











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
The term intellectual disability (id) refers to those persons whose intellectual functioning is lower than the population average, characterized by the coexistence of two or more limitations "associated with adaptive areas in communication, home life, social skills, self-management, health and security" 1. In this sense, according to the American Association on Intellectual and Developmental Disabilities (AAIDD), in 2018, intellectual disability "is a disability characterized by significant limitations in both intellectual functioning (reasoning, learning, problem solving) and in adaptive behavior, which covers many everyday social and practical skills. This disability originates before the age of 18" 2.
For the purpose of this study, the population of children and youths with di was approached since it is in condition of disability with barriers to inclusion in different areas of daily life 3, and therefore with high indexes of obesity, thus in risk of acquiring chronic non-communicable diseases (CNCD) 4,5.
In this way, there is evidence of a notable increase of cardiovascular risk factors due to unhealthy lifestyles in children and youths with id, since their physical activity is far lower than that of their peers with no disability 5,6. Similarly, the presence of overweight and obesity in population with id is growing; according to Foley, Harvey, Hae-Ja and So-Yeun, as well as Sherill (1993) and Moreno (2003), quoted by Laureano, "Students in id condition present high obesity indexes and thus a higher risk of contracting chronic non-communicable diseases (CNCD)" 5.
In adults, certain researches show that there is a higher predisposition to present cardiovascular risk factors in the population with intellectual disability. In this sense, Ojeda and Crespo note in a study conducted in a Chilean population that 49 °% of the total sample present overweight or obesity, and 54.3 °% showed relative risk related to waist circumference 7. On the other hand, the Spanish Society for the Study of Obesity (SEEDO, for its initials in Spanish) warns that, according to a study of the University of Illinois at Chicago, usa, people with id present a four-fold risk of developing obesity with a body mass index (bmi) greater than 40, compared with their peers without this condition 8.
On the other hand, regarding physical fitness and cardiovascular risk, some studies, like the one conducted by Secchi, García, Espana and Pinero, propose establishing a relation between physical condition and indirect cardiovascular risk indicators, such as cardiovascular condition, in children without disabilities 9. In this study they found that 31.6 °% of children have a low aerobic capacity, a fact that is indicative of cardiovascular risk. Moreover, in the id population, Martínez, Ayán, and Cancela found in a study carried out in a Spanish population that "moderate id was associated with a greater cardiovascular disease risk (p = 0.042)"; the latter determined through waist circumference and body mass index as early indicators of cardiovascular risk associated with adiposity 10.
Therefore, it is still necessary to identify the early indicators of cardiovascular risk in the population of children and youths in order to promote health and the prevention of the disease through the practice of physical activity as an effective tool for the prevention of chronic non-communicable diseases.
In Colombia, assessing the physical condition of school students is a relatively recent aspect in the academic spheres. There are researches that, in the educational field, have taken the initiative to develop studies on this matter, however, the exclusion criteria of these studies include students with any disability, and have focused on the physical fitness of the population of school students with no without disabilities in order to determine standards and to validate assessment batteries 11,13.
Considering these studies, it is evidenced that the physical fitness could be a cardiovascular risk indicator, however, this is not known in the Colombian population with id. Therefore, the present study seeks to determine the relation between the physical fitness related to health and cardiovascular risk in students with intellectual disability.
Materials and Methods
This study has a quantitative cross-section, analytical approach. This quantitative approach uses data collection to prove a hypothesis, based on numerical measurement and statistical analysis in order to establish behavior patterns and prove the theory 14,15.
The study was conducted in the Gustavo Restrepo School, D campus, a school with exclusive classroom for id. The study selected 175 students who met inclusion criteria such as being enrolled in this school for the schoolyear 2016; aged between 15 and 22 years old; having been diagnosed by a physician with an id such as mild or moderate mental retardation (CIE-10 Classification) or Down syndrome; and having the approval of the parents through an informed consent. Exclusion criteria for the study were not having the parents' or guardians' approval through the signature of the informed consent; having a physical disability associated with a severe musculoskeletal or neurological disorder; and/or presenting medical restriction related to physical activity. This information was provided by the school together with the parents.
For the inclusion of the students as participating subjects, the signature of the informed consent was sought from the parents or legal guardians. Previous to the tests, a meeting with parents and guardians was coordinated in order to explain the research project, as well as its implications and scope. Besides, each participant was asked to present the results of a physical fitness test written by a general physician to detect any restriction for practicing physical activity. Permission to take pictures during the tests was also asked for.
In order to establish relations among variables, the independent variables to be considered were resistance force, flexibility, and cardiopulmonary performance, included in the fitness conditions for health. The variables related to body composition (body fat percentage, waist circumference, body mass index), considered as early indicators of cardiovascular risk and associated with adiposity, were established as dependent variables.
Considering the precedents presented before, confusion variables for the descriptive analyses included age, gender and type of disability; for the correlation analysis, the confusion variable was age.
For the present study, the variables included in the physical fitness for health: resistance force, flexibility, cardiopulmonary performance, and body composition, were assessed. Specifically, for the body composition variable following measuring tests were conducted: calculation of body weight and body fat, with impedance scale (r = 0.88 - 0.89; 95 °% ci =0.95) 16,17; height measurement, with measuring rod; and body mass index and waist circumference, with tape measure (in females: sensitivity 82.35 °%, specificity 78.77; in males: sensitivity 82.03 °%, specificity 94.83 °%); for assessing flexibility of the posterior trunk and lower limbs, the Sit and Reach protocol proposed by Winnick and Short was used; resistance was measured with the Curl Up Test (cci 0.095, R = 0.93-0.97) 16,17, Extended Arm Hang Test (alpha = 0.85 in population with mental retardation), and prehensile dynamometer (construct validity: Winnick and Short) 16,17; cardiopulmonary performance was assessed with the Course Navette Test and PACER (alpha = 0.97 in population with mental retardation) 16,17.
The Brockport Physical Fitness Test and the corresponding scales, a battery proposed by Joseph P. Winnick in 1999 for children and youths between 10 and 17 with disabilities, which was updated in 2014, was applied in children under 18 years of age. For the population older than 18 years, the protocols and scales of the American College of Sports Medicine were used; and for measuring body mass index, the who scales. In the Course Navette and PACER tests, the Leger et al. equation 16,17 was used, for children younger than 19 years: VO2Max = 31.025 + (3.238 x S) - (3.248 x A) + (0.153 x S x A); and for youths older than 19 years: 5.857 x S - 19.458 18.
The selection bias was minimized since all students had the possibility of participating in the research, meeting all inclusion and exclusion criteria described before.
In order to reduce and prevent measurement bias, training on the selected tests was provided to the persons who carried out the measurements. The researchers performed the measurements to prevent data manipulation and management.
In order to conduct the analyses, data were grouped by age, gender and diagnosis. This way, descriptive analyses were performed in youths younger and older than 18 years independently, as well as comparisons between males and females. Likewise, descriptive analyses by diagnosis were carried out considering the differential behavior put forward in literature between mental retardation and Down syndrome. Correlation analyses were performed in two groups, participants younger than 18 years and older than 18 years, taking into account that the data tests, scales and behaviors were different.
Data were registered in an Excel database that was exported to the SPSS version 20.1 program aiming at performing the respective multivariate and bivariate analyses with descriptive and analytical statistics. For the normality analysis, the Kolmogorov-Smirnov test, with a confidence level of 95 °%, was implemented. Measures of central tendency such as standard average and deviation were conducted for those continuous variables with normal behavior. Likewise, for correlations the Pearson correlation coefficient was used. The Spearman correlation coefficient, p (rho), a measure for the correlation between two aleatory variables was used for those variables not presenting a normal behavior.
This research complies with the postulates of the Declaration of Helsinki and the Resolution 8430 of 1993 relating to clinical researches in Colombia, since it is a moderate-risk research because the carried out interventions can change the baseline physiological conditions of these specific subjects 19,20. For this reason, the study was not performed in the population with medical contraindication for the practice of physical activity, or with any baseline pathology that could be affected with the implementation of the tests. Likewise, considering the Resolution 8430, an informed consent of the parents and guardians authorizing the participation or non-participation of their children was applied, moreover, an informed approval of each student was also implemented. The latter was reviewed by the psychosocial staff of the school the participating children and youths attend. This project had also the approval of the Advisory Committee of the Masters' Degree in Physical Education for Health of the University of Santo Tomás, in charge of approving the projects and ensuring the fulfilment of the ethical principles. By the time the project was conducted, the University did not have an ethics committee.
Results
One of the relevant findings shows the difference found in the contrasting results of males and females, warning that females have a poorer physical fitness with cardiovascular risk levels -this assessed with indirect indicators such as body mass index (BMI) and body fat percentage- greater than in males, particularly in the population older than 18 years. However, there are exceptions among males that alerts of a greater cardiovascular risk in some of them (figure 1, figure 2).
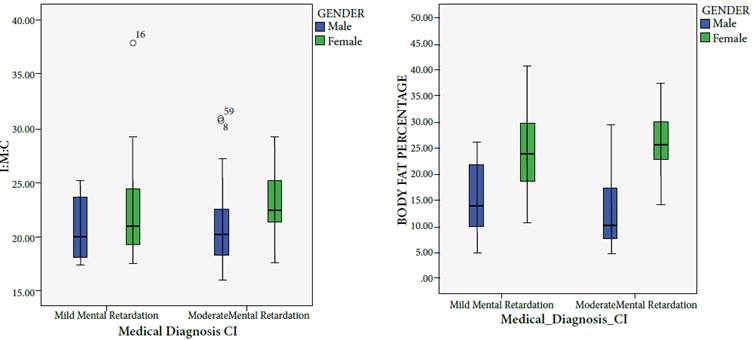
Figure 1 BMI and body fat percentage through medical diagnosis, grouped by gender, younger than 18 years
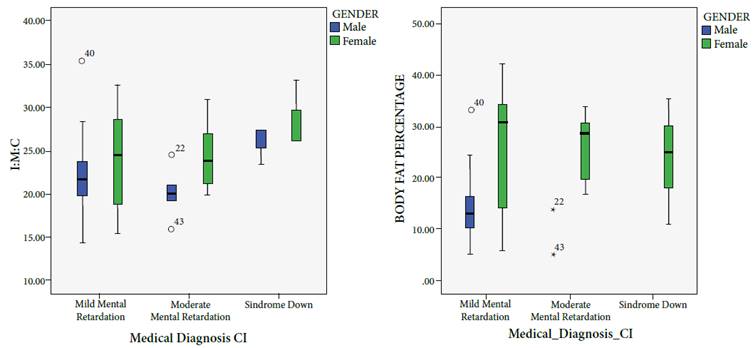
Figure 2 Body fat percentage and BMI through medical diagnosis, grouped by gender, in people older than 18 years
Regarding some physical fitness variables, such as cardiopulmonary resistance in the population younger than 18 years, the results were lower in females compared to those in males, constituting a higher cardiovascular risk in this population (figure 3).
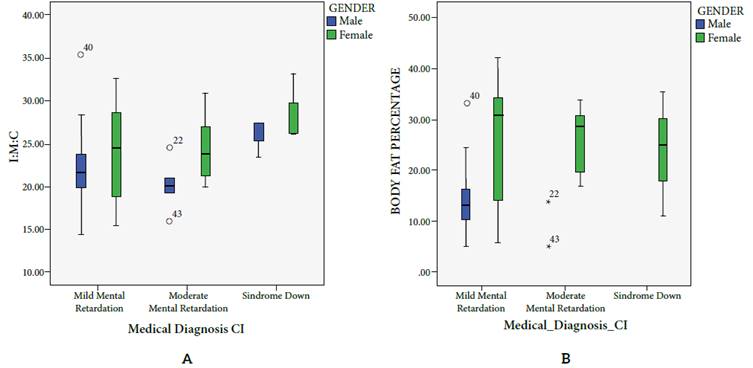
In population older than 18 years a third diagnosis comes up, Down syndrome (ds), which was not present in the population aged under 18 years. In this population cardiovascular risk is higher in those diagnosed with ds, since it is clear that their physical fitness shows poor and low results, while the anthropometric variables lie over the overweight and obesity levels, determined based on waist circumference, body fat percentage and BMI. Body fat percentage for males in general are found in normal valuation ranges, even though there are differences by diagnosis, showing a higher percentage in those diagnosed with ds. By contrast, females register high, and obesity values, higher than in females diagnosed with mild id (figure 2).
As to the cardiopulmonary condition in population older than 18 years, behavior was rated fair standard and low. In the population with ds, values for percentile 50 show a low physical fitness, slightly higher in some females who reach a fair standard condition. In the population diagnosed with moderate id, the difference between males and females is considerably higher for males, since the mean reaches a good, and in some case excellent physical assessment; the opposite in females, whose 50 percentile lies in a standar and downward physical assessment. For the population diagnosed with mild id, behavior is similar, but 50 percentile of males and females does not exceed that of the population diagnosed with moderate id.
Once the data was collected based on the assessed variables, the research clearly shows the low levels of physical fitness of the students with intellectual disability in the Gustavo Restrepo School, allowing to establish in an indirect fashion cardiovascular risk. However, considering the variables defined as cardiovascular risk predictors, following results are evidenced:
As to the relations between the physical fitness variables and the indirect variables with cardiovascular risk associated with adiposity, a significative and inversely proportional correlation between body fat percentage and force of the upper limbs (r = 0.593, p = 0.01) was found; as it is between body fat percentage and abdominal strength (r = 0.27, p = 0.01); as well as with aerobic capacity (-0.423, p = 0.01). In this population, waist circumference and bmi did not present any correlation with the physical fitness variables, where the body fat percentage could be considered the main risk predictor (table 1).
Table 1 Correlation between anthropometric (cardiovascular risk) and physical fitness variables in youths younger than 18 years old.
| BMI | Body Fat Percentage | Waist Circumference | ||
| VO2 Max | Pearson Correlation Sig (Bilateral) | -250* .048 | -.423** .001 | -.245 .053 |
| Abdominal Strengh | Pearson Correlation Sig (Bilateral) | -.027 .838 | -.272* .031 | -,.20 .878 |
| Arm Strength | Pearson Correlation Sig (Bilateral) | -.365** .003 | -.593** .000 | -.240 .058 |
*Correlation is significant at 3.05 level
** Correlation is significant at 0.01 level
Source: Master’s dissertation conducted by Marco Aurelio Rodríguez in the 2016 Master’s Degree Program in Physical Activity for Health, University of Santo Tomás, available in: https://repository.usta.edu.co/bitstream/handle/11634/4147/Rodriguezmarco2016.pdf?sequence=1&isAllowed=y
Regarding the correlations of the population older than 18 years, a high correlation (r = 0.78, p = 0.01) among the anthropometric variables, specifically among bmi, body fat percentage and waist circumference was observed, thus being in this case the waist circumference a fundamental risk indicator, in contrast to the population younger than 18 years. Considering the relations between the physical fitness variables and the indirect variables with cardiovascular risk associated with adiposity, findings show a significant and inversely proportional correlation between body fat percentage and the force of the upper limbs (r = 0.592, p = 0.01); bmi and the force of the upper limbs (r = 0.605, p = 0.01); between bmi and abdominal strength (r = 0.28, p = 0.05); as well as between body fat percentage and aerobic capacity (r = -0.471, p = 0.01) (table 2).
Table 2 Correlation between anthropometric (cardiovascular risk) and physical fitness variables in youth older than 18 years
| BMI | Body Fat Percentage | Waist Circumference | ||
| VO2 Max | Pearson Correlation Sig (Bilateral) | -.428** .001 | -.471** .000 | -.380** .005 |
| Abdominal Strengh | Pearson Correlation Sig (Bilateral) | -.258* .037 | -.262 .055 | -.172 .213 |
| Arm Strength | Pearson Correlation Sig (Bilateral) | -.605** .000 | -.592** .000 | -.560** .000 |
*Correlation is significant at 0.05 level
**Correlation is significant at 0.01 level
Source: Retrieved from the Master’s dissertation conducted by Marco Aurelio Rodríguez in the 2016 Master’s Degree Program in Physical Activity for Health, University of Santo Tomás, available in: https://repository.usta.edu.co/bitstream/handle/11634/4147/Rodriguezmarco2016.pdf?sequence=1&isAllowed=y
Discussion
he study allowed the comparison of the behavior of physical fitness by gender, age, and intellectual disability level, which showed a relation between physical fitness and the cardiovascular risk indirect indicators of the assessed students. Thus proving the hypothesis advanced here since the same findings showed that those students with greater waist circumference, higher body fat percentage and higher bmi, with values between overweight and obesity, presented lower VO2Max and in the same way, lower strength of the arms. These findings were similar to those presented by Secchi, Garcia, et al., who established that the population with intellectual disability present cardiovascular risk, determined based on the early indicators related to cardiopulmonary resistance 9. Likewise, relations between arms strength and early indicators of cardiovascular risk associated with adiposity have been found in the Colombian pediatric population without disability in the studies conducted by Rodriguez, et al., who found that "the best muscle performance was associated with better indicators of physical well-being" 21. They also affirm that "the assessment of muscle strength in early ages will allow the implementation of programs for cardiovascular and metabolic risk prevention", considering the power of an early risk predictor.
The difference between the population younger than 18 years and that older than 18 is also noticeable, since the minors show a better physical fitness and anthropometric values somehow apart from cardiovascular risk in the older population. With good, and sometimes excellent results for the VO2Max and strength values, corroborating that in the id population cardiovascular risk grows over the years in relation to the assessment of physical fitness and anthropometric condition, as Wouters, et al., put it, thus making them particularly vulnerable to health problems in adulthood 22.
One of the first conclusions of this research is having proved that it is possible to include populations with mild and moderate id and persons with ds in studies related to assessing physical fitness using reliable and internationally valid tests. This allowed evidencing the actual difference in terms of physical fitness in population with mild to moderate intellectual disability or Down syndrome. These findings are similar to those established by Martinez et al., who found in their study performed in a Spanish population that "moderate id has been associated with a higher risk of cardiovascular disease (p = 0.042)", the latter determined by measuring waist circumference and bmi as early indicators of cardiovascular risk associated with adiposity and also used in the present study 10. Likewise, Golubovic et al., obtained in their study significantly low results of the physical fitness performance in children with intellectual disability compared to typically developing children 23.
On the other hand, similarities with studies performed in population with id in other countries focused on assessing physical fitness associated with health were found, thus corroborating that overweight and obesity have become a problem of public health that are also present in the id population, not only in developed countries, it is also increasing in Latin America and, of course, in Colombia, as it was evidenced in this study 4,8,22.
Considering the correlation of gender, physical activity and body composition, the study showed that physical fitness in males presents higher values both for children younger than 18 years and for youths older than 18 years, thus proving that for them, the assertion that in this population there is lower participation in physical activity is maintained, not forgetting the case of some male subjects who show extreme high values of cardiovascular risk. In females, the VO2Max shows warning values since in the 50 percentile in females it has low levels, as it does in males with ds 24,26. As to body composition, females show values nearing cardiovascular risk figures in a higher proportion than in males, and even further nearer to this risk in the ds population.
Finally, it is worth mentioning that "there is consensus that the measure of waist circumference (wc) is an indirect indicator of the presence of intra-abdominal fat. This assessment is easily available and low cost, for this reason it is used to early predict the risk of suffering diseases such as diabetes mellitus, hypertension and cardiovascular conditions" 27. However, in the present study this variable is not considered a risk indicator for the population aged under 18 years, to whom it would be relevant to measure blood pressure, body fat and strength percentages, as Rodriguez et al. suggest 21.
Generally speaking, it can be asserted that in persons with id there is an inversely proportional correlation between age and physical fitness, since it was found that these variables decreased with increasing age and show lower percentiles in the individuals diagnosed with Down syndrome (SD).
This research reveals the physical fitness of students with id attending the Colegio Gustavo Restrepo, by using anthropometric and physical fitness variables that reflect the inversely proportional correlation between the physical fitness variables and the early cardiovascular risk indicators related to adiposity. Likewise, this research opens the door toward the possibility of future studies in this population since this population has been excluded in previous studies in Colombia related to assessing physical fitness in school students.

