











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Psychomotor development is defined as the set of skills that an infant acquires during the first two years of life, comprising the motor, cognitive, socio-affective, language, and sensory areas 1-4. In addition to the above, a delay in motor development can be caused by different risk factors, such as birth weight, gestational age, intrauterine growth restriction, mother's education and sociodemographic level. Play-based interventions and those that promote shared reading are more effective and feasible in developing countries 5-9.
Infants in rural areas of developing countries are twice as likely to present low birth-weight when compared with infants from urban areas, and 65% are likely to suffer from growth retardation 10. During the peri-gestational period, a series of factors that can influence or condition the normal growth and development of the fetus come together 11-13.
During the postnatal stage, the most frequent factors are respiratory distress syndrome, meningitis, periventricular hemorrhage, trauma, seizures, hyperbilirubinemia, hypoxia, and macro or microcephaly. The presence of the latter is in the range of approximately 12% in neuropediatrics; 50% of these are attributed to delayed motor maturation 14,15. Therefore, the objective of this study was to determine the sociodemographic and maternal risk factors associated with psychomotor retardation in infants that attend the SITI rehabilitation ward (sala infantil de tratamiento integral)-a comprehensive treatment ward for children at the Centro de Rehabilitación y Educación Especial in Villahermosa, Tabasco in 2017.
Materials and methods
A retrospective, observational case-control study was conducted on infants under two years old that attended the sin ward at the Centro de Rehabilitación y Educación Especial in Villahermosa, Tabasco in 2017.
The study population included those patients who visited the service during the months of January-June 2017, selected using non-probability convenience sampling, showing a 1:1 case and control correlation.
The case selection criteria included patients under two years of age who attended the rehabilitation ward with a diagnosis of psychomotor retardation. Exclusion: infants under two years old with psychomotor retardation secondary to other pathologies such as Down syndrome and infantile cerebral palsy, among others.
With regard to the control selection criteria, children under two years old were included when they were admitted to the unit without a diagnosis of psychomotor retardation and without clinical symptoms suggestive of it.
Patients with an inconclusive diagnosis suggestive of psychomotor retardation were excluded.
Data collection was performed using a 45-item questionnaire, which included variables such as the medical history diagnosis of psychomotor retardation and perinatal risk factors, such as the presence of trauma prior to the consultation or cases of previous infections reported by the mother or guardian, etc. were classified dichotomously. The data suggested by the socioeconomic evaluation carried out by the institution's social work department was used for the socioeconomic class assessment.
The data was processed and analyzed using the SPSS statistical program, version 23. Pearson's chi-square test and Fisher's exact test were used for the correlation of the variables, together with the odds ratio (OR), a 95% confidence interval (CI), and a significant association of variables with a p <.05 value was accepted.
This investigation was conducted following the Declaration of Helsinki guidelines and the Ley General de Salud (General Health Law) in its last reform, which was published DOF 06-01-2016, under the Fifth Title "Investigación para la Salud," a single chapter; articles 96 and 100, which mentions health research as an act that contributes to the development of knowledge of biological and psychological processes in humans 16,17. The children's guardians agreed to participate after signing an informed consent. This project was presented to and approved by the teaching field of the Centro de Rehabilitación y Educación Especial of the State of Tabasco and the Research and Ethics Committee of the Universidad del Valle de México, Villahermosa Campus.
Results
Seventy infants with psychomotor retardation and 70 clinically healthy pediatric patients without the condition under study were assessed; 43 of the cases were male and 27 were female.
The mean age of the infants was 3.26 ± 1.24 months for the confirmed cases and 3.02 ± 1.09 months for the controls.
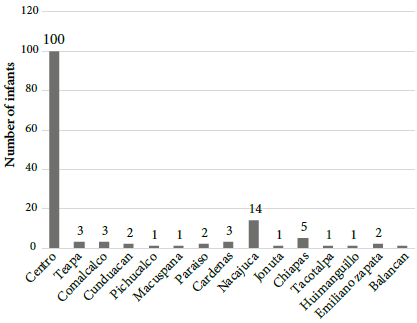
The majority of the children who attend the entity's rehabilitation center are from the municipality where the center is located, followed by Nacajuca in the state of Tabasco, as well as from the state of Chiapas (Figure 1).
Regarding the sociodemographic factors, only a low socioeconomic status showed a significant association with the presentation (p =.000; 95% CI = 0.349-0.80). The other variables such as the presence of piped water, location and drainage showed no relationship (p >.05) (Table 1).
Table 1 Relationship between sociodemographic factors and infants with psychomotor retardation.
| Variable | Psychomotor retardation | No psychomotor retardation | OR | 95% CI | gl | Value | p |
|---|---|---|---|---|---|---|---|
| Location | |||||||
| Urban | 34 | 42 | 0.63 | 0.3222-1. | 1 | 1.84 | 0.175* |
| Rural | 36 | 28 | |||||
| Piped water | |||||||
| Yes | 68 | 69 | 0.493 | 0.044-5. | 1 | 0.341 | 0.559* |
| No | 2 | 1 | |||||
| Drainage | |||||||
| Yes | 58 | 63 | 0.537 | 0.198-1. | 1 | 1.52 | 0.217* |
| No | 12 | 7 | |||||
| Socioeconomic status | |||||||
| Mean | 24 | 53 | 0.16 | 0.349-0.80 | 1 | 24.27 | 0.000* |
| Low | 46 | 17 | |||||
| Wall material | |||||||
| Brick | 13 | 6 | 3 | 5.679 | 0.128* | ||
| Block | 53 | 60 | |||||
| Laminate | 4 | 2 | |||||
| Wood | 2 |
*Pearson's chi-square test.
In relation to maternal history, a positive family history of psychomotor retardation showed 10-fold increased risk of presentation of the event (p =.000; 95% CI = 3.82-35.61). Mothers who presented with a disease during pregnancy had 3-fold increased risk of presentation compared to those who were clinically healthy (p =.002; 95% CI = 1.603-8.84), and a history of a traumatic accident showed 5-fold increased probability of presentation (p =.015; 95% CI = 1.32-18.76) (Table 2).
Table 2 Relationship between maternal factors and the presentation of psychomotor retardation
| PPsychomotoretardation | No psychomotor retardation | OR | 95% CI | gl | Value | p | |
|---|---|---|---|---|---|---|---|
| Family history | |||||||
| Positive | 29 | 4 | 11.67 | 3.82-35.61 | 1 | 24.781 | 0.000* |
| Negative | 41 | 66 | |||||
| Disease during pregnancy | |||||||
| Positive | 25 | 9 | 3.76 | 1.603-8.84 | 1 | 9.94 | 0.002* |
| Negative | 45 | 61 | |||||
| Medications intake | |||||||
| Positive | 5 | 4 | 1.29 | 0.326-4. | 1 | 0.500+ | |
| Negative | 65 | 66 | |||||
| Illegal substance | |||||||
| Positive | 0 | 3 | 2.045 | 1.72-2. | 1 | 3.066 | 0.080* |
| Negative | 70 | 67 | |||||
| Traumatic accident | |||||||
| Positive | 13 | 3 | 5.09 | 1.32-18.76 | 1 | 0.015+ | |
| Negative | 57 | 67 | |||||
| Type of delivery | |||||||
| Vaginal | 38 | 37 | 1.05 | 0.545-2. | 1 | 0.029 | 0.865* |
| Abdominal | 32 | 33 | |||||
| Gender | |||||||
| Male | 43 | 29 | 1.26 | 0.645-2. | 1 | 0.471 | 0.49 |
| Female | 27 | 31 |
*Pearson’s chi-square test; + Fisher’s exact test.
Regarding perinatal factors, only cases that were positive for infectious diseases prior to the consultation were more predominant in infants with psychomotor retardation (p =.000; 95% ci = 9.60-555.718) (Table 3).
Table 3 The relationship between perinatal factors and psychomotor retardation.
| Psychomotor retardation | No psychomotor retardation | OR | 95% CI | gl | Value | p | |
|---|---|---|---|---|---|---|---|
| Traumatic history | |||||||
| Positive | 10 | 4 | 2.75 | 0.819-9. | 0.157+ | ||
| Negative | 60 | 66 | |||||
| Infectious disease history | |||||||
| Positive | 36 | 1 | 73.059 | 9.60-555.718 | 1 | 45.001 | 0.000* |
| Negative | 34 | 69 | |||||
| Pregnancies | |||||||
| First | 33 | 41 | 5 | 9.51 | 0.090* | ||
| Second | 19 | 21 | |||||
| Third | 12 | 5 | |||||
| Fourth | 5 | 1 | |||||
| Fifth | 0 | 2 | |||||
| Sixth | 1 | 0 | |||||
*Pearson’s chi-square test; + Fisher’s exact test.
Discussion
The psychomotor retardation approach includes a series of variables that need to be analyzed. Since motor alteration has a direct impact on the central nervous system, attention should not only focus on the musculoskeletal system but also on all of the aspects affected by the presentation.
Therefore, continuous follow-up in the postnatal stage is of vital importance. At the Hospital Sor María Ludovica in Argentina, in a follow-up of 140 apparently healthy infants from six to nine months of age, 22.5% were at risk of developmental delay, 13% of language delay, 3% of delayed motor skills, and 5% of coordination disorders 18.
According to the aforementioned, there are several sociodemographic factors that directly affect psychomotor development that are attributable to the presentation of the condition during the first months of life such as a lower social class. Within this section, among the factors associated with the presence of psychomotor retardation, detection is more readily seen in the infant population in Cuenca, Ecuador, which has twice the risk of presentation of the condition, frequently associated with microcephaly. The risk for the presence of this abnormality is 17 times higher and twice as prevalent in family groups with a non-nuclear structure 19.
It is evident that the presentation of the condition affects various tracts and systems, as well as life processes, combined with a 3.91 increase in the degree of malnutrition in infants who are suffering from the disease. Given the above, there is no doubt that various factors can influence the condition and improvement of the healthcare. However, the condition has not shown an affinity for a particular gender, according to the results obtained.
Maternal factors are related to the frequency of presentation and its impacts on the appropriate evolution. It is indisputable that sociodemographic and economic factors directly influence the rehabilitation of the patient. Leiva and Valdés emphasize that household income, as well as the educational level of the head of household had a significant impact on the presentation of psychomotor retardation in four and five-year-old school children from Talca, Chile. However, in a population from Robert Manuel Zulueta Calvo in Havana, an unsuitable socioeconomic level shows a five-fold increased risk of association with the disease 20,21.
Furthermore, late preterm infants are more predisposed to presenting hypoglycemia, jaundice, oculomotor alterations, as well as communication, fine motor, and social-individual skills disorders. With regard to the Ages & Stages Questionnaires scale used for the detection of neurodevelopmental disorders, the female group had a greater weight compared to the male group at the Severo Ochoa University Hospital in Leganés, Madrid 22.
According to the socioeconomic class applied to the study population by the Departamento de Trabajo Social in Tabasco, a significant relationship was found with a low socioeconomic status, while sex showed no affinity. As for the demographic factors, there is overcrowding and basic sanitation, but they showed no significant relationship. Compared to the results, the variables of location, piped water, and wall material showed no relationship either.
When carrying out the economic impact analysis, it is outstanding that it continues to focus on the presentation of the alterations, since the lower strata are an important focal point regarding the incidence of the condition. Therefore, urban areas are susceptible to various pathology presentations, for which a direct attribute cannot be presented.
In this regard, maternal factors that are directly related to the presentation of the case such as previous malnutrition during pregnancy, previous hypertension, and amniotic fluid problems can also be considered triggers of generalized developmental disorders such as Autism Spectrum Disorder and Asperger's Syndrome 23. Compared to the results obtained, the presence of illness during pregnancy is cited as a factor associated with psychomotor retardation with three times the risk of presentation in the infant and a traumatic accident has five times the risk of presentation. In addition to this, similarities in the presentation of results were found with maternal factors such as a history of contagious infectious diseases and a low IQ, as well as diseases during pregnancy, with regard to the presentations of infants with psychomotor development disorders 24-26.
Finally, all the aforementioned emphasizes the importance of investigating the causes that can be related with the presentation of the pathology, since the prognosis is related to the magnitude of the origin and the rehabilitation therapy to be carried out for each infant being of the utmost importance.
Various factors are related to the presence of psychomotor retardation in the newborn during his first months of life, such as a low social class. The presence of infections such as hyper-bilirubinemia, toxoplasmosis, and heart disease at a very early age in the newborn can lead to delayed psychomotor development compared to clinically healthy children. Therefore, within the recommendations, adequate prenatal within the first level of care remains to be a fundamental pillar of health care, as a frequent amount of cases in a family history shows a high relationship with the presentation of cases, as well as suffering from diseases during pregnancy or a history of trauma, which affects the incidence of the disease along with a late or torpid rehabilitation. In addition to this, nutrition and the importance of an adequate diet during pregnancy deserves a timely reference.
During the postnatal stage, intervention in the area of psychology regarding both familial processes and social coping strategies in which the affected patient will be involved are also important. Hearing and language, together with rehabilitation for the early correction of speech, mobility and strength, as well as family support during the process, must also be addressed.

