











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink1. Introduction
Virtually all pathologies of the nervous and musculoskeletal systems are manifested through movement dysfunctions. Autosomal dominant hereditary ataxias form a heterogeneous group of neurodegenerative conditions characterized by progressive neuronal loss of the cerebellum, brainstem nuclei, and spinocerebellar tracts [1].
Within this family, type 2 cerebellar ataxias (SCA2) are the most frequent in Cuba, with the main clinical manifestations the ataxia of gait, dysmetria, dysarthria and adiadochokinesia, and anticipating in all cases the age of onset of the disease in 6 years compared to previous generations [2]. Another distinctive feature of the disease is the progressive deterioration of the gait and mobility of the person who suffers from it until death, making it a serious health problem.
Since there is no cure, an important part of the therapeutic treatment of SCAs focuses on rehabilitation [3][4][5] and there are few studies carried out to clarify the causes of their kinematic manifestations, which is due to factors related to the micro-localization of cases worldwide and factors associated with difficulties with homogeneity in patient recruitment and the diversity of methods used in the biomechanical studies of movement disorders, which has led in many cases to draw contradictory conclusions [6][7][8][9].
In Cuba, cerebrovascular accidents (CVA) rank third as the cause of general death, the first cause of death of neurological origin, as well as the most frequent basic cause of death among the deceased. They generate a high cost and expense of material and financial resources.
This is due to severity, length of hospitalization and rehabilitation time [11][12]. Associated with the anatomical location and magnitude of the CVA, patients frequently present sequelae related to biomechanical disorders associated with the execution of movements, which complicate the process of walking, contribute to the loss of balance and cause falls [13][14].
From a diagnostic point of view, visual analysis of patients with complex movement disorders is limited. Typically, the evaluation is conducted with a certain degree of subjectivity, through qualitative assessments involving clinical scales and the criteria of medical experts 15][17].
In addition to the above problem, the fact that the uniqueness of human movements depends on the socio-economic and life conditions of the populations of individuals, and currently have a quantitative method for the evaluation of kinematic disorders of the march, which hinders the planning of rehabilitation actions that should be applied.
2. Methodology
The methodology followed for the development of the study carried out consisted of 3 stages. The first focused on the assembly and metrological validation of a videography system adapted to the study of motor disorders in patients in a hospital setting [18].
The second stage included the analysis and descriptive-multivariate evaluation of 3 movement structures executed by groups of healthy and sick subjects under laboratory conditions and the third stage focused on obtaining and validating gait models and classifiers from the kinematic data of the groups of people studied (figure 1).
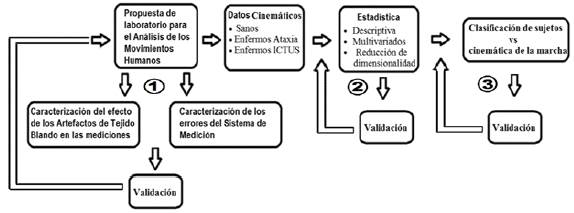
Figure 1 Methodological proposal. (In graphic: *Laboratory proposal for the analysis of human movements. *KINEMATIC DATA: Healthy, Sick Ataxia, Sick ICTUS. *STATISTICS: Descriptive, Multivariate, Dimensionality reduction. *Classification of the subjects vs Kinematics of the march. *Characterization of the effect of soft tissue artefacts in measurements. *Characterization of measurement system errors. *Validation).
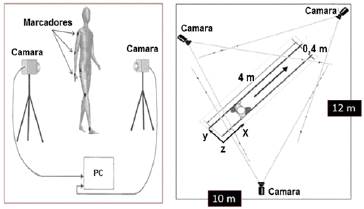
Figure 2 Measurement set, composed of anatomical markers, spatial distribution of cameras and computer for motion capture.
The passive markers used were positioned on the surface of the body according to different spatial configurations and their trajectories were obtained by means of an ATI model 9600 video capture card, with 64 MB of video memory and a spatial resolution of 240 x 480 pixels which was coupled to a computer. It was worked at a frequency of frames corresponding to (30 c/s) and a shutter ratio of 1/500 seconds.
2.2 Metrological validation
For the metrological validation of the instrumentation used, an electromechanical device was designed and constructed from which the dimensional errors of the study volumes in each of the laboratories employed were obtained and analyzed.
This task required a multifactorial study in which speed, diameter and inter-marker distances were analyzed to determine the precision and accuracy of the measurements made with the videography system, as well as the simulation of the occlusion of the marker trajectories by means of the rotation of a cluster of markers placed at the end of the arm of the built device (figure 3).

Absolute errors (ABSE) were calculated as the difference between the inter-marker length of the pattern used, measured with a digital caliper (precision ± 0.001 m) and the one obtained after the digitization of the cluster markers with the videographic technique (equation 1). Similarly, the mean of the errors was used as a reference to evaluate the accuracy of the measurement system [19].

(In the equation: Distance patterns)
Where: X2, X1, Y2, Y1, Z2, Z1 are the coordinates in the 3D space of the markers.
2.3 Protocol for the evaluation of the kinematics of movements
A cross-sectional descriptive study of 33 patients (16 men and 17 women) with clinical-neurological diagnosis of spinocerebellar ataxia was performed [20]. The sample also included 28 patients with CVA, 10 men and 18 women with clinical and imaging diagnoses of occlusive episode in the middle cerebral artery, attended at the General Hospital Dr Juan Bruno Zayas Alfons, from January 2000 to December 2016.
Likewise, it was included a sample of 51 healthy individuals older than 18 years (18 men and 33 women, with an average age of 51 and 54 years, respectively), randomly chosen, with no family and consanguineous relationship with the patients, without a history of having suffered from diseases related to movement disorders or accidents (Table 1).

For the quantitative evaluation of kinematic disorders, the participants (healthy and sick) were filmed during the realization of 3 structures of movement, gait (a), sitting-standing up-sitting (b) and plant-extension with the tip of the foot (c) (Figure 4).
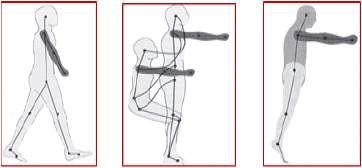
Figure 4 Evaluated movement structures, (a) gait, (b) sitting-standing up-sitting of a chair, (c) plant- extension with the tip of the foot.
Participants were asked to perform the 3 motor tasks routinely on 30 occasions. The gait was carried out in a straight path of 10 m in both directions and a regulated chair was provided to guarantee a 90° bending angle in the knee during the sitting position.
Likewise, spherical markers of 0.020 m in diameter (covered with reflective material) were placed in different locations (sacrum, iliac crests, mid-lateral portions of the thighs and triceps sural, external condyles of the femur, lateral malleoli, posterior back) of both calcaneus, fifth metatarsal and greater toe of both feet) [21][22][23][24][25][26][27].
Patients who required technical aids to perform the movements, had heart and respiratory affections, musculoskeletal conditions and a proven history of accidents and falls, were excluded from the study.
2.4 Protocol for the classification of normal and pathological motor skills
A multivariate cross-sectional study was conducted using Principal Component Analysis (PCA) as a dimensional reduction technique, the results of which allowed the objective identification of the motor activity that contained most of the kinematic disorder, reflected in the greater amount of altered kinematic variables (differed significantly) with respect to normal behavior.
From the kinematic data of the selected motor activity, the classification models for each age group were obtained, as well as for the 2 pathologies, they were subjected to a cross validation with data of healthy and sick individuals who were not part of the initial design of obtaining said models [28].
Dimensionality reduction and the classification was made using Minitab® R16 software and Mathlab® R2010b software, and for the acquisition, pre-processing, calculation and filtering of the kinematic registers, the Human® software of HMA Technologies Inc. was used.
3. Results and Discussion
3.1 Metrological characterization technique of videographic
The metrological characterization of the videographic technique used for the analysis of movements was made based on the analysis of measurement errors in 3 laboratories.
The precision validated with the videographic technique poses error magnitudes of less than 12 % with respect to the variable of lesser metric magnitude, the step width, of approximately 110 mm. Similarly, the fact that the low rotation speeds of the marker cluster influenced the increase in precision (fast speed - errors of 0.0053 m; slow speed -errors of 0.0049 m for the inter-marker distance of 0.3 m), corresponds to the results described by other authors.
As the speed increased, there was a loss of resolution of the marker contour, resulting in poor location of the marker center with the pattern recognition tools of the automatic digitalization software and of the technician when manual digitalization was used [19]. A similar behavior to the mean of the errors (2 to 3 mm) was observed between the Canadian laboratories for 2 speeds of movements (fast 72 rpm and slow 27 rpm) and in the case of the laboratory of the General Hospital "Dr Juan Bruno Zayas Alfonso" a difference of around 5 mm was obtained between the mean of the errors, registering for the slow speed 10 mm and 15 mm for the fast one, (figure 5 ).
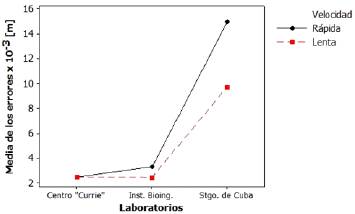
Figure 5 Mean values of errors for factor interaction, laboratory and speed, 0.1 m inter-marker distance. (In graphic: X-Axis: Average errors x 10-3 (m). Y-Axis: Laboratories. Conventions: Speed, Fast/Slow).
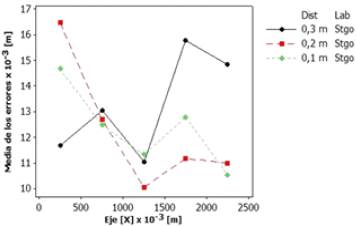
Likewise, the study of the distribution of errors within the study volume (2.5 m x 1 m x 1 m), proposed for the biomechanical evaluation of the locomotor apparatus of patients with SCA and CVA, showed that the central portion (with respect to the orientation in the x-axis) of the study volume of the laboratory of the General Hospital of Santiago de Cuba corresponds to the region of highest precision of the measurements, which ranged between 10 mm and 12 mm for inter-marker distances that varied between 0.3 m and 0.1 m, (Figure 6).
3.2 Biomechanical characterization of movement disorders in healthy subjects and patients with SCA and CVA.
For the 3 movement structures evaluated, the results of the descriptive study and the comparison of kinematic patterns in men and women, healthy and sick with the 2 diseases showed a decrease in movement speeds (gait, ascent and descent), the cycle and step lengths with an increase in gait width and lift base, lateral oscillations of the hip and of the times (of support, of cycle and of double support). See Figure 7 for results of locomotion in SCA.
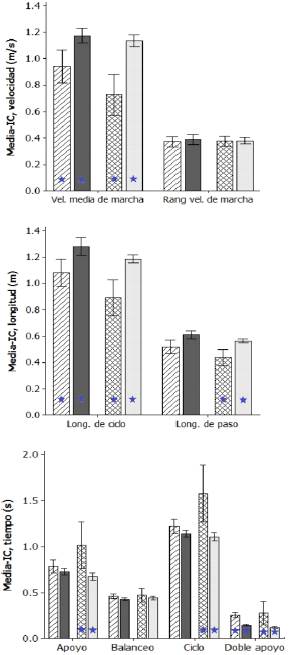
Figure 7 Behavior of kinematic parameters of gait, mean and confidential interval (95%) in men and women, healthy and sick with SCA. (In graphic: 1st graphic. X-Axis: Mean speed of the march, Speed range of the march. Y-Axis: MEAN-IC, speed (m / s). 2nd graphic. X-Axis: Cycle length, Step length. Y-Axis: MEAN-IC, length (m). 3rd graphic. X-Axis: Support, Swinging, Cycle, Double support. Y-Axis: MEAN-IC, time (s).
In the 3 structures of movements evaluated, the results of the descriptive study and comparison of kinematic patterns in men and women, healthy and sick with SCA and CVA, corroborated the need of patients to practice a slow and insecure gait.
This gait is characterized by the generation of small ranges of movements and an exaggerated increase in spatial parameters related to stability, aspects that coincide with that reported in the literature [20].
Once the PCA technique was applied in the groups of patients, it was evidenced that the gait was the physical activity that best described the movement disorders present in the groups of men and women, healthy and sick with SCA and CVA.
3.3 Behavior of discriminant linear models
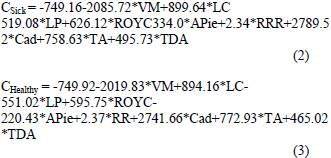
In the group of healthy and sick men with SCA the model allowed the classification of 94.12% of the individuals, with a 0.775% correlation and a high level of statistical significance (p<0.05).
Male sex SCA:
Also, in the group of women with CVA, a discriminant model was obtained that allowed the classification of 100% of healthy and sick women with CVA, with a 0.921% correlation and high level of statistical significance (p<0.05).
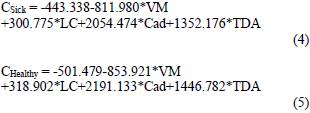
In the group of healthy and sick men with CVA, the model allowed the classification of 100% of the individuals, with a 0.97% correlation and a high level of statistical significance (p<0.05).
Male sex with CVA:
The validation of the discriminant models was made from the kinematic parameters of the gait obtained from 3 patients with SCA (2 women and 1 man), randomly selected, whose kinematic parameters were not used to obtain the models.
Similarly, 5 subjects with CVA (2 women and 3 men) were randomly selected whose kinematic parameters once introduced in the corresponding models allowed the correct classification of all of them.
4. Conclusions
The study conducted, based on the use of the videographic technique, the evaluation of kinematic parameters of the locomotor system, related to the execution of 3 physical activities of daily life, allowing the analysis of kinematic parameters in samples of healthy and sick individuals with SCA and CVA.
The results of the study of the 3 movements in the 2 groups of patients with SCA and CVA, revealed that the movement disorders were characterized in a general way, by the decrease of the spatial parameters of the partial realizations. The most important parameters are step length, cycle length and the maximum height of the food, combined with the increase in the execution times of each of the particular phases.
The metrological characterization of the laboratory for the analysis of human movements, allowed to obtain the dimensions and distribution of the errors within the volume of study. The validation of the method was carried out using the theoretical model obtained in clinical protocols oriented to the study of 2 neurological diseases.
Videographic measurements of the gait allowed to obtain the discriminant functions for the classification of groups of healthy and sick people with SCA and CVA, which has made it possible to have the first quantitative tools aimed at complementing the evolutionary monitoring of motor skills.

