










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAvances en Psicología Latinoamericana
versão impressa ISSN 1794-4724versão On-line ISSN 2145-4515
Av. Psicol. Latinoam. v.26 n.1 Bogotá jan./jun. 2008
Is maternal deprivation the root of all evil?
David R. Cross*
Karyn B. Purvis*
* Texas Christian University, U. S. A. Address Correspondence to: David R. Cross, Ph.D. Department of Psychology, Texas Christian University. TCU Box 298920, Fort Worth, TX 76129, USA. E-mail: d.cross@tcu.edu.
Fecha de recepción: septiembre de 2007
Fecha de aceptación: marzo de 2008
Abstract
In this paper we seriously entertain the question, Is maternal deprivation the root of all evil? Our consideration of this question is broken down into three parts. In the first part, we discuss the nature of evil, focusing in particular on the legal concept of depravity. In the second part, we discuss the nurture of evil, focusing in particular on the common developmental trajectory seen in those who are depraved. In the third part, we discuss the roots of evil, focusing in particular on the animal and human research regarding maternal deprivation. Our conclusion is that maternal deprivation may actually be the root of all evil, but only because depraved individuals have been deprived of normative maternal care, which is the cradle of our humanity.
Key words: maternal deprivation, evil, depravity, development, parenting.
Resumen
En este artículo se aborda seriamente la pregunta ¿es la privación materna la raíz de toda la maldad? Nuestra consideración sobre esta cuestión se divide en tres partes. En la primera parte, discutimos la naturaleza de la maldad, enfocándonos en particular sobre el concepto de depravación. En la segunda parte, discutimos la crianza de la maldad, enfocándonos en particular sobre la trayectoria evolutiva común vista en aquellos que son depravados. En la tercera parte, discutimos la raíz de la maldad, enfocándonos en particular sobre la investigacion animal y humana sobre la privación materna. Nuestra conclusión es que la privación materna puede ser realmente la raíz de todos los males, pero sólo cuando los individuos depravados han sido privados del cuidado maternal normativo, el cual es la cuna de nuestra humanidad.
Palabras clave: privación materna, maldad, depravación, desarrollo, crianza de los hijos.
In this article we seriously consider the proposition that maternal deprivation is the root of all kinds of evil. This proposition is an obvious paraphrase of Pauls well-known, but often misquoted, admonition to Timothy: For the love of money is the root of all kinds of evil (Timothy 6:10). We will argue that as a practical matter, there may have been much truth in Pauls advice to Timothy about the perils of money, but as a scientific matter, Paul may have been wide of the mark. In contrast, the Ten Commandments serve as an uncannily accurate preview of the arguments we will be making in this paper (Exodus 20:1-17, paraphrased):
You shall have no other gods before me.
You shall not worship false idols.
You shall not misuse the name of the Lord.
Remember the Sabbath day by keeping it holy.
Honor your father and mother, so that you may live long in the land.
You shall not murder.
You shall not commit adultery.
You shall not steal.
You shall not lie.
You shall not covet your neighbors possessions, or his people.
We will have several opportunities to refer back to the Ten Commandments as we progress through our arguments. For now, we would like to highlight several features of this early guide to moral conduct. First, the first four commandments prescribe appropriate modes of worship, and reflect major concerns of the fledgling church. Second, the fifth commandment tells us to honor our parents, as we honor God—thus the first five commandments dictate that we are servants to a higher good (this reminds us of Gale Sayers, 2001, immortal saying, The Lord is first, my friends are second, and I am third.). Third, the remaining five commandments (which perhaps may be seen as following, developmentally, from the first five) are prescriptions for moral, humane behavior. The final point regarding the Ten Commandments is that of the last five commandments, the first four are behavioral, whereas the last is cognitive—it is not enough to act well, one should also think well.
Returning to the central proposition of this article, you will notice that it contains three core concepts: maternal deprivation, root, and evil. We will address these one at a time, in reverse order. In this way we will investigate the truth value of this proposition, based on the best scientific evidence available.
Depraved behavior: The nature of evil
Evil is a complex and multifaceted concept. The American Heritage Dictionary of the English Language offers the following definition of evil:
adj.
- Morally bad or wrong; wicked: an evil tyrant.
- Causing ruin, injury, or pain; harmful: the evil effects of a poor diet.
- Characterized by or indicating future misfortune; ominous: evil omens.
- Bad or blameworthy by report; infamous: an evil reputation.
- Characterized by anger or spite; malicious: an evil temper.
noun.
- The quality of being morally bad or wrong; wickedness.
- That which causes harm, misfortune, or destruction: a leader's power to do both good and evil.
- An evil force, power, or personification.
- Something that is a cause or source of suffering, injury, or destruction: the social evils of poverty and injustice.
As this definition makes clear, evil can refer to evil acts (e.g., breaches of the Ten Commandments), evil persons (those whom break the commandments), evil characteristics of persons (violent or covetous), supernatural forces that are evil (Satan), or natural forces that are evil (money). Like common psychological constructs such as learning, intelligence, and creativity, evil is clearly a complex and challenging concept. Further, evil is a concept that is not often discussed in scientific circles. A PsychINFO search yielded just 279 hits for evil (in the title), as compared to 7269 hits for aggression and 8380 hits for violence. Andrew Delbanco (1995) in his book The death of Satan argues that the concept of evil is dying out in America and that perhaps, as a consequence, we have become more tolerant of evil in our midst. He further argues that evil is increasingly visible (e.g., on the evening news and in the theater), is increasingly prevalent (e.g., mass murders, crimes of humanity), and yet we have lost a vocabulary for talking about it. Due to the disinterest of science and the secularization of religious institutions, our explanations for evil—both scientific and popular—may never have been weaker.
Nevertheless evil is a concept that may have some value, even in scientific discourse, for it seems to encode a level of depravity that is missing in such terms as violence and aggression. Although evil may be difficult to define, it appears to be something that we know when we see it:
To know evil, you have only to stand on the road in Jasper, Texas, where on June 7, 1998, three white men offered a ride to a 49-year-old black man, James Byrd Jr., who was on his way home from an anniversary party. Instead of taking him where he wanted to go, they beat, kicked, and tortured him merely for the color of his skin, and then spray-painted his face black before chaining him by the ankles to the back of their truck. As they sped down an isolated logging road, dragging him for nearly three miles, he tried keeping his head up, but his skin ripped off, his bones broke, and his elbows were shattered to the bone. When his head hit a culvert, it was ripped off, along with his right arm. What was left of his torso was dumped in front of a church for its black congregation to find. In TNT's documentary, The faces of evil, Dr. Molefi Kete Asante of Temple University points out multiple circles still evident on the road, drawn there to mark 75 separate places where Byrds body parts were found. ‘On this road, Asante says quietly, ‘I am confronted with the immensity of the cruelty that can exist in the human heart (Ramsland, 2003, p. 1).
If we agree to call acts such as the torture, mutilation, and murder of James Byrd as evil, then evil would seem to come in several varieties, including the following. First, there is the hate crime, where one or more individuals brutally attack someone on the basis of religious or ethnic background (e.g., the murders of James Byrd in Jasper, Texas, and of Matthew Shepard in Laramie, Wyoming). Second, there is genocide, or crimes against humanity, where an organized group of individuals attacks another group, usually on the basis of religious or ethnic background (e.g., Osama bin Laden and El Qaeda, or Hitler and the Nazis). Third, there is mass murder, where one or more individuals attack a group, more or less at random (e.g., Charles Whitman at the University of Texas, or the Columbine shootings). Fourth, there is the serial killer, who commits a series of murders, usually in a gruesome manner (e.g., Jack the Ripper, Ted Bundy). Fifth, there is the parent who kills (e.g., Andrea Yates of Houston, or Susan Smith of South Carolina). And sixth, there are children who kill, often in pairs or small groups. Consider the following account of a child murderer, one of several written about by Dr. Katherine Ramsland in her excellent online article, Children who kill (Ramsland, 2003, p. 5):
May 21, 1998—Kipland Kinkel, 15, had just been expelled from school in Springfield, Oregon, for carrying a gun to class. He returned with a semiautomatic rifle and went into the cafeteria, where he started shooting. He killed one student and wounded eight others, one of whom later died, and he also caused a stampede that resulted in more injuries. He was disarmed and taken to the police station, where he withdrew a hidden knife. He claimed he wanted to die. Police officers who went to his home discovered that hed killed both of his parents and had booby-trapped the house with five homemade bombs—one of which he'd placed underneath his mothers corpse. His classmates had once dubbed him the student ‘most likely to start World War III.
What do the hate crimes, crimes against humanity, mass murders, serial killings, murders of children by parents, and murders by children, all have in common? They are pre-meditated acts of violence. These are not crimes of passion, or of instrumental aggression. These are acts of cold blooded murder, often accompanied by wanton cruelty. In other words, these are acts of evil. But what separates these evil deeds from other capital offenses, such as murder or manslaughter? According to the legal system, it is the depravity of the crime. If murder is premeditated, is accompanied by torture or maiming, is senseless or wanton, then it is considered depraved by the legal system, and warrants stiffer penalties, including the death penalty.
Michael Welner is a forensic psychiatrist who has begun a systematic study of depravity, arguing that depravity is an important factor in the conviction and sentencing of criminals, but is fuzzily defined and unsystematically applied in U.S. courts. He has developed The depravity scale (Welner, 1998; see also www.depravityscale.org) as a way of standardizing and clarifying the construct of depravity. Welner essentially takes a behavioral approach to defining and measuring depravity, arguing that we should look at what the killer actually says and does, before, during, and after the crime, rather than placing our faith solely on hard evidence and traditional psychological examinations. Welners depravity scale has three subscales—intent, action, and attritudes:
The evidence establishing depraved intent includes the following behaviors:
- Intent to emotionally traumatize the victim (e.g., an intruder who attempts to destroy objects of greatest personal meaning).
- Intent to maximize damage (e.g., a terrorist who says We figured the best time to put the nerve gas on the train was during rush hour.).
- Intent to permanently disfigure (e.g., a stalker whose attacks focus on the face or sexual organs, as with a caustic substance).
- Influencing depravity in others to avoid prosecution or penalty (e.g., hiring a contract killer).
- Influencing depravity in others to overcome personal limitations (e.g., teenage girls who kill, typically recruit male accomplices to actually perform the act).
The evidence establishing depraved actions includes the following behaviors:
- Prolonging a victims suffering (e.g., The child was found with cigarette burns on her genitalia, and cord burns around her wrists.).
- Unrelenting physical and emotional harm (e.g., The child was dirty, malnourished, and found with numerous fractures, both new and old.).
- Degree of physical harm (e.g., The victim was beaten so badly he could not be recognized, and lay in intensive care for eight weeks.).
- Quality of the victims suffering (e.g., The victim was left in the desert, begging for his life.).
The evidence establishing depraved attitudes includes the following:
- Perpetrator shows response of indifference, satisfaction, or satiety to depravity (e.g., defendant brags about the offense: Sometimes you just gotta take out the trash.).
- Falsely accusing others of depraved actions, deliberately exposing the innocent to penalty (e.g., I didnt do it, but I will give you the name of the person who did.).
- Perpetrator projects responsibility for depravity onto the victim; perpetrator projects a sense of entitlement (e.g., I didnt rape her, she wanted it, or They deserved to die, they were stupid.).
Welner, who has collected over 4,000 responses to his scale, is still in the process of validating The depravity scale. But thus far he has found impressive consistency in respondents perceptions of depravity, and it appears that there is substantial agreement within the United States about what constitutes a depraved criminal act. In this article we argue that depravity is the essential ingredient for evil, and that Welner may have taken some of the first steps in placing the study of evil on a firm scientific foundation.
Pathways to depravity: The nurture of evil
Violent crime is a big problem in the United States, a statement that should surprise almost no one. According to Garbarino (1999), there are approximately 23,000 homicides committed in the United States annually, and of the killers, 10% (2,300) are under age 18. Coincidentally, approximately 2,300 children kill themselves each year in the United States. These numbers amount to about two or three large high schools being lost to violent crimes by youths each year—a staggering number. As bad as these numbers are, the actual problem is far worse. Garbarino (1999) argues that homicide and suicide rates actually underestimate the incidence of violent crime. There are a number of reasons why this is true. One reason is improved care provided by trauma units. Garbarino reports that in Chicago, serious (life-threatening) assaults increased by 400% from the 1970s to the 1990s, but the homicide rate stayed the same—this due to improved treatment by trauma services. Further, overall homicide rates—which are leveling off—are affected by demographic trends such as the percentage of youth in the overall population, which is decreasing. All of this is to say there is an epidemic of deadly youth violence in the United States, and quite understandably, lots of people want to know why.
We believe that the best answer to the question of why children kill is essentially a developmental one. In other words, if we are to understand the causes of youth violence, we are going to have to look closely at the developmental histories of children who commit violent acts. There is nothing new about looking to childhood experiences for causes of violence (see, for example, Garbarino, 1999; Karr-Morse & Wiley, 1997; Lavin & Park, 1999). What is new in this paper is that we provide a comprehensive summary of the evidence—more comprehensive we believe than any other review to date—and also introduce a new perspective on the ontogenetic origins of depravity, namely, what is known from animal and human research about the long-term effects of maternal deprivation.
The essential elements of our summary are diagrammed in Figure 1. Figure 1 charts the cascade of developmental events leading from early parent-child interactions during infancy to the commission of violent crimes during adolescence. There is good empirical evidence supporting all components of the model, although the evidence is stronger in some places in others. Nevertheless, even this model, while impressively comprehensive, is incomplete. For example, Figure 1 does not include prenatal influences (see, for example, Karr-Morse & Wiley, 1997), but instead begins postnatally. Further, the chart is truncated at the other end, and does not include adulthood. There are several reasons for these choices, including brevity, but the overarching reasons are (a) we wish to focus on the nurture of evil, and (b) childhood is not only where we find the root causes, but also the early manifestations of depraved behavior.
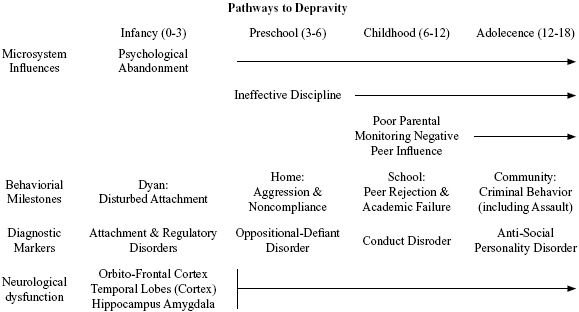
Figure 1. The developmental pathways to depravity during childhood, highlighted by microsystem infl uences,
behavioral milestones, diagnostic markers, and neurological dysfunction (Source: authors).
The first row in Figure 1 identifies major landmarks in the nurture of children who become violent. We have deliberately labeled this row Microsystem Influences (see Bronfenbrenner, 1992, 1999) to emphasize the systemic nature childrens developmental histories. A simplified view of Bronfenbrenners ecological systems model is presented in Figure 2. The core system in this model is the microsystem, which is a particular social context in which the developing child participates. Of course, the first and most important microsystem is the family, which includes parents, siblings, and perhaps extended family members. Microsystems are characterized by several social-developmental features, including settings, roles, and activities. As microsystems, families typically exist within certain settings (homes), while family members are prescribed different roles (parent vs. child), and engage in setting-appropriate activities (e.g., feeding, nurturing). Microsystems are the building blocks for larger, more complex systems relevant to the developing child. The mesosystem is the set of all microsystems within which the child participates (e.g., home, school, neighborhood peer group). An important feature of ecological systems theory is that it emphasizes the connections and consistencies among these microsystems of the developing child, a feature that is instantiated practically by multisystemic therapy (see the multisystemic therapy website for a complete list of references: http://www.mstservices.com/). The exosystem is the set of all microsystems which impact the developing child directly, but within which the child does not participate. Common examples are parents workplaces and settings where parents socialize or worship. The importance of the exosystem lies in the fact that practices (e.g., child care policies) and events (e.g., layoffs) occurring within the childs exosystem can have dramatic effects on the childs developmental trajectory. The macrosystem refers to the set of beliefs, practices, laws, and values that characterize the broader culture or society within which the child and family develop. These macrosystem-level phenomena (determining, for example, accessibility to quality child care) permeate the developing childs exosystem and mesosystem experiences, thereby shaping and directing the childs developmental trajectories. The chronosystem (Bronfenbrenner, 1986) is the final component of Bronfenbrenners model, and refers to changes occuring in the ecology of the child as he or she develops. Some of these changes may be driven by forces external to the family (e.g., changes in child welfare policy), some may be driven by structural or other changes occurring within the family (e.g., divorce, death of a parent, birth of a sibling), and some are driven by developing persons within the childs mesosystem, including the child. For example, when children reach the age of two or three, becoming more mobile and independent, parents are faced with a new set of challenges in terms of discipline. To take another example, as children develop they typically branch out beyond the home into multiple microsystems (i.e., home, school, peer group), in other words, their mesosystems expand.
It is a well-documented fact that the parents of violent children are notoriously poor at fulfilling the normative roles associated with the microsystem of the home. During infancy, the major factor appears to be parental abandonment (Garbarino, 1999). Although abuse at the hands of parents receives the most attention, developmental psychologists are coming to believe that neglect is at least as harmful (Cicchetti & Carlson, 1989; Cicchetti & Toth, 1995; Pollak, Cicchetti, Hornung & Reed, 2000). Further, the situation in many high-risk homes is tantamount to abandonment, where the needs of the developing infant are barely met, and abuse is mixed with neglect and a general failure to fulfill the roles and obligations of parenthood. Thus, it is often the case that even though parents may not physically abandon their offspring, their failure to parent is in effect a form of psychological abandonment.
As might be expected, maltreated infants are at high-risk for disturbances of attachment (Carlson, Cicchetti, Barnett & Braunwald, 1989; Egeland & Sroufe, 1981). Infants raised in these high-risk situations are more likely to develop insecure or disorganized attachments, and these disturbances of attachment may then become independent risk factors contributing to poor developmental trajectories later during the preschool years and childhood (Greenberg, 1999; Lyons-Ruth & Jacobvitz, 1999). The same breakdowns in caretaking that disturb the development of attachment are likely to disturb other important socio-emotional processes, such as the young childs ability to regulate affective and sensorimotor responses (Calkins & Fox, 2002; Greenspan, 1992; Schore, 1994). These physiological and behavioral processes are associated with what we call the OTHA Complex, which refers to a set of cortical and limbic structures including the orbito-frontal cortex, medial temporal lobes, hippocampus, and amygdala (Schore, 1994; Siegel, 1999). As we shall see, the OTHA complex is implicated in studies of depraved behavior (e.g., violent criminals), as well as in studies of maternal deprivation (e.g., institutionally-reared children).
This brief summary of developmental outcomes associated with early parental abandonment is contained within the first column of Figure 1 (Infancy). Many of the post-infancy components of the Figure 1 have been researched by Gerald Patterson and his colleagues at the Oregon Learning Center (Patterson, 1986; Patterson, DeBaryshe & Ramsey, 1989; Reid, Patterson & Snyder, 2002). Patterson and his colleagues have systematically developed and tested a developmental model of antisocial behavior in boys. According to the Oregon model, the developing child poses a series of challenges to parents, challenges for which some parents are ill prepared. The first of these challenges is presented by the preschooler, whose normal strivings for independence are met with ineffective and harsh discipline. This aggressive and poorly socialized preschooler is poorly prepared for the transition to school, where he faces rejection by normally developing peers, and academic failure. The challenges to parents escalate during childhood, as boys in particular become increasingly independent, aggressive, and connected to a deviant peer group. Interactional patterns within the family become increasingly aversive over time, and these maladaptive patterns themselves are supportive of pathological processes both within individual family members and within the family system (Patterson, 1980; Patterson & Banks, 1989). The net result is a pathway that leads from early interactional and parenting failures to adolescents that are aggressive, antisocial, and prone to criminal activity (Garbarino, 1999; Karr-Morse & Wiley, 1997).
Operating in parallel to these microsystem influences and developmental behavioral milestones are a series of diagnostic classifications that run from attachment and regulatory disorders during infancy to anti-social personality disorder during adolescence and adulthood (Black, 1999; Frick, 1998; Lahey & Loeber, 1994; Loeber et al, 1992). These diagnostic markers are summarized in the third row of Figure 1, and represent a developmental sequence of increasingly serious psychopathological conditions. This sequence is characterized by the fact that although each diagnostic marker (e.g., oppositional defiant disorder) may be followed by the next diagnostic marker in the sequence (e.g., conduct disorder), adolescents who are classified with the later-onset markers (i.e., antisocial personality disorder) almost certainly have progressed through the early markers in the sequence. According to Frick (1998, pp. 15-16):
[T]here seems to be a clear hierarchical pattern to the behavioral progression. Whereas few boys start showing the more severe antisocial and aggressive behaviors without first showing the less severe oppositional behaviors at earlier ages, a large proportion of children with less severe oppositional behaviors do not progress on to the more serious antisocial behaviors. To illustrate this hierarchical pattern, a 4-year longitudinal study of clinic-referred boys (initially aged 6-13) found that 82% of the boys who developed a serious conduct disorder in the third and fourth years of the study had shown less serious oppositional behaviors in prior years (Hinshaw et al., 1993; Lahey & Loeber, 1994). In contrast, only about half (47%) of the boys who showed oppositional behaviors in the first year of the study progressed on to the more severe antisocial and aggressive behaviors over the 4-year course of the study.
This asymmetry between forward-looking and backward-looking probabilities appears to apply to the entire sequence shown in Figure 1, going all the way from attachment disorder infancy to adulthood criminality (Greenberg, 1999; Heckel & Shumaker, 2001). We have represented the asymmetry of these developmental pathways in Figure 3, which shows the sequence of diagnostic markers as a series of concentric circles (which are not drawn to scale). The figure is designed to show how, for example, only some of the children classified with attachment disorder will go on to be classified with oppositional defiant disorder. On the other hand, a very high percentage of those children classified with oppositional defiant disorder were earlier classified with attachment disorder. Whether or not a child remains on the pathway to depraved behavior is determined by a constellation of risk and resilience factors that characterize the developing childs ecological system (see Figure 2).
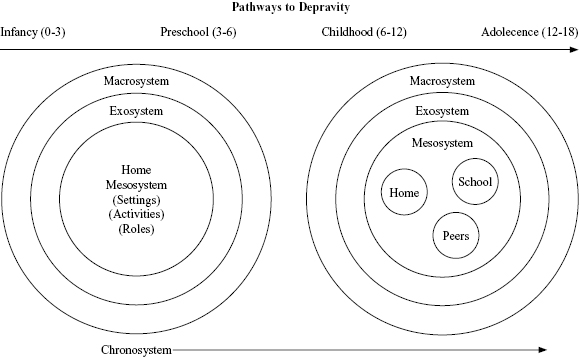
Figure 2. An ecological systems model for understanding childrens development in context (Bronfenbrenner, 1992, 1999) (Source: authors).
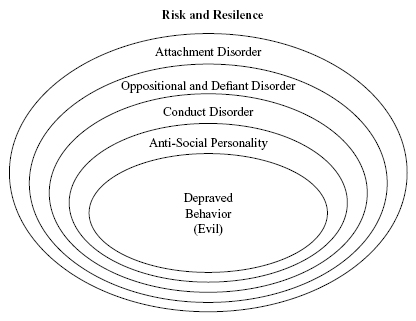
Figure 3. The prospective and retrospective pathways to and from depravity are asymmetrical: Virtually everyone who is classifi ed as anti-social personality (or engages in depraved behavior) has passed through all of the previous steps in the sequence; however, many of those who are classifi ed at earlier steps manage to avoid progressing to more serious classifications. (Source: authors).
Before going on to the next section it is worthwhile summarizing the major diagnostic features of the disorders listed in Figures 1 and 3. We will skip attachment and regulatory disorders, since they will be discussed more fully in the following section on maternal deprivation. According to the fourth edition of the Diagnostic and statistical manual of mental disorders (1994; see also Frick, 1999), oppositional defiant disorder (ODD) is characterized by a recurrent pattern of negativistic, defiant, disobedient, and hostile behavior towards authority figures. Symptoms of ODD include frequent loss of temper, frequent arguments with adults, refusals to comply with adults requests or rules, deliberately annoying other people, blaming others for his mistakes or behavior, is touchy or easily annoyed by others, and is often resentful or angry. Conduct disorder (CD) takes this pattern of oppositional behavior to next level, and is a disorder of later childhood and adolescence. CD is characterized by a repetitive and persistent pattern of behavior in which the basic rights of others or major age-appropriate societal norms are violated. Symptoms of CD include aggression to people or animals (e.g., bullying, fighting, use of weapons, cruelty to people and/or animals, forced sex), destruction of property (e.g., fire setting), deceitfulness or theft (e.g., breaking and entering, auto theft, stealing personal valuables), and serious violations of rules (e.g., staying out at night, running away, truancy). Importantly, there are two subtypes of CD, and childhood-onset type and an adolescent-onset type. The childhood-onset type is the one represented by the sequence shown in Figures 1 and 3 (Black, 1999; Frick, 1999). Finally, antisocial personality disorder (APD) is characterized by a pervasive pattern of disregard for and violation of the rights of others occurring since the age of 15 years, and is characterized by the following symptoms: Repeatedly engaging in acts that are grounds for arrest, repeated lying, use of aliases, or conning of others, impulsivity and failure to plan ahead, irritability and aggressiveness, leading to repeated fights and assaults, reckless disregard for the safety of others and oneself, irresponsible work behavior (e.g., cant hold jobs for long), and lack of remorse. In order to receive an APD diagnosis, individuals must be at least 18, and displayed of CD with onset before age 15.
These three diagnostic categories—ODD, CD, and APD—not only form a pathological developmental sequence, as has already been discussed, but their symptoms read like a systematic breaking of the Ten Commandments, one of mankinds most basic set of moral guidelines. Further, one can easily see in these symptoms either the outright depravity contained in Welners (1998) Depravity scale, or at least the seeds of this depravity. The point that we have attempted to make in this section is that a reasonable argument can be made for origins of such depravity (evil) in the developmental histories of those individuals who commit depraved actions. The problem with the evidence reviewed thus far is that the developmental pathway from early abandonment and maltreatment to later serious antisocial behavior is multi-determined, making it difficult to make causal inferences regarding the origins of depravity. However, there is a body of literature that is able to separate negative early experiences such as abuse and neglect, from ongoing risk factors that are present when children continue to be raised by the same parents, in the same neighborhoods, and with the same peer group. The body of literature that we refer is the research on maternal deprivation, which includes studies involving both animals and humans (studies of postinstitutionalized children raised by adoptive parents). This research points strongly to early experiences as having profound and long-term consequences for childrens development.
Maternal deprivation: The roots of evil
Children adopted from the foster care system or from institutions overseas are likely to have experienced a wide variety of risk factors (Johnson, 2000; Rutter, 1981; Yarrow, 1961). Almost by definition, children who are eligible for adoption have experienced the loss of their biological mother, either through death, abandonment, or separation. We will use the term maternal deprivation to refer to the wide range of possibilities here, including maternal privation—being deprived of maternal care from birth—and maternal deprivation—being separated from the biological mother after some period of maternal care (Ainsworth, 1962; Gandelman, 1992). In addition to maternal deprivation, children eligible for adoption, especially those with backgrounds of institutional care, may have experienced environmental deprivation (Gandelman, 1992; Gunnar, 2001). Some of these children, raised in the worst institutional settings imaginable, may have experienced not only maternal and environmental deprivation, but nutritional deprivation as well, leading to an early childhood experienced that could be characterized as global deprivation (Gunnar, 2001; Rutter et al, 1998). Furthermore, children adopted from foster care or institutional care settings may have experienced maltreatment, either at the hands of peers, family members, or by others assigned to their care (Johnson, 2000). Based on the presence of these risk factors, either singly or in combination, children adopted from foster care or institutional care would appear to be at serious risk for a variety of delays and disturbances of development.
A growing body of research has documented a wide range of developmental problems associated with environmental, maternal, and nutritional privation. Recently there have been several good reviews of the international adoption literature, which is a particularly rich source of information about the impact of early deprivation (Gunnar, 2001; Gunnar, Bruce & Grotevant, 2001; Johnson, 2000). Reviews of the existing evidence suggest that the consequences of early severe deprivation can be divided into two broad categories. The first category includes deficits that are very general in their nature, and show a striking tendency for catching up once children are placed in adoptive homes. Deficits in this category include physical growth, general intellectual performance, and language (Gunnar, 2001; Johnson, 2000; Mason & Narad, 2002; Rutter & the ERA Study Team, 1998). These findings suggest that there is a fairly wide window of opportunity for these general characteristics to develop.
However, there is another category of deficits that do not remit so easily after severely deprived children are placed in adoptive homes. These deficits are less global, and appear to be specific consequences of maternal deprivation (Ainsworth, 1962; Gunnar, 2001; Kraemer, 1992). If true, this is an important fact, for it means that adopted children with a wide range of backgrounds are susceptible to these socio-emotional deficits, because maternal deprivation, broadly defined as it is here, is by far the most common characteristic in the backgrounds of adopted children. The socio-emotional deficits commonly seen in adopted children manifest themselves in a variety of ways, including externalizing behavior problems (e.g., aggression), poor emotion regulation (especially with anger), poor inhibitory control, weak social cognition, and disordered attachments (Gunnar, 2001; Johnson, 2000). In the discussion that follows, we will divide these into three subcategories: attachment disorders, regulatory disorders, and behavior problems. Although these categories are often discussed as if they were independent aspects of the childs functioning, there is a growing understanding of the rich connections among them, based both on common developmental histories and underlying neuropsychological processes (Kraemer, 1992; Schore, 1994; Siegel, 1999).
Research on the connection between maternal deprivation and later attachment disturbances has a venerable tradition stretching back to the pioneering work of Bowlby (1951; 1969/1982, 1973, 1980) and Harlow (1958, 1971), among others. Research with postinstitutionalized children has documented that maternally deprived children are at risk for a range of attachment disturbances, ranging from the relatively mild to the severe (Federici, 1998; Gunnar, 2001; Zeanah, in press). As might be expected, postinstitutionalized (PI) children are at higher risk for insecure attachments, although this risk appears to be moderated by age at adoption (Chisholm, Carter, Ames, & Morison, 1995; Juffer & Rosenboom, 1997; Marcovitch et al., 1997). More troublesome is that children with backgrounds of maternal deprivation are at very high risk for disorders of attachment, especially disorders of nonattachment (Zeanah & Boris, 2000; Zeanah, Boris, Bakshi, & Lieberman, 2000), a finding that has been observed by at least three different research groups (Chisholm, 1998; OConnor, Bredenkamp & Rutter, 1994; Tizard & Rees, 1975). An important addendum to these findings is a substantial debate about nosologies for attachment disorders, with Zeanah and his colleagues (Zeanah, 1996; Lieberman & Zeanah, 1995; Zeanah & Boris, 2000) making a convincing case for developmentally-based alternatives to the official classification schemes found in the Diagnostic and statistical manual of mental disorders (1994) and the International classification of diseases (1992).
Children who suffer maternal deprivation will very often experience limited sensory input and have limited opportunities for transactional experiences with their social and physical environments (Gunnar, 2001; Johnson, 2000). Although not as well researched as are the attachment disturbances associated with maternal deprivation, sensory deficits have been documented in at least a few studies (Cermak & Danhauer, 1997; Cermak & Groza, 1998; Haradon, Bascom, Dragomir, & Scripcaru, 1994; see also Johnson, 2000). These sensory deficits are often conceptualized as sensory integration deficits, i.e. disturbances in the childs ability to process, integrate, and modulate sensory input (Ayers, 1979; Fisher & Murray, 1991; Kranowitz, 1998). In terms of clinical nosologies, sensory integration problems have been included in the Zero to Three (1994) classification of regulatory disorders (Barton & Robins, 2000). Originally proposed by Greenspan and colleagues (Greenspan, 1992; Greenspan & Weider, 1993), regulatory disorders include both sensory and emotional components, and indicate fundamental disturbances in the childs ability to organize activity and responsivity to environmental input (Barton & Robins, 2000; Stieben et al, 2007). There is a growing consensus among developmentalists that the ability to self-regulate in this way emerges from the matrix of caregiver-child interactions early in life (Hofer, 1994; Schore, 1994), so it is no surprise that maternally deprived children would exhibits deficiencies in this regard. In fact, neuropsychological research with post-institutionalized children has shown that key structures (OTHA in Figure 1, above) associated with self-regulation and processing of socio-emotional information are functionally depressed (Chugani, Behen, Muzik, Juhasz, Nagy, & Chugani, 2001). Further evidence for regulatory abnormalities comes from studies that have documented chronic abnormalities in neuroendocrinological functioning among samples of children with institutional backgrounds (Carlson & Earls, 1997; Gunnar, Morison, Chisholm, & Schuder, 2001).
As might be expected, given that foster-care and institutional-care children are at risk for disturbances in such foundational developmental arenas as attachment and self-regulation, these children are also at risk for behavior problems and poor peer relationships (Gunnar, 2001). Several research teams investigating the adjustment of children adopted from institutions have documented behavior problems that may arise after adoption (Fisher, Ames, Chisholm, & Savoie, 1997; Gunnar et al, 2007; Juffer & van Ijzendoorn, 2005; Rutter et al, 1998; Verhulst, Althaus, & Versluis-Den Bieman, 1990a, 1990b, 1992). These findings are congruent with studies of institutionalized children, such as those conducted by Tizard and her colleagues (Hodges & Tizard, 1989a, 1989b; Tizard & Hodges, 1978; Tizard & Rees, 1974). In general, what these studies show is that many maternally deprived children experience problems of an externalizing nature (i.e., control of anger and inappropriate aggression), and have difficulty forming friendships with peers. There are at least three avenues by which these problems may develop. First, institutionally- or foster-reared children may have been denied the opportunity to develop those self-regulatory processes associated with sensitive and responsive maternal care (Hofer, 1994; Schore, 1994), and which are now believed to be preventative of problematic childhood behaviors (Calkins & Fox, 2002; Dishion, French, & Patterson, 1995; Quay, 1993). Second, these children may have been denied the opportunity develop prosocial behaviors that ordinarily develop by virtue of normative socialization in the home environment (Grusec, Davidov, & Lundell, 2002; Eisenberg & Valiente, 2002). And third, maternally deprived children may have had the opportunity to learn behaviors that are considered antisocial (and hence maladaptive) by their adoptive families and by society at large, but that were adaptive in the ecologies where they lived and learned prior to being adopted. Johnson (2000) has, for example, described the maltreatment experienced by at least some institutionalized children, and whether the child was the victim or the instigator, these situations are opportunities for acquiring behaviors appropriate for that context.
Parental care: The cradle of humanity
The parallels between the profiles of psychologically abandoned children, as seen in the sequences displayed in Figures 1 and 3, and the profiles of adopted children with institutional backgrounds are striking. Of particular importance is the fact that the same neural structures (OTHA) show up repeatedly in studies of both normal and abnormal socio-emotional development (Chugani, et al., 2001; Schore, 1994). The associated behaviors are seen not only in the sequences leading up to severe antisocial behavior, but also in the studies of post-institutionalized children. The convergence of these findings strongly suggests that early experience, maternal deprivation in particular, is a causative factor in the formation of the antisocial personality. Keeping Figure 3 in mind, we can conclude, with some degree of certainty, that although not all maternally deprived (or psychological abandoned) individuals will become antisocial, virtually anyone who in fact becomes antisocial will have been maternally deprived. In this sense, then, we can conclude that maternal deprivation may actually be the root of all evil. But the converse is also true, maternal (or more generally, parental) care is the foundation for our humanity, that which makes us essentially human. For isnt it true that the monsters in our midst, those who are depraved, show us what is most important to being human by what they lack?
References
1. Ainsworth, M. D. The effects of maternal deprivation: A review of findings and controversy in the context of research strategy. In M. D. Ainsworth, R. G. Andry, R. G. Harlow, S. Lebovici, M. Mead, D. G. Prugh, & B. Wootton (Eds.), Deprivation and maternal care: A reassessment of its effects (pp. 97-159). Geneva, Switzerland: World Health Organization, (1962). [ Links ]
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, Fourth Edition. Washington, DC: Author, (1994). [ Links ]
3. Ayers, A. J. Sensory integration and the child. Los Angeles, CA: Western Psychological Services, (1979). [ Links ]
4. Barton, M. L., & Robins, D. Regulatory disorders. In C. H. Zeanah (Ed.), Handbook of infant mental health, Second Edition (pp. 311-325). New York: Guilford Press, (2000). [ Links ]
5. Black, D. W. Bad boys, bad men: Confronting antisocial personality disorder. New York: Oxford University Press, (1999). [ Links ]
6. Bowlby, J. Attachment and loss: Vol. 1: Attachment. New York: Basic Books, (1969/1982). [ Links ]
7. Bowlby, J. Attachment and loss: Vol. 2: Separation. New York: Basic Books, (1973). [ Links ]
8. Bowlby, J. Attachment and loss: Vol. 3: Loss. New York: Basic Books, (1980). [ Links ]
9. Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Developmental Psychology, 22, (1986), 723-742. [ Links ]
10. Bronfenbrenner, U. Ecological systems theory. In R. Vasta (Ed.), Six theories of child development: Revised formulations and current issues (pp. 187-249). London, UK: Jessica Kingsley Publishers, (1992). [ Links ]
11. Bronfenbrenner, U. Environments in developmental perspective: Theoretical and operational models. In S. L. Friedman & T. D. Wachs (Eds.), Measuring environment across the lifespan: Emerging methods and concepts (pp. 3-28). Washington, DC: American Psychological Association,(1999). [ Links ]
12. Calkins, S. D., & Fox, N. A. Self-regulatory processes in early personality development: A multilevel approach to the study of childhood social withdrawal and aggression. Development and Psychobiology, 14, (2002), 477-498. [ Links ]
13. Carlson, M., & Earls, F. Psychological and neuroendocrinological sequelae of early deprivation among institutionalized children in Romania. Annals of the New York Academy of Sciences, 807, (1997), 419-428. [ Links ]
14. Carlson, V., Cicchetti, D., Barnett, D., & Braunwald, K. A prospective longitudinal study of disorganized/disoriented attachment. Developmental Psychology, 25, (1989), 525-531. [ Links ]
15. Cermak, S. A., & Danhauer, L. A. Sensory processing in the post-institutionalized child. American Journal of Occupational Therapy, 51, (1997), 500-507. [ Links ]
16. Cermak, S. A., & Groza, V. Sensory processing problems in post-institutionalized children: Implications for social work. Child & Adolescent Social Work Journal, 15, (1998), 5-37. [ Links ]
17. Chisholm, K. A three-year follow-up of attachment and indiscriminate friendliness in children adopted from Romanian orphanages. Child Development, 69, (1998), 1092-1106. [ Links ]
18. Chisholm, K., Carter, M. C., Ames, E. W., Morison, S. J. Attachment security and indiscriminately friendly behavior in children adopted from Romanian orphanages. Development and Psychopathology, 7, (1995), 283-294. [ Links ]
19. Chugani, H. T., Behen, M. T., Muzik, O., Juhasz, C., Nagy, F., & Chugani, D. C. Local brain functional activity following early deprivation: A study of postinstitutionalized Romanian orphans. Neuroimage, 14, (2001), 1290-1301. [ Links ]
20. Cicchetti, D., & Carlson, V. (Eds.). Child maltreatment: Theory and research on the causes and consequences of child abuse and neglect. New York: Cambridge University Press, (1989). [ Links ]
21. Cicchetti, D., & Toth, S. L. A developmental psychopathology perspective on child abuse and neglect. Journal of the American Academy of Child & Adolescent Psychiatry, 34, (1995), 541-565. [ Links ]
22. Delbanco, A. The death of Satan. New York: Farrar, Strauss, Giroux, (1995). [ Links ]
23. Dishion, T. J., French, D. C., & Patterson, G. R. The development and ecology of antisocial behavior. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology. Vol. 2: Risk, disorder, and adaptation (pp. 421-471). New York: John Wiley & Sons, (1995). [ Links ]
24. Egeland, B., & Sroufe, L. A. Developmental sequelae of maltreatment in infancy. New directions for child development, No. 11 (pp. 77-92). San Francisco: Jossey-Bass, (1981). [ Links ]
25. Eisenberg, N., & Valiente, C. Parenting and children's prosocial and moral development. In M. H. Bornstein (Ed). Handbook of parenting: Vol. 5: Practical issues in parenting, Second Edition (pp. 111-142). Mahwah, NJ: Lawrence Erlbaum Associates, (2002). [ Links ]
26. Federici, R. S. Hope for the hopeless child: A guide for families. Alexandria, VA: Federici & Associates, (1998). [ Links ]
27. Fisher, A. G., & Murray, E. A. Introduction to sensory integration theory. In A. G. Fisher, E. A. Murray, & A. C. Bundy (Eds.). Sensory integration: Theory and practice (pp.3-24). Philadelphia: F. A. Davis, (1991). [ Links ]
28. Fisher, L., Ames, E. W., Chisholm, K., & Savoie, L. Problems reported by parents of Romanian orphans adopted to British Columbia. International Journal of Behavioral Development, 20, (1997), 67-82. [ Links ]
29. Frick, P. J. Conduct disorders and severe antisocial behavior. New York: Plenum Press, (1998). [ Links ]
30. Gandelman, R. The psychobiology of behavioral development. New York: Oxford University Press, (1992). [ Links ]
31. Garbarino, J. Lost boys: Why our sons turn violent and how we can save them. New York: Free Press, (1999). [ Links ]
32. Greenberg, M. T. Attachment and psychopathology in childhood. In J. Cassidy & P. R. Shaver (Eds.), Handbook of attachment: Theory, research, and clinical applications (pp. 469-496). New York: Guilford Press, (1999). [ Links ]
33. Greenspan, S. Regulatory disorders. Infancy and early childhood: The practice of clinical assessment and intervention with emotional and developmental challenges. Madison, CT: International Universities Press, (1992). [ Links ]
34. Greenspan, S., & Weider, S. Regulatory disorders. In C. H. Zeanah (Ed.), Handbook of infant mental health (pp. 280-290). New York: Guilford Press, (1993). [ Links ]
35. Grusec, J. E., Davidov, M., & Lundell, L. Prosocial and helping behavior. In P. K. Smith & C. H. Hart (Eds.). Blackwell handbook of childhood social development (pp. 457-474). Malden, MA: Blackwell Publishers, (2002). [ Links ]
36. Gunnar, M. R. Effects of early deprivation: Findings from orphanage-reared infants and children. In C. A. Nelson and M. Luciana (Eds.), Handbook of developmental cognitive neuroscience (pp. 617-629). Cambridge, MA: MIT Press, (2001). [ Links ]
37. Gunnar, M. R., Bruce, J., & Grotevant, H. International adoption of institutionally reared children: Research and policy. Development and Psychopathology, 12, (2000), 677-693. [ Links ]
38. Gunnar, M. R., Morison, S. J., Chisholm, K., & Schuder, M. Salivary cortisol levels in children adopted from Romanian orphanages. Development and Psychopathology, 7, (2001), 611-628. [ Links ]
39. Gunnar, M. R., Van Dulmen, M. H. M., & the International Adoption Project Team. Behavior problems in postinstitutionalized internationally adopted children. Development and Psychopathology, 19, (2007), 129-148. [ Links ]
40. Haradon, G., Bascom, B., Dragomir, C., & Scripcaru, V. Sensory functions of institutionalized Romanian infants: A pilot study. Occupational Therapy International, 1, (1994), 250-260. [ Links ]
41. Harlow, H. F. The nature of love. American Psychologist, 13, (1958), 673-685. [ Links ]
42. Harlow, H. F., Harlow, M. K., & Suomi, S. J. From thought to therapy: Lessons from a primate laboratory. American Scientist, 59, (1971), 538-549. [ Links ]
43. Heckel, R. V., & Shumaker, D. M. Children who murder: A psychological perspective. Westport, CN: Praeger, (2001). [ Links ]
44. Hofer, M. A. Hidden regulators in attachment, separation, and loss. In N. A. Fox (Ed.), The development of emotion regulation: Biological and behavioral considerations (pp. 192-207). Monographs of the Society for Research in Child Development, 59 (2-3, Serial No. 240), (1994). [ Links ]
45. Hodges, J., & Tizard, B. IQ and behavioural adjustment of ex-institutionalized adolescents. Journal of Child Psychology and Psychiatry, 30, (1989a), 53-75. [ Links ]
46. Hodges, J., & Tizard, B. Social and family relationships of ex-institutionalized adolescents. Journal of Child Psychology and Psychiatry, 30, (1989b), 77-97. [ Links ]
47. Johnson, D. E. Medical and developmental sequelae of early childhood institutionalization in Eastern European countries. In C. A. Nelson (Ed.), The effects of early adversity in neurobehavioral development. Minnesota Symposia on Child Psychology, 31, (2000), 113-162. [ Links ]
48. Juffer, F., & Rosenboom, L. G. Infant-mother attachment in internationally adopted children in the Netherlands. International Journal of Behavioral Development, 20, (1997), 93-107. [ Links ]
49. Juffer, F., & van Ijzendoorn, M. H. Behavior problems and mental health referrals of international adoptees: A meta-analysis. Journal of the American Medical Association, 293, (2005), 2501-2515. [ Links ]
50. Karr-Morse, R., & Wiley, M. S. Ghosts from the nursery: Tracing the roots of violence. New York: The Atlantic Monthly Press, (1997). [ Links ]
51. Kraemer, G. W. A psychobiological theory of attachment. Behavioral and Brain Sciences, 15, (1992), 493-541. [ Links ]
52. Kranowitz, C. S. The out-of-sync child. New York: Penguin Putnam, (1998). [ Links ]
53. Lahey, B. B., & Loeber, R. Framework for a developmental model of oppositional defiant disorder and conduct disorder. In D. K. Routh (Ed.), Disruptive behavior disorders in childhood (pp. 139-180). New York: Plenum, (1994). [ Links ]
54. Lavin, P., & Park, C. Despair turned into rage: Understanding and helping abused, neglected, and abandoned youth. Annapolis Junction, MD: Child Welfare League of America, (1999). [ Links ]
55. Loeber, R., Green, S. M., Lahey, B. B., Christ, M. A. G., & Frick, P. J. Developmental sequences in the age of onset of disruptive child behaviors. Journal of Child and Family Studies, 1, (1992), 21-41. [ Links ]
56. Lyons-Ruth, K., & Jacobvitz, D. Attachment disorganization: Unresolved loss, relational violence, and lapses in behavioral and attentional strategies. In J. Cassidy & P. R. Shaver (Eds.), Handbook of attachment: Theory, research, and clinical applications (pp. 520-554). New York: Guilford Press, (1999). [ Links ]
57. Marcovitch, S., Goldberg, S., Gold, A., Washington, J., Wasson, C., Krekewich, K., & Handley-Derry, M. Determinants of behavioural problems in Romanian children adopted in Ontario. International Journal of Behavioral Development, 20, (1997), 17-31. [ Links ]
58. Mason, P., & Narad, C. Growth and pubertal development in internationally adopted children. Current Opinion in Endocrinology & Diabetes, 9, (2002), 26-31. [ Links ]
59. OConnor, T. G., Bredenkamp, D., & Rutter, M. Attachment disturbances and disorders in children exposed to early severe deprivation. Infant Mental Health Journal, 20, (1994), 10-29. [ Links ]
60. Patterson, G. R. Mothers: The unacknowledged victims. Monographs of the Society for Research in Child Development, 45, No. 5, (1980). [ Links ]
61. Patterson, G. R. Performance models for antisocial boys. American Psychologist, 41, (1986), 432-444. [ Links ]
62. Patterson, G. R., & Bank, C. L. Some amplifying mechanisms for pathologic processes in families. In M. R. Gunnar & E. Thelen (Eds.), Systems and development. The Minnesota symposia on child psychology, Vol. 22 (pp. 167-209). Hillsdale, NJ: Lawrence Erlbaum Associates, (1989). [ Links ]
63. Patterson, G. R., DeBaryshe, B. D., & Ramsey, E. A developmental perspective on antisocial behavior. American Psychologist, 44, (1989), 329-335. [ Links ]
64. Pickett, J. P. (Ed.). American heritage dictionary of the English language, Fourth Edition. Boston, MA: Houghton Mifflin, (2000). [ Links ]
65. Pollak, S. D., Cicchetti, D., Hornung, K., & Reed, A. Recognizing emotion in faces: Developmental effects of child abuse and neglect. Developmental Psychology, 36, (2000), 679-688. [ Links ]
66. Quay, H. C. The psychobiology of undersocialized aggressive conduct disorder: A theoretical perspective. Development and Psychobiology, 5, (1993), 165-180. [ Links ]
67. Ramsland, K. Evil, Part One: Its Manifestations. Chapter 1: A Look at Evils Face. Court TVs Crime Library, (2003). Retrieved November 16, 2007, from www.crimelibrary.com/criminal_mind/psychology/evil1/1.html [ Links ]
68. Ramsland, K. School killers. Chapter 1: The List. Court TVs Crime Library, (2003). Retrieved November 16, 2007, from www.crimelibrary.com/serial_killers/weird/kids1/index_1.html [ Links ]
69. Reid, J. B., Patterson, G. R., & Snyder, J. Antisocial behavior in children and adolescents: A developmental analysis and model for intervention. Washington, DC: American Psychological Association, (2002). [ Links ]
70. Rutter, M. Maternal deprivation reassessed. New York: Penguin Books, (1981). [ Links ]
71. Rutter, M., & the English and Romanian Adoptees (ERA) Study Team. Developmental catchup and deficit, following adoption after severe global early deprivation. Journal of Child Psychology and Psychiatry, 39, (1998), 465-476. [ Links ]
72. Rutter, M., Andersen-Wood, L., Beckett, C., Bredenkamp, D., Castle, C., Grootheus, C., Kreppner, J., Keaveney, L., Lord, C., & OConnor, T. G. Quasi-autistic patterns following severe global privation. Journal of Child Psychology and Psychiatry, 40, (1999), 537-549. [ Links ]
73. Sayers, G., & Silverman, A. I am third (Reissue Edition). New York: Penguin, (2001). [ Links ]
74. Schore, A. N. Affect regulation and the development of self: The neurobiology of emotional development. Hillsdale, NJ: Lawrence Erlbaum Associates, (1994). [ Links ]
75. Siegel, D. J. The developing mind: Toward a neurobiology of interpersonal experience. New York: Guilford Press, (1999). [ Links ]
76. Stieben, J., Lewis, M. D., Granic, I., Zelazo, P. D., Segalowitz, S., & Pepler, D. Neurophysiological mechanisms of emotion regulation for subtypes of externalizing children. Development and Psychopathology, 19, (2007), 455-480. [ Links ]
77. Tizard, B., & Hodges, J. The effects of early institutional rearing on the development of eight-year-old children. Journal of Child Psychology and Psychiatry, 19, (1978), 99-118. [ Links ]
78. Tizard, B., & Rees, J. The effect of early institutional rearing on the behavior problems and affectional relationships of four-year-old children. Journal of Child Psychology and Psychiatry, 27, (1974), 61-73. [ Links ]
79. Tuckett, P. (Producer). Faces of evil. TNT Network, (1998). [ Links ]
80. United States Public Health Service. Report of the Surgeon Generals Conference on Childrens Mental Health: A National Action Agenda. Washington, DC: Department of Health and Human Services, (2000). [ Links ]
81. Verhulst, F., Althaus, M., & Versluis-Den Bieman, H. J. Problem behavior in international adoptees: I. An epidemiological study. Journal of the American Academy of Child and Adolescent Psychology, 29, (1990a), 94-103. [ Links ]
82. Verhulst, F., Althaus, M., & Versluis-Den Bieman, H. J. Problem behavior in international adoptees: II. Age at placement. Journal of the American Academy of Child and Adolescent Psychology, 29, (1990b), 104-111. [ Links ]
83. Verhulst, F., Althaus, M., & Versluis-Den Bieman, H. J. Damaging backgrounds: Later adjustment problems in international adoptees. Journal of the American Academy of Child and Adolescent Psychology, 31, (1992), 518-524. [ Links ]
84. Welner, M. Defining evil: A depravity scale for todays courts. The Forensic Echo, 2, (1998), 4-14. [ Links ]
85. World Health Organization. The ICD-10 classification of mental and behavioral disorders: Clinical descriptions and diagnostic guidelines. Geneva, Switzerland: Author, (1992). [ Links ]
86. Yarrow, L. J. Maternal deprivation: Toward an empirical and conceptual re-evaluation. Psychological Bulletin, 58, (1961), 459-490. [ Links ]
87. Zeanah, C. H. Disturbances of attachment in young children adopted from institutions. Journal of Developmental and Behavioral Pediatrics, 21, (2000), 230-236. [ Links ]
88. Zeanah, C. H. Beyond insecurity: A reconceptualization of attachment disorders of infancy. Journal of Consulting and Clinical Psychology, 64, (1996), 42-52. [ Links ]
89. Zeanah, C. H., & Boris, N. W. Disturbances and disorders of attachment in early childhood. In C. H. Zeanah (Ed.), Handbook of infant mental health, Second Edition (pp. 353-368). New York: Guilford Press, (2000). [ Links ]
90. Zeanah, C. H., Boris, N. W., Bakshi, S., & Lieberman, A. Disorders of attachment. In J. Osofsky & H. Fitzgerald (Eds.), WAIMH handbook of infant mental health (pp. 93-122). New York: Wiley, (2000). [ Links ]

