based on the performance of functional tasks on which the patient is scored on an ascending scale from zero to six. The examiner may use separate segments of the Motor Assessment Scale without compromising reliability or validity (20). In this study only the three upper limb components of the assessment were used. An assessment of upper limb muscle tone was also conducted using the MAS, which has been shown to demonstrate interrater reliability (21).
Ethics
Ethical approval was granted by the University of Rosario ethics committee in accordance with the declaration of Helsinki. All patients included in the study signed an informed consent form.
Overview of procedure
All participants received three physical treatment sessions on their hemiparetic hand based on an identical physical treatment protocol (appendix 1). Treatment was given by a trained occupational therapist and was aimed at activation of the hand lumbrical action. This action involves extension of the interphalangeal joints with flexion of the MCP joints (5). Treatment sessions took place in the hospital and in the laboratory prior to the experimental or control procedure commencing.
Upon arrival in the laboratory the patients were seated comfortably at a desk. Once all physical hand treatment had finished they were randomised to a control or experimental group by tossing a coin. In order to ensure equal numbers in each group the final patient was assigned to the control group. All patients then watched a video showing a hand grasping an object using the lumbrical action (figure 1).
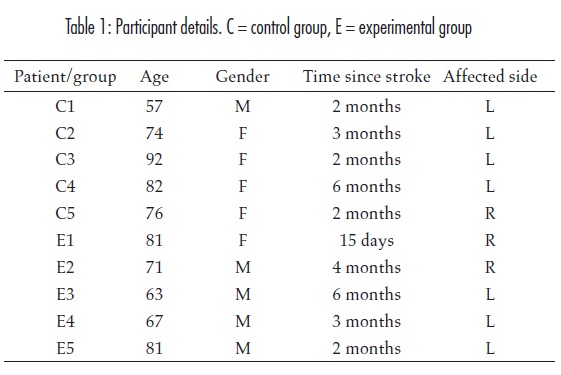
Reflective markers were placed on the tip of the index finger, the index PIP joint, the index MCP joint and the thumb tip of the hemiparetic hand (figure 2).
The patients randomised to the experimental group listened to a tape recorded KMI task focusing on the activation of the lumbrical muscles of the paretic hand (appendix 2). The patients in the control group listened to a guided relaxation task which focused on general muscular relaxation. After listening to the KMI and relaxation tasks both patients were asked to grasp a compact disc case (15.5 cm in length, 16.5cm high and 5cm wide) 14 times using the lumbrical action.
Data analysis
Hand movements were captured at 50hz using a six camera optoelectronic system (BTS Bioengineering, Milan). Ten of the recorded grasps from each patient were analysed. Kinematic analysis was carried out using SmartAnalyzer software (BTS Bioengineering, Milan).
The MT for each grasp and angular displacement values for the PIP and MCP joints during the grasp were obtained. The timing of each grasp was then normalised and the angular displacement values interpolated with splines using MATLAB® software. This allowed comparison of the whole movement across participants. Ensemble averages (22) were created from these interpolated displacement values. Curves of angular displacement over time were then constructed. These curves were divided for analysis into three phases: 1) the approach phase, as the hand closed around the object; 2) the hold phase, as the hand grasped the object; 3) the leave phase as the hand left the object (figure 3).
Kinematic variables and statistical analysis
-
Mean divergence of the index PIP joint from the target extension of 180° provided a measure of constant error (CE). An inde-pendent samples two tailed t test was used to compare differences in CE across the control and experimental groups. Proba-bility of error (p) value less than 0.05 was taken as significant. Significant differences were then tested with omega squared (w2) to see how much of this difference could be explained by the effect of KMI.
-
To measure correlation between MCP and PIP angular displacement values a correla-tion co-efficient (r) was calculated for these values for both groups.
-
Mean overall MT for both groups was compared using the t test.
Results
Table 3 shows that CE (SD) for the approach phase was 16.6° (6.68°) for the experimental group and 28.6° (10.37°) for the control group. The difference was not significant.
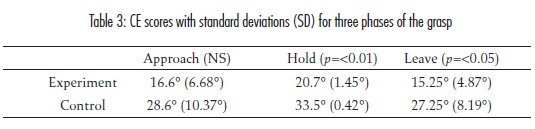
CE (SD) (figure 3) during the hold phase was 33.5° (0.42°) for the control group and 20.7°(1.45°) for the experimental group. The difference was significant (p=<0.01). w2 was 0.98, indicating that 98% of the difference could be explained with reference to the use of KMI.
CE (SD) (table 3) during the leave phase was 27.25° (8.19°) for the control group and 15.25° (4.87°) for the experimental group. The difference was significant (p=<0.05). w2 was 0.41, indicating that 41% of the difference could be explained with reference to the use of KMI.
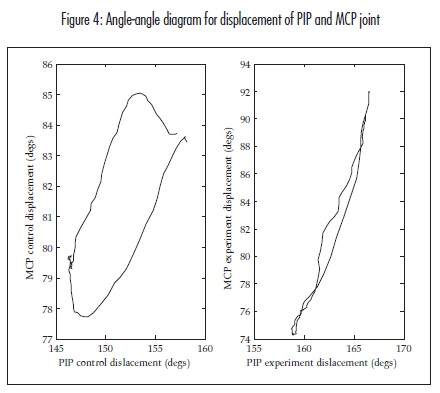
Figure 4 shows the angular displacement of the PIP and MCP joints for the control group and experimental group. Correlation coefficients (r) were calculated for these displacement values. r for the experimental group was 0.99, which was significant (p=<0.01). r for the control group was 0.77, which was not significant.
Mean (SD) MT was 3.54s (1.01s) for the control group and 2.11s (0.51s) for the experimental group. The difference was not significant.
Discussion
The aim of this study was to ascertain if KMI can facilitate activation of the hand lumbrical muscles in the post-stroke hemiparetic hand. Our hypotheses were: 1) KMI training would facilitate greater extension in the index PIP joint during grasping and to explore this we looked at mean divergence from a target of 180° extension for the index finger PIP joint (CE); 2) KMI training would promote a stronger correlation in the MCP-PIP joint displacement profiles during grasping and to assess this we calculated r values for MCP and PIP angular displacement for both groups; 3) KMI training would promote a faster mean MT for the whole grasp.
Table 3 shows that the CE for the PIP displacement of the experimental group during the hold phase of the grasp was found to be significantly lower than that for the control group (p=<0.01). The CE for PIP displacement during the leave phase of the grasp was also found to be significantly lower for the experimental group (p=<0.05). This indicates that the experimental group came closer to achieving the target PIP angle of 180° extension. In addition the MCP-PIP angular displacement correlation coefficient for the experimental group was 0.99 was significant (p=<0.01), while the correlation co-efficient for the MCP-PIP displacement for the control group was 0.77 (non-significant). MT for the experimental group was about 1.6 times faster than for the control group (non- significant). These results suggest we may accept the initial hypotheses. However, there are reasons for caution, outlined below.
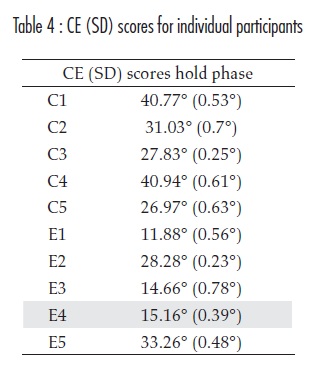
Firstly, there was no pre- and post-experiment comparison of the patients' performance. This made it difficult to gauge the degree of improvement in lumbrical activation. We would stress, however, that comparison of individual patients' CE scores indicates that improvement did occur. For example, referring to table 4, it can be seen that patient E5 scored zero on the Motor Assessment Scale advanced hand activities test and had the highest MAS score of three, while patients C1 and C4 scored two on the Motor Assessment Scale advanced hand activities test and had an MAS score of two. These figures indicate a lower level of manual dexterity for E5 at baseline. However, referring to table four, it can be seen that, following KMI training, E5 achieved a lower CE (SD) score of 33.26° (0.48°) during the hold phase, compared with 40.77° (0.53°) for C1 and 40.94° (0.61°) for C4. These results signal improvement for E5 in line with our first hypothesis. In another comparison, patient E3 scored one and patient C5 scored three on the Motor Assessment Scale hand movement test (table 2). This indicates a lower degree of manual dexterity for E3 at baseline. However table four shows that, following KMI training, CE(SD) for E3 was lower during the hold phase at 14.66° (0.78°) than for C5 at 26.97° (0.63°). Again, this would suggest improvement for E3 in keeping with our initial hypothesis.
A second limitation concerns the randomisation process. The same researcher was delivering the physical treatment as well as assigning patients to group. It was necessary, therefore, to ensure 'masking', so that the investigator would not know in advance which group the patient would be allocated to. This was done by tossing a coin at the end of the course of physical treatment to decide allocation. However for the last patient treated it was clear in advance which group he would go into. There may therefore have been the possibility of bias during the administration of the treatment protocol. A mitigating factor here is that this final patient, C1, was actually one of three patients with the second highest Motor Assessment Scale advanced hand activities score at baseline (table 2). As he was placed in the control group it is felt that he was unlikely to have biased the results in favour of the experimental hypotheses.
Another potential problem concerns the wide age range of the participants. Apart from the inclusion criteria described in the methods section, age was not treated as an independent variable in the study. Research has suggested that older people may be able to use motor imagery as effectively as younger people (23). However, it also suggested that the effects of motor imagery training may be less specific in the older population, with increased activation in muscles not identified as prime movers in the training task. This may be related to reduced selectivity in pyramidal tract function in older people (23). It may therefore be the case that age may, in part, be a confounding factor which should be taken into account in future research.
One final limitation of the study is the small sample size. Here, we would stress that the t test does take account of this, in that a smaller sample requires a higher critical ratio for the identification of statistically significant difference. This is also true for the test used to assess r for statistical significance. However, a larger sample would still be desirable.
One finding which requires explanation is the significant difference for CE at (p=<0.01) for the hold phase of the grasp and the higher p value of <0.05 for significant difference of CE in the leave phase. This may be explained by examining the t test, which is based on a comparison of measurements of mean magnitude and SD for single variables across the control and experimental group. If the SD values for both groups are low and close, while a larger gap is maintained between the measurements of mean magnitude for the groups, then statistically significant differences are more likely (24).
In our study these conditions were met most markedly during the hold phase, explaining the lower p value during this segment (table 3). It is likely that the resistance of the grasped object during this phase acted to stabilise the PIP joint and reduce variance. During the leaving phase of the movement this stabilising factor was not present, leading to higher and more divergent SDs and so producing a higher p value.
The results of this study suggest that KMI, alongside physical treatment, is an effective means to facilitate activation of the lumbrical muscles in the hemiparetic hand. However, the inclusion of a pre- and post experiment assessment of function, an improved randomisation process, age related stratified sampling and a larger sample size would strengthen the robustness of these findings.
Acknowledgements
Dr. Steve Hansen commented on the initial experiment design. Dr. Antonio Miguel assisted with mathematical aspects of data preparation. Fontayin Horta and other staff and students at Barrios Unidos and Mayor University hospitals, Bogotá, helped identify appropriate study participants and assisted with patient transport. Patients and their families gave their time generously. Central University, Bogotá, kindly allowed the use of their human movement laboratory.
Appendix one
Protocol for hemiplegic hand therapy physical treatment
1. Sensory stimulation of sides of hand using pencil edge, starting with medial border (abductor digiti minimi), and including sides of fingere, finger tips and web spaces, returning to abductor digiti minimi to finish. Repeated twice.
2. Facilitation of thumb opposition, repeated five times.
3. Facilitation of activation in lumbrical muscles, repeated 10 times.
4. Facilitation of lumbrical action in individual fingere, repeated five times for each finger.
5. Facilitation of abduction in index finger, repeated five times. Facilitation of abduction in little finger, repeated five times.
6. Facilitated placing of hand on table, with medial border making contact first each time. Repeated three times.
Appendix two
Script for guided KMI training
The following words were used:
"Concéntrese en su respiración, inhale y exhale normalmente, olvidándose de cualquier otro sonido adentro o afuera de esta habitación, sólo concéntrese en su respiración. Olvídese de las preocupaciones. Cierre los ojos si desea, pero evite quedarse dormido".
This initial relaxation script was repeated 6 times. The following script was then used:
"Relaje los músculos, en particular, concéntrese en relajar el lado de su cuerpo que ha sido afectado por el accidente cerebro vascular. Ahora recuerde el video sobre la mano realizando la acción de coger que vio anteriormente. Imagine que su mano débil hace ese movimiento. Imagine la sensación de los nudillos contrayéndose hacia arriba mientras los dedos se mantienen firmes. Recuerde mantener su mano quieta, mientras imagina la sensación de movimiento".
This script was repeated 6 times
Once this script was repeated 6 times the following words were used:
"Ahora vuélvase consciente de su presencia en esta habitación, si tenía los ojos cerrados ábralos nuevamente y observe a su alrededor. La sesión ha terminado".
Script for guided imagery focusing on general sensory awareness
The following words were used:
"Concéntrese en su respiración, inhale y exhale normalmente, olvidándose de cualquier otro sonido adentro o afuera de esta habitación, sólo concéntrese en su respiración. Olvídese de las preocupaciones. Cierre los ojos si desea, pero evite quedarse dormido".
This initial relaxation phase was repeated 3 times. This was followed by the following words:
"Concéntrese en sus piernas y pies y relájelos. Concéntrese en sus manos y brazos y relájelos. Ahora que se siente relajado, concéntrese en los sonidos que le rodean. Ahora concéntrese en su respiración por un tiempo más, respire normalmente".
This script was repeated 5 times. The following words were then used.
"Ahora vuélvase consciente de su presencia en esta habitación, si tenía los ojos cerrados ábralos nuevamente y observe a su alrededor. La sesión ha terminado".
References
1. Smania N, Paolucci S, Tinazzi M, Borghero A, Manganotti P, Fiaschi, A, et al. Active finger extension: a simple movement predicting recovery of arm function in patients with acute stroke. Stroke 2007; 38:1088-1090. [ Links ]
2. Fritz SL, Light KE, Patterson TS, Behrman AL, Davis SB. Active finger extension predicts outcomes after constraint-induced movement therapy for individuals with hemiparesis after stroke. Stroke 2005; 36:1172-1177. [ Links ]
3. Raghavan P. The nature of hand motor impairment after stroke and its treatment. Current Treatment Options in Cardiovascular Medicine 2007; 9:221-228. [ Links ]
4. Long C. Intrinsic-extrinsic muscle control of the fingers: electromyographic studies. The Journal of Bone and Joint Surgery 1968; 50:973-984. [ Links ]
5. Palastanga N, Field D, Soames R. Anatomy and human movement - structure and function. London: Butterworth Heinemann; 2006. [ Links ]
6. Mulder T. Motor imagery and action observation: cognitive tools for rehabilitation. Journal of Neural Transmission 2007; 10:1265-1278. [ Links ]
7. Dickstein R, Deutsch, JE. Motor imagery in physical therapist practice. Physical Therapy 2007; 87:942-953. [ Links ]
8. Jeannerod, M. The cognitive neuroscience of action. Oxford: Blackwell; 1997. [ Links ]
9. Mulder T, Zijlstra S, Zijlstra W, Hochstenbach J. The role of motor imagery in learning a totally novel movement. Experimental Brain Research 2004; 154:211-217. [ Links ]
10. Yue G, Cole KJ. Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractions. Journal of Neurophysiology 1992; 67:5. [ Links ]
11. Page SJ, Levine P, Sisto SA, Johnston MV. A randomized efficacy and feasibility study of imagery in acute stroke. Clinical Rehabilitation 2001; 15:233-240. [ Links ]
12. Page SJ, Levine P, Leonard A. Effects of mental Practice on affected limb use and function in chronic stroke. Archives of Physical Medicine and Rehabilitation 2005; 86:399-402. [ Links ]
13. Page SJ, Levine P, Leonard A. Mental practice in chronic stroke - results of a randomized, placebo-controlled trial. Stroke 2007; 38:1293-1297. [ Links ]
14. Malouin F, Belleville S, Richards CL, Desrosiers J, Doyon J. Working memory and mental practice outcomes after stroke. Archives of Physical Medicine and Rehabilitation 2004; 85:177-83. [ Links ]
15. Dickstein R, Dunsky A, Marcovitz E. Motor imagery for gait rehabilitation in post-stroke hemiparesis. Physical Therapy 2004; 84:1167-1177. [ Links ]
16. Jeannerod M. Motor cognition: what actions tell the self. Oxford: Oxford University Press; 2006. [ Links ]
17. Schmidt RA, Lee TD. Motor control and learning: a behavioral emphasis. Champaign: Human Kinetics; 2005. [ Links ]
18. Cirstea MC, Mitnitski AB, Feldman AG, Levin MF. Interjoint coordination dynamics during reaching in stroke. Experimental Brain Research 2003; 151:289-300. [ Links ]
19. Carr JH, Shepherd RB, Nordholm L, Lynne D. Investigation of a new motor assessment scale for stroke patients. Physical Therapy 1985; 65:175-180. [ Links ]
20. Carr JH, Shepherd RB. Neurological rehabilitation - optimizing motor performance. Oxford: Butterworth Heinemann; 1998. [ Links ]
21. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Physical Therapy 1987; 67:206-207. [ Links ]
22. Robertson DGE, Hamill J, Caldwell G, Kamen G, Whittlesey S, editors. Research methods in biomechanics. Champaign: Human Kinetics; 2004. [ Links ]
23. Léonard, G, Tremblay F. Corticomotor facilitation associated with observation, imagery and imitation of hand actions:: a comparative study in young and old adults. Experimental Brain Research 2007; 177:167-175. [ Links ]
24. Vincent WJ. Statistics in kinesiology. Champaign: Human Kinetics; 1999. [ Links ]

