










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkCES Medicina Veterinaria y Zootecnia
On-line version ISSN 1900-9607
Ces. Med. Vet. Zootec. vol.9 no.2 Medellín July/Dec. 2014
First report of canine borreliosis seroprevalence in a middle-altitude tropical urban area (Medellín-Colombia)¤
Primer reporte de seroprevalencia de borreliosis canina en una ciudad localizada en una altitud media en la región tropical (Medellín, Colombia)
Primeiro relato de soroprevalência de borreliose canina em uma cidade localizada a uma altitude média na região tropical (Medellín, Colombia)
María S. González-Domínguez1, MV, MSc; Juan Pablo Villegas1, MV, MSc; Sara Carmona1, MVZ, cMSc; Hernán Castañeda 1, MVZ.
¤To cite this article: Gonzalez-Dominguez MS, Villegas JP, Carmona S, Castañeda H. First report of canine borreliosis seroprevalence in a middle-altitude tropical urban area (Medellín-Colombia). Rev CES Med Zootec. 2014; Vol 9(2): 348-354.
* Corresponding autor at: Universidad CES. Calle 10 A # 22- 04.Tel. 4440555 Ext 1550. Medellín, Antioquia, Colombia.
E-mail: mgonzalez@ces.edu.co (María S. Gonzalez-Dominguez).
1 Grupo de investigación INCA-CES, Facultad de Medicina Veterinaria y Zootecnia, Universidad CES. Medellín, Colombia.
(Recibido: 29 de agosto, 2014; aceptado: 19 de noviembre, 2014)
Abstract
Anamnesis: A one year old French Bulldog male, affected by gastrointestinal symptoms and abdominal pain, with no response to the established therapeutic schedule was attended. Clinical and laboratory findings: The most significant finding was thrombocytopenia and seropositive for Borrelia burgdorferi by IDEXX 4S Snap test. Treatment approach: treatment was established with tetracycline and doxycycline. Eight months later the dog showed signs of polyarthritis and received a second antibiotic treatment with remission of the disease and sero-reversion. Conclusions: This case is of epidemiological relevance because it is the first time canine borreliosis is evidenced by serology in dogs from an urban setting, suggesting the disease is moving on toward middle altitude and urban areas. Clinical signs and treatment schedule are reviewed.
Key words: Borrelia burgdorferi, canine borreliosis, thrombocytopenia, zoonosis.
Resumen
Anamnesis: un perro de la raza Bulldog francés de un año de edad, fue llevado a consulta por tener síntomas gastrointestinales, sin respuesta al tratamiento previo. Hallazgos clínicos y de laboratorio: el perro presentó trombocitopenia y serología positiva a Borrelia burgdorferi por IDEXX 4S Snap test. Tratamiento: El tratamiento se instauró con tetraclina y doxiciclina. A los 8 meses el perro mostró poliartritis y continuaba seropositivo, por lo cual recibió un segundo esquema con antibióticos que resulto en remisión de los signos y serorreversión. Conclusiones: este caso es de relevancia epidemiológica por ser la primera vez que se diagnostica la borreliosis canina en un área rural por serología, lo que sugiere que la enfermedad se puede estar desplazando hacia centros urbanos y mayores altitudes. En la discusión se revisan los signos clínicos y el esquema de tratamiento de la enfermedad en caninos.
Palabras clave: Borrelia burgdorferi, borreliosis canina, trombocitopenia, zoonosis.
Resumo
História: A consulta foi realizada a cão do raça buldogue francês de um ano, ter sintomas gastrointestinais, sem resposta ao tratamento anterior. Os achados clínicos e laboratoriais: o cão tem trombocitopenia e sorologia positiva para Borrelia burgdorferi pelo IDEXX 4S Snap test. Tratamento: o tratamento foi iniciado com tetraciclina e doxiciclina. Aos 8 meses, o cão tem artrite e manteve-se soropositivo, pelo qual recebeu um segundo esquema de antibiótico o que resultou em remissão dos sinais e sero-reversão. Conclusões: neste caso, é de importância epidemiológica por ser o primeiro borreliose canina diagnosticado sorologicamente em uma área rural, o que sugere que a doença está se deslocando para os centros urbanos e as altitudes mais elevadas. Na seção de discussão dos sinais clínicos e esquema de tratamento da doença em cães são tratados.
Palavras-chave: Borrelia burgdorferi, canine borreliose, trombocitopenia, zoonoses.
Introduction
Borreliosis or Lyme's disease was first described after the occurrence of an arthritis epidemy in Lyme, Connecticut in 1976 1. In 1982, a Spirochete was proposed as the etiology 2, subsequently confirmed on 3. Borrelia is a gram negative microorganism requiring two hosts for completing its life cycle: a mammal and an arthropod, the lattest an Ixodes tick 4. Clinical signs in dogs include fever, lethargy, claudication, local inflammatory reactions, pain, polyarthritis, renal and digestive abnormalities 5. Diagnosis is based on detection of circulating antibodies by ELISA, amplification of Borreliaburgdorferi genome by PCR, bacterial culture, and clinical laboratory findings 4-6. Treatment consists of the administration of antibiotics during 10 to 30 days (Including cephalosporins, amoxicillin, azithromycin or doxycycline 4,5 or even for more than 4 weeks 7. Prophylaxis is based on commercial vaccines 5,8,9 not available at the moment in Colombia. In the present work we report the presence of a probable case of Borreliaburgdorferi diagnosed by serology only in Medellin, Colombia, a city located at 1.540 m over sea level.
Patient examination
Anamnesis
A one-year-old male French bulldog was attended at the Small Animal Clinics of University CES (Medellin, Colombia). At consultation the dog had complete vaccination and anti-parasite schedules. The dog was presented due to recurrent emesis, loss of appetite and loose stools during the last four days. The owner reported that the dog was born in Colombia and has never left the country. The owner signed informed consent for sampling and data collection for this case report. The authors reported there is no conflict of interest.
Clinical findings and diagnostic aids used
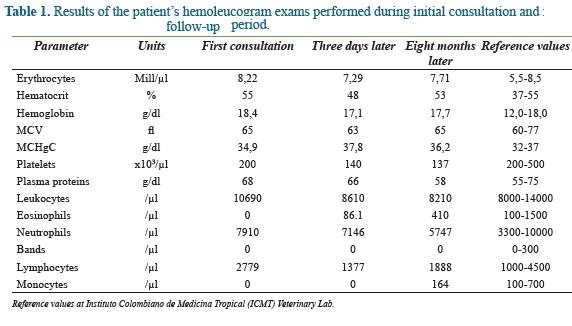
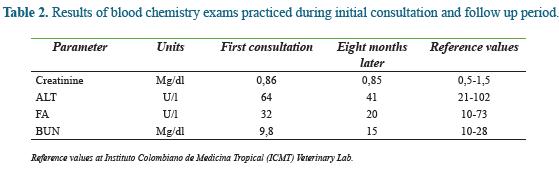
On physical examination, body weight, respiratory and cardiac frequency and capillary refill time were 12 kg, 30/min, 112 bpm, and 2 sec, respectively. Mucosae were normal and body temperature was 38 °C. The dog demonstrated pain at abdominal palpation, and then it was considered intestinal obstruction. Abdominal contrast radiography, hemoleucogram parameters (Table 1), serum alkaline phosphatase (AP), alanine amino transferase (ALT), blood urea nitrogen (BUN), Creatinine (Table 2) and fecal tests were performed.
Treatment approach
After no radiographic evidence of abnormalities in the intestine and no parasites detected in fecal test, a treatment for a general non specific condition was established as follows: 80 ml/kg/day crystalloids, 0,9% sodium chloride and 28 mg/kg/12 h dipirone. Twenty-four hours later 15 mg/kg/12 h metronidazole, 15 mg/kg/12 h trimetoprim-sulfa and 2 mg/kg/12 h ranitidine were instituted for therapy.
A comercial soft diet was also prescribed. In a control hemoleucogram exam performed three days later it was found thrombocytopenia (Table 1) then a Snap IDEXX 4S test was practiced (98.8% sensitivity, CI = 95.4%-99.9%; and 100% specificity, CI = 98%-100%)10 which detects antibodies against Ehrlichia canis, Borrelia burgdorferi, Anaplasma phagocitophylum and Dirofilaria Immitis specific antigens. The result was positive for Borrelia burgdorferi. No additional laboratory confirmatory evidence of the disease was made, like ELISA or PCR. Treatment was then completed with 5 mg/kg/12 h oxytetracicline. Once the oral way was restored the antibiotic was changed to 10 mg/kg/24 h PO/19 days doxycycline hyclate, 15 mg/kg/12 h PO/5 days metronidazol and 20 mg/24 h PO/10 days omeprazol. Eight months later, the patient was led once again at consultation when he was presented severe neck pain, and a progressive loss of appetite. No changes were observed at the vertebral column radiographic exam or in the hemoleucogram parameters (Table 1) or blood chemistry exams (Table 2). The dog was then treated with 30 mg/kg/2 days dipirone and 4 mg/kg/2 days tramadol, followed by 0.75 mg/kg dexamethasone and 2 mg/kg ranitidine. In addition, a control test resulted positive for Borrelia burgdorferi. The patient was given 5 mg/kg/12h during 25 days doxycycline. Nine months later two additional serological tests resulted negative.
Discussion
The occurrence of borreliosis and its clinical forms will depend on the species of Borrelia implicated, the zone of incidence, the continent where it occurs and the breed of the dog. According to Gerber et al. (2007), the predominant affected breed is Bernese mountain dog but they could not determine it to be a breed predisposition. In humans affected by the disease several species of Borrelia have been isolated and correlate with clinical sings and tissue tropism, a pattern of pathogenicity proposed to occur also in canine borreliosis 11,12. In several tropical regions of Colombia the disease was evidenced by serology: in Monteria (Capital of Cordoba State) a city located in a tropical low altitude (18 m above sea level), 12% seropositivity was found of in a sample of 200 dogs 13. Interestingly, a serological survey performed in a human population in the same region showed a 4.6% seropositivity 14. In the present case report the dog lived in Medellin city located at 1.540 m above sea level. This fact represent the first time borreliosis is reported in that altitude. Other studies have correlated the incidence of borreliosis to the frequency of Ixodes ticks that was found under the limit of 1300 15 and 1070 m above sea level 16 in Italy and Switzerland, respectively.
Several species of ticks including Ixodes vector of B. burdogferi, can be found in the tropical zone where the patient was located. In 25 Municipalities of the Antioquia State (Colombia), Rhipicephalus (Boophilus) microplus (Ixodes) was the predominant tick isolated in 68% of the cases 17. In contrast, 100% of captures were classified as Rhipicephalus (Boophilus) microplus in the Cundinamarca State (Colombia) 18.
Clinical signs of canine borreliosis may include pyrexia, loss of appetite, lethargy, lymphadenopathy, and polyarthritis 6, and glomerulonephritis that progress toward renal failure and myocarditis 4,11,12. Although the patient showed mild thrombocytopenia with platelet aggregation, changes in blood chemistry parameters are not specific. Krimer et al (2011) found claudication, anorexia, pyrexia and loss of weight with no neurological signs in patients affected by borreliosis 19. At the first consultation, the patient showed acute abdominal pain probably related to enteritis, whereas at the second one, presented thoracolumbar pain, acute cervical column pain, and loss of appetite.
Patients affected by borreliosis become seropositive and can persist as such for months, or years. The diagnosis is based on serological tests (ELISA, Direct Immunofluorescence), or antigen detection by PCR 4. The patient was diagnosed seropositive, and remained as such eight months later; however, at a sampling performed one year after the first consultation, he had seroconverted. Because of the highly complex behavior of the disease, Speck et al (2007), proposed a diagnosis schedule based on the results of hemoleucogram parameters, blood chemistry, urine analysis, testing for other infectious agents, rheumatoid factor, and antinuclear antibodies tests, with the aim to discard differential diagnoses 20. In a study conducted in New York (Westchester County) and Connecticut found that serotest results revealed little or no change in antibody titer for lame dogs given antibiotics or for healthy dogs 2 or more months after initial sample collection21. It is important to note that the patient was positive for serological diagnosis with a SNAP test and no diagnosis was supplemented, which makes the case is suspected but not confirmed the presence of the disease. This becomes the first epidemiological alarm to monitor the disease and begin to identify possible cases and if required begin prophylactic vaccination processes.
The current treatment of canine borreliosis is based on the use of tetracycline, mainly doxycycline, ampicillin or amoxicillin, third generation cephalosporin and/or erythromycin and its derivatives 11,22,23. In a review on human borreliosis (Lyme's disease) by Stricker (2007) the author stated that a 14 weeks antibiotic schedule is necessary for successful treatment of patients with persistent symptoms of the disease. In addition, this author mentioned that severity and duration of Lyme's disease may be aggravated by tick-born co-infections 7,24. The patient was treated with oxytetracycline followed by doxycycline, which resulted in a successful remission of clinical signs. Sero-reversion in the patient was in agreement with previous reports where patients sero-reverted after a successful antibiotic schedule 25,26.
Prevention of canine borreliosis is mainly based on vector control by using depot insecticides. The current available vaccination schedules 4,11,12,27, warrant immunity during one year 8. However, due to the lack of authorization for its use in Colombia, we recommend a program based on controlling ectoparasites by the use of spot-on products, or collars containing fipronil, amitraz or other acaricides. In several studies performed in Europe and in the United States, Ixodes ticks have prevalence of infections with Borrelia burgdorferi, between 4.6 and 7.8% 24,28. We can suspect an increase in the incidence of canine borreliosis in the near future. Similarly, the zoonotic potential should be taken into account for prevention and control of the disease.
Conclusion
Because of the high persistence of ticks in the Department of Antioquia as well as in other Departments of the Country, together with the possibility of a widespread distribution of ticks as a consequence of climate change, we must suspect an increase incidence of tick-borne bacterial infections. Finally, it is necessary to determine a diagnostic schedule aimed to detect these dogs in the early stages of the disease, which could provide the patient with a better prognosis and a greater expectancy of life and it is important to complement the serological diagnosis with ELISA and PCR, to establish more comprehensive diagnostics.
Acknowledgements
INCA-CES Research Group research activities are supported by Universidad CES (Medellin, Colombia). The authors thank Dr. Juan Maldonado-Estrada (Universidad de Antioquia) for his critical reviewing of the manuscript.
References
1. Steere AC, Malawista SE, Snydman DR, Shope RE, Andiman WA, Ross MR, et al. Lyme arthritis: an epidemic of oligoarticular arthritis in children and adults in three connecticut communities. Arthritis Rheum. febrero de 1977;20(1):7-17. [ Links ]
2. Burgdorfer W, Barbour AG, Hayes SF, Benach JL, Grunwaldt E, Davis JP. Lyme disease-a tick-borne spirochetosis? Science. 18 de junio de 1982;216(4552):1317-9. [ Links ]
3. Berger BW, Clemmensen OJ, Ackerman AB. Lyme disease is a spirochetosis. A review of the disease and evidence for its cause. Am J Dermatopathol. abril de 1983;5(2):111-24. [ Links ]
4. Fritz CL, Kjemtrup AM. Lyme borreliosis. J Am Vet Med Assoc. 1 de noviembre de 2003;223(9):1261-70. [ Links ]
5. Krupka I, Straubinger RK. Lyme Borreliosis in Dogs and Cats: Background, Diagnosis, Treatment and Prevention of Infections with Borrelia burgdorferi sensu stricto. Veterinary Clinics of North America: Small Animal Practice. noviembre de 2010;40(6):1103-19. [ Links ]
6. Wagner B, Freer H, Rollins A, Garcia-Tapia D, Erb HN, Earnhart C, et al. Antibodies to Borrelia burgdorferi OspA, OspC, OspF, and C6 Antigens as Markers for Early and Late Infection in Dogs. Clinical and Vaccine Immunology. 15 de febrero de 2012;19(4):527-35. [ Links ]
7. Stricker RB. Counterpoint: Long-Term Antibiotic Therapy Improves Persistent Symptoms Associated with Lyme Disease. Clinical Infectious Diseases. 15 de julio de 2007;45(2):149-57. [ Links ]
8. LaFleur RL, Callister SM, Dant JC, Jobe DA, Lovrich SD, Warner TF, et al. One-Year Duration of Immunity Induced by Vaccination with a Canine Lyme Disease Bacterin. Clinical and Vaccine Immunology. 17 de marzo de 2010;17(5):870-4. [ Links ]
9. Leschnik MW, Kirtz G, Khanakah G, Duscher G, Leidinger E, Thalhammer JG, et al. Humoral Immune Response in Dogs Naturally Infected with Borrelia burgdorferi Sensu Lato and in Dogs after Immunization with a Borrelia Vaccine. Clinical and Vaccine Immunology. 10 de marzo de 2010;17(5):828-35. [ Links ]
10. IDEXX L. http://al.idexx.com/html/es_es/smallanimal/inhouse/snap/4dx.html#tab4. [ Links ]
11. Hartmann K, Greene CE. Enfermedades provocadas por infecciones bacterianas sistémicas. Tratado de Medicina Interna Veterinaria. Sexta edición. Madrid: Elsevier Saunders; 2007. p. 616-31. [ Links ]
12. Little SE, Heise SR, Blagburn BL, Callister SM, Mead PS. Lyme borreliosis in dogs and humans in the USA. Trends in Parasitology. abril de 2010;26(4):213-8. [ Links ]
13. Buitrago F, Toloza R, Mestra A, Jaramillo P. Determinación de anticuerpos para Borrelia burgdorferi en perros mediante técnica de ELISA en el área rural del municipio de Montería - Córdoba. MVZ-Córdoba. 2003;8(1):282. [ Links ]
14. Miranda J, Mattar S, Perdomo K, Palencia L. Seroprevalencia de Borreliosis, o Enfermedad de Lyme, en una Población Rural Expuesta de Córdoba, Colombia. Rev Salud Pública. junio de 2009;11(3). [ Links ]
15. Rizzoli A, Merler S, Furlanello C, Genchi C. Geographical information systems and bootstrap aggregation (bagging) of tree-based classifiers for Lyme disease risk prediction in Trentino, Italian Alps. J Med Entomol. mayo de 2002;39(3):485-92. [ Links ]
16. Burri C, Moran Cadenas F, Douet V, Moret J, Gern L. Ixodes ricinus density and infection prevalence of Borrelia burgdorferi sensu lato along a North-facing altitudinal gradient in the Rhône Valley (Switzerland). Vector Borne Zoonotic Dis. 2007;7(1):50-8. [ Links ]
17. López VG, Zúñiga AI, Villar CC, Osorio GD. Distribución de garrapatas en 25 municipios del departamento de Antioquia. Revista ICA. 1985;20(1):40-4. [ Links ]
18. Cortés JA, Betancourt JA, Arguelles J, Pulido LA. Distribución de garrapatas Rhipicephalus (Boophilus) microplus en bovinos y fincas del Altiplano cundiboyacense (Colombia). Corpoica Cienc Tecnol Agropecu. 2010;11(1):73-84. [ Links ]
19. Krimer PM, Miller AD, Li Q, Grosenbaugh DA, Susta L, Schatzberg SJ. Molecular and pathological investigations of the central nervous system in Borrelia burgdorferi-infected dogs. Journal of Veterinary Diagnostic Investigation. 13 de junio de 2011;23(4):757-63. [ Links ]
20. Speck S, Reiner B, Streich WJ, Reusch C, Wittenbrink MM. Canine borreliosis: A laboratory diagnostic trial. Veterinary Microbiology. febrero de 2007;120(1-2):132-41. [ Links ]
21. Magnarelli LA, Anderson JF, Schreier AB. Persistence of antibodies to Borrelia burgdorferi in dogs of New York and Connecticut. J Am Vet Med Assoc. 1 de abril de 1990;196(7):1064-8. [ Links ]
22. Wormser GP, O'Connell S. Treatment of infection caused by Borrelia burgdorferi sensu lato. Expert Review of Anti-infective Therapy. febrero de 2011;9(2):245-60. [ Links ]
23. Littman MP, Goldstein RE, Labato MA, Lappin MR, Moore GE. ACVIM small animal consensus statement on Lyme disease in dogs: diagnosis, treatment, and prevention. J Vet Intern Med. abril de 2006;20(2):422-34. [ Links ]
24. Wodecka B, Rymaszewska A, Sawczuk M, Skotarczak B. Detectability of tick-borne agents DNA in the blood of dogs, undergoing treatment for borreliosis. Ann Agric Environ Med. junio de 2009;16(1):9-14. [ Links ]
25. Mitchell PD, Reed KD, Hofkes JM. Immunoserologic evidence of coinfection with Borrelia burgdorferi, Babesia microti, and human granulocytic Ehrlichia species in residents of Wisconsin and Minnesota. J Clin Microbiol. marzo de 1996;34(3):724-7. [ Links ]
26. Gerber B, Haug K, Eichenberger S, Reusch CE, Wittenbrink MM. Follow-up of Bernese Mountain dogs and other dogs with serologically diagnosed Borrelia burgdorferi infection: What happens to seropositive animals? BMC Veterinary Research. 2009;5(1):18. [ Links ]
27. Littman MP. Canine borreliosis. Veterinary Clinics of North America: Small Animal Practice. julio de 2003;33(4):827-62. [ Links ]
28. Reye AL, Hubschen JM, Sausy A, Muller CP. Prevalence and Seasonality of Tick-Borne Pathogens in Questing Ixodes ricinus Ticks from Luxembourg. Applied and Environmental Microbiology. 1 de mayo de 2010;76(9):2923-31. [ Links ]
