











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Knee osteoarthritis is a chronic, degenerative, and progressive pathology that primarily affects the joint cartilage of the knee and soft tissue structures, such as ligaments, muscles, tendons, and menisci 1. According to global data, the prevalence of knee osteoarthritis in people over 60 years of age is approximately 10 % in men and 13 % in women 2. Furthermore, approximately 80 % of individuals over 65 years of age present with radiographic changes at the knee level, compatible with knee osteoarthritis 3. In Latin American countries such as Cuba, the estimated rates are 17 %-19 % in the urban population, whereas in rural populations they are between 21 % and 23 % 4. With respect to incidence rates, in the United States, there are approximately 240 cases per 100,000 inhabitants each year 1. In Peru, according to reports from Seguro Social de Salud (Social Health Insurance) on the population under its health coverage, the incidence of knee osteoarthritis for the last five years is around 5.6 cases per year per 1000 inhabitants 5. At the primary care level, knee osteoarthritis accounts for 10 % of medical consultations, is the fourth and eighth leading cause of disability in women and men, respectively, and has an impact on global public health 6.
Osteoarthritis is a rheumatological condition that can affect different joints of the body, but the knee is particularly vulnerable due to the constant stress and use to which it is subjected 7. Therefore, patients may experience symptoms to varying degrees according to the particularities of their body and the presence of certain risk factors 8. The main symptoms in patients with knee osteoarthritis are pain of mechanical origin, which is chronic and has an insidious onset and progressive course; joint stiffness subsequent to long periods of immobility; and decreased functional capacity for daily activities 9,11. The decline of autonomy has a direct impact on an individual's quality of life and can have psychosocial effects, delaying the course of recovery 12.
Kinesiophobia, defined as a disproportionate fear of movement and physical activity, stems from the emotional and psychological profile of patients with knee osteoarthritis as a result of a sense of vulnerability due to a previous painful injury related to their background of beliefs, expectations, and experiences and represents a potential obstacle and possible element of pain chronification and disease perpetuation (disability) 13,14. Therefore, knee osteoarthritis, as a degenerative and chronic pathology, will deteriorate the patient's functionality in terms of routine tasks and progressive levels of pain and stiffness 15. The maintenance of these symptoms will affect the patient's psychological profile due to the impact on quality of life, possibly resulting in anxiety, depression, or kinesiophobia, which is intrinsically linked to their understanding of the negative implications of movement in their physical recovery 16. In this way, decreased activity due to fear of further injury or complications will paradoxically lead to further physical deconditioning, perpetuating symptoms, further limiting the individual's functional capacity and creating a vicious cycle in which clinical symptomatology is constantly and reciprocally related to the levels of kinesiophobia.
Few studies have addressed the relationship between the primary symptoms of patients with knee osteoarthritis and kinesiophobia and have shown inconsistent results in the different associations proposed; however, certain similarities have been noted (e.g., greater involvement of the female sex, implication of occupation and education). However, differences in the population, evolution of the disease, and social context have hindered agreement on the results and, thus, adequate understanding of the problematic reality, affecting the patient's rehabilitation 17,19. Therefore, this study aimed to determine the association among pain, stiffness, functional capacity, and kinesiophobia in patients with knee osteoarthritis at Hospital Nacional Hipolito Unanue in the city of Lima, Peru.
Materials and methods
e conducted an observational, correlational, and cross-sectional study. Patients with a diagnosis of knee osteoarthritis visiting the Department of Rehabilitation Medicine of Hospital Nacional Hipolito Unanue in the city of Lima (Peru) during the first two months of 2020 were included in this study. Initially, 99 patients were included. The inclusion criteria were as follows: (i) patients with a diagnosis of knee osteoarthritis, (ii) those undergoing physiotherapeutic treatment during the study period, and (iii) those who had signed the informed consent form. The exclusion criteria were as follows: (i) patients with surgical intervention on the knee or an adjacent area; (ii) those with a psychiatric or psychological history; (iii) those on analgesic, antidepressant, or anxiolytic medication; and (iv) those with peripheral vascular diseases diagnosed in the lower limbs. Based on the inclusion and exclusion criteria, the sample included 88 patients with knee osteoarthritis.
Sociodemographic and clinical variables, such as age, sex, current occupation, level of education, time of illness (in range categories), and affected lower limbs, were evaluated. For the evaluation of pain, stiffness, and functional capacity, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire was used. This instrument evaluates pain, stiffness, and functional capacity in patients with knee osteoarthritis through 5, 2, and 17 questions, respectively, with the following response options: none (0 points), mild (1 point), moderate (2 points), severe (3 points), and extreme (4 points) 20. From these numbers, specific ranges are obtained within each dimension of the questionnaire; for pain, the categories were mild (0-7 points), moderate (8-14 points), and severe (15-20 points); for stiffness, the categories were mild (0-2 points), moderate (3-5 points), and severe (6-8 points); and for functional capacity, the categories were adequate (0-22 points), with difficulty (23^5 points), and with severe difficulty (46-68 points) 21. The WOMAC questionnaire was validated with a Spearman correlation coefficient of 0.77 (p < 0.004), a Cronbach's alpha value of 0.92, and a high test-retest reliability of 0.66 to 0.81 22,24.
The kinesiophobia variable was evaluated by the Tampa Kinesiophobia Scale (TSK-11) in its Spanish version. The questionnaire was composed of 11 questions that measured the fear of movement and physical activity due to injury in patients with chronic musculoskeletal pain. Each item had four response options: strongly disagree (1 point), disagree (2 points), agree (3 points), and strongly agree (4 points) 25. The final categories had a cutoff point of 35 and were defined as low kinesiophobia (11-34 points) and high kinesiophobia (35-44 points) 14. This scale has Cronbach's alpha values in the range of 0.7-0.9, indicating acceptable/excellent internal consistency, high test-retest reliability with an intraclass correlation coefficient of >0.7, and a predictive validity range of moderate to good 26.
The Statistical Package for the Social Sciences (SPSS), version 26.0, software was used for the statistical analysis of the study. Therefore, the sociodemographic and clinical variables of age, sex, current occupation, time of illness, education level, and affected lower limbs were presented as frequencies and percentages for qualitative variables and as mean and standard deviation for quantitative variables. Likewise, frequency and percentage were used to present, in a descriptive way, the primary variables of pain, stiffness, functional capacity, and kinesiophobia. In the bivariate analysis, the nonparametric Pearson's chi-square test was used to determine the association between pain, stiffness, functional capacity, and kinesiophobia, considering a p value of <0.01. In addition, prior to selecting this statistic, the normality curves for the study variables were evaluated using the Kolmogorov-Smirnov test.
At all stages of the research, the ethical principles of the Declaration of Helsinki of the World Medical Association were considered, as well as respect for patients' dignity and confidentiality. They were informed of the purpose, risks, and benefits of the study, and their participation was requested by means of signing the informed consent form. The research was evaluated and approved by the Research Ethics Committee of Hospital Nacional Hipolito Unanue.
Results
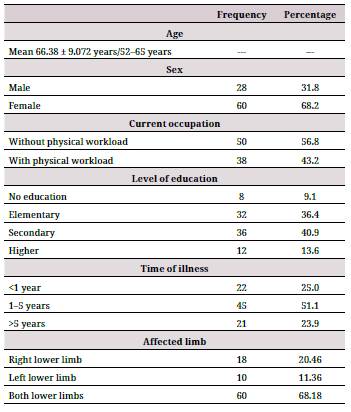
Regarding patients' sociodemographic and clinical characteristics, the mean age was 66.38 years (±9.072), with a range of 52-65 years. Of the patients, 68.2 % were female, 56.8 % had a current occupation without physical workload, 40.9 % had a secondary level education, 51.1 % reported a time of illness of 1-5 years, and 68.8 % presented with both lower limbs affected by knee osteoarthritis (Table 1).
Table 1 Sociodemographic and clinical characteristics in patients with knee osteoarthritis at Hospital Nacional Hipolito Unanue, Peru.
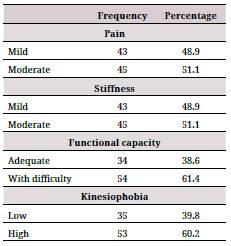
On the other hand, regarding the primary variables (Table 2), 51.1 °% of the evaluated patients presented with moderate pain, 51.1 °% with moderate joint stiffness, 61.4 °% with functional capacity difficulty, and 60.2 °% with a high level of kinesiophobia.
Table 2 Pain, stiffness, functional capacity, and kinesiophobia in patients with knee osteoarthritis at Hospital Nacional Hipolito Unanue, Peru.
For the analysis of the association between pain, stiffness, and functional capacity along with kinesiophobia in patients with knee osteoarthritis, a p value of <0.01 was obtained using Pearson's chi-square test. In addition, higher rates of high kinesiophobia were found in levels of moderate pain, moderate stiffness, and functional capacity with difficulty (Table 3).
Table 3 Association between pain, stiffness, functional capacity, and kinesiophobia in patients with knee osteoarthritis at Hospital Nacional Hipolito Unanue, Peru.
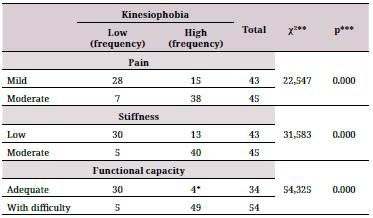
*Correction with Fisher's exact test.
**Pearson's chi-square value.
***p < 0.01.
Discussion
Knee osteoarthritis is one of the most common rheumatologic pathologies worldwide, especially in individuals over 60 years of age (older adults) 2,5. From the physical aspect, osteoarthritis of the knee manifests itself through three fundamental symptoms: pain, stiffness, and functional capacity difficulty, which can show a diverse gradation according to the characteristics of the pathology, the patient, and the associated concomitant conditions 8. However, due to the chronic characteristics of knee osteoarthritis, patients' psychological and emotional aspects are often involved, leading to the development of kinesiophobia, or fear of movement, which is a psychosocial condition that is linked to negative experiences of pain and health status perception. The patient's physical-functional part leads to psychosocial involvement, resulting in the emergence of kinesiophobia. In addition, the development of kinesiophobia causes a chronification of the symptoms and a limitation in recovery, resulting in a reciprocal (circular) relationship between the physical and psychosocial dimensions 13,15.
The sociodemographic and clinical characteristics of the patients who participated in the study showed a mean age of 66.38 years, with a higher prevalence of the female sex. Similarly, the findings revealed that a higher percentage of patients had a secondary level of education, over 50 % had a current occupation with no physical workload, a time of illness of 1-5 years, and bilateral involvement of the lower limbs due to knee osteoarthritis. These results are similar to studies in which the average age was between 63.6 and 68.96 years and in which the female sex was predominant 19,27. In one of the studies, a primary education level predominated 27, and in another, a secondary level education was attained similar to our research. In addition, bilateral lower limb involvement and the time of illness were also similar to our results 19,27.
In terms of the clinical variables associated with knee osteoarthritis, our study reported a moderate degree of pain with percentages >50 %. These findings differ from those obtained previously in another related study, where the degree of mild pain was more frequent, possibly because the patients assessed were younger (from the age of 30), indicating the presence of mild symptomatology 21. However, our data coincide with two other preliminary studies that were also performed in patients with knee osteoarthritis, in which the group with a moderate degree of pain was the one with the highest percentage 28,30.
On the other hand, moderate stiffness had a percentage of >50 % in our study, which was similar to that determined by previous studies where moderate joint stiffness was most common, but different from another where mild stiffness had a higher percentage 21,29,30. This is also explained by the difference in the age ranges of the assessed population, assuming that sensations of stiffness have less impact at younger ages.
Functional capacity with difficulty had a percentage of >60 % of the total subjects evaluated in this study. These data are similar to those found in previous studies also performed in the population with knee osteoarthritis in which degrees of functional capacity with difficulty or a corresponding moderate difficulty in the main activities of daily living were indicated 21,29,30. Regarding the psychosocial variable kinesiophobia, in our study, the high level had a percentage of >60 %, which is similar to studies where kinesiophobia was evaluated in populations with knee osteoarthritis or joint cartilage defects of the knee, where high levels were also most common 17,28.
According to the main objective of the study, an association was observed among moderate pain, moderate stiffness, difficulty in functional capacity, and high kinesiophobia. These results coincide with those obtained in previous studies where higher levels of pain were associated with higher degrees of kinesiophobia in patients with knee osteoarthritis 17,18,31. On the other hand, patients' functional capacity or physical function was also associated with kinesiophobia in one of these studies; however, the same was not applicable to stiffness, possibly due to its transient nature, unlike the other two symptoms 17.
There are several limitations of this study. Firstly, the patients included were both old and new to the service; thus, symptomatology may have decreased in the former due to physiotherapeutic intervention as opposed to the latter. This would explain the absence of severe cases observed for the main clinical variables, especially when we consider that patients continued to perform their personal and work activities, although at a reduced workload, regardless of the symptomatology. Secondly, a lack of clarity in some TSK-11 statements may have raised doubts among participants. Therefore, the research staff was always close to the respondents in order to answer their questions.
This study allowed us to determine that pain, stiffness, and functional capacity are associated with kinesiophobia in patients with knee osteoarthritis, which indicates that the degree of pain, stiffness, and deterioration of physical capacity increases with the increasing level of kinesiophobia. This information becomes relevant for future studies addressing the correlational analysis between the physical and psychosocial aspects of patients with chronic degenerative pathologies, such as knee osteoarthritis, both for the theoretical understanding of the phenomenon and for its implementation in healthcare practice.

