











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Secondary hypertension corresponds to 15 % of the causes of arterial hypertension, and among them, primary hyperaldosteronism is the most common cause of reversible hypertension, with a very characteristic clinical frame. It has a slightly higher prevalence in women, between 30 and 60 years, and is usually unilateral.
An aldosterone producing tumor of the adrenal cortex is the main cause of primary hyperaldosteronism and should always be excluded when in the presence of severe hypertension, since the standard treatment is surgical and leads to a stabilization of the tension pattern after a few months.
Case presentation
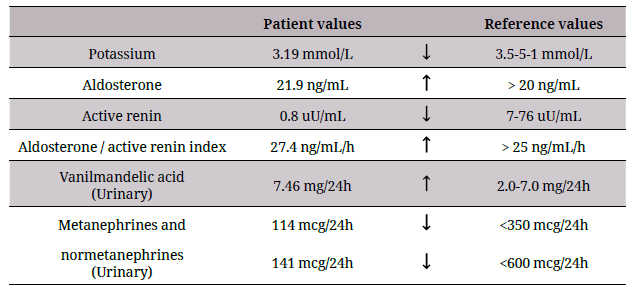
The authors describe the clinical case of a 63-year-old male patient who presented with a severe hypertension with five years of evolution, treated with four antihypertensive agents (nifedipine 60mg daily, losartan 100mg daily, nebivolol 5 mg daily, and rilmenidine 1mg daily) introduced sequentially, maintaining systolic blood pressure [BP] greater than 170 mmHg, with progressive worsening in the last two years. He is an autonomous patient, with history of non-insulin treated type 2 diabetes mellitus and a stroke, four years previously, without chronic sequelae. In the etiological study of hypertension, several analytical alterations were identified, and they are explained in table 1.
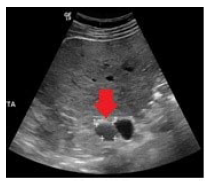
By ultrasonography, a nodular lesion was detected on the left adrenal gland (figure 1) which was subsequently confirmed by abdominal CT, showing a solid lesion of about 2.5 cm on the left adrenal gland. The patient was submitted to surgery and the lesion was excised with histological confirmation of a corticomedullary adenoma of the adrenal gland.
The patient presented improvement in his ambulatory blood pressure profile (with systolic BP around 130mmHg), and confirmed in 24 h ambulatory blood pressure monitoring (systolic BP 113-138 mm Hg and diastolic BP 66-78 mm Hg) seven months after the procedure, despite suspending two of the four antihypertensive drugs (nebivolol and rilmenidine, the latter still during the admission) and reducing the dose of the remaining ones (nifedipine to 30mg daily, losartan to 50mg daily). For the time being the patient maintains normalized aldosterone/active renin index and no hypokalemia.
Discussion
Hypertension causes significant morbidity and mortality worldwide, having a prevalence of about 30 % of the adult world population, and around 85 % of them above 55 years-old 1,2. Hypertension has the largest prevalence of all cardiovascular risk factors and, due to its deleterious effects on the cardiovascular and renal systems, it is considered responsible for 45 % of the heart disease related deaths and 51 % of them due to stroke 1,3.
The prevalence of hypertension increases with age and most individuals with hypertension are diagnosed with primary hypertension. Primary hypertension accounts for approximately 85 % of the diagnosed cases. It is estimated that approximately 15 % of hypertensive patients have identifiable conditions that result in blood pressure elevation (secondary hypertension) 4.
Common causes of secondary hypertension include obstructive sleep apnea, renal artery stenosis, chronic kidney disease, and endocrine alterations 3,4,5. Endocrine hypertension accounts for approximately 3 % of the secondary forms of hypertension and is a term assigned to states in which hormonal derangements result in clinically significant hypertension 4. The most common causes of endocrine hypertension are excess production of mineralocorticoids (primary hyperaldosteronism), catecholamines (pheochromocytoma), thyroid hormone, and glucocorticoids (Cushing syndrome) 4.
Primary hyperaldosteronism is the most common cause of reversible hypertension, with a reported prevalence of 5 % to 20 %, and presents in a myriad of clinical scenarios 1,4,6. Adrenocortical adenoma is the most common adrenal tumor. Because the majority of adenomas are non-functioning, most of these lesions are detected incidentally on routine imaging performed for unrelated reasons 7.
Primary aldosteronism is characterized by autonomous production of aldosterone by the adrenal glands along with suppressed renin production by the renal juxtaglomerular apparatus. This leads to volume expansion, severe hypertension, metabolic alkalosis, and hypokalemia 1,5,6,8. Classically, excessive aldosterone secretion in primary hyperaldosteronism not only results in difficult to manage hypertension in the majority of patients, but also produces biochemical effects of hypokalemia in 10 % to 30 % of patients 1. In many occasions, primary hyperaldosteronism is completely asymptomatic. When symptoms occur, they are usually secondary to hypertension or the resulting hypokalemia: cramps and fatigue; cardiac arrhythmias, manifested by palpitations; progressive weakness, even reporting cases of generalized paralysis; polydipsia and polyuria due to diabetes insipidus induced by hypokalemia 8. It is important to identify the existence of primary aldosteronism among resistant hypertensive patients since it is frequently curable, with clear reduction in disease burden 9.
Mineralocorticoid receptor antagonists absolutely interfere with the interpretation of the aldosterone/renin plasmatic index and should be discontinued at least six weeks before testing 8,10. Angiotensin converting enzyme inhibitors and angiotensin receptor blockers falsely increase plasma renin activity; therefore, a useful clinical point is that when plasma renin activity is undetectably low in a patient taking this type of medication, primary aldosteronism is suspected 10. Although it is the most used screening method in patients with suspected primary hyperaldosteronemia, given the low prevalence of this condition, the screening tests are reserved for those patients with resistant hypertension or hypertension associated with hypokalemia (even when hypokalemia is suspected to be secondary to the use of diuretics) 8.
The elevation of the aldosterone/renin index is a sensitive but not specific test, so that confirmatory tests are necessary in patients with elevated indexes 10.
There are four suppression tests used to confirm the alterations: oral sodium load, oral fludrocortisone load, oral captopril load and saline infusion to suppress aldosterone secretion; with the first and last being the most commonly used 10.
There is also an adrenal venous sampling, which is considered the gold-standard test to distinguish between unilateral or bilateral disease in patients with primary aldosteronism who desire surgical treatment of their hypertension. It is done by catheterization of femoral venous access, sampling blood from both adrenal veins and from the inferior vena cava below the renal veins and measurement of aldosterone and cortisol levels. The aldosterone/ cortisol index should be elevated in secretory tumor 10.
Adrenalectomy is the procedure of choice for unilateral aldosterone-secreting adenomas, while medical therapy is best for bilateral adrenal hyperplasia 1. Biochemical cure following adrenalectomy occurs in 99 % of patients, and hemodynamic improvement is seen in over 90 %, prompting a reduction in quantity and dosing of anti-hypertensive medications in most patients 1. End-organ damage secondary to hypertension and excess aldosterone is significantly improved by both surgical and medical treatment 1,4. Resistant hypertension is an increasingly common clinical problem that is often heterogeneous in etiology, risk factors and comorbidities. In light of diagnostic advances, evidence points to higher prevalence of secondary causes of hypertension, about 10 to 35 °/o 5. For diagnosing, patient's history and physical examination are important, as are assessing compliance, regular blood pressure measurement, biochemical evaluation and noninvasive imaging 3.
Although the most common causes of therapeutic failure are undiscovered secondary causes of hypertension and lack of patient compliance, other causes should be suspected, tested and, if confirmed, curable forms of arterial hypertension should be treated 3. Given the large impact on global health, controlling hypertension is of extreme importance 1.

