











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkI. Introduction
A patient death reporting study made between 2010 and 2012 in an English hospital showed that the 6% of a sample of 2010 cases resulted from the equipment failure due to its bad usage, bad setting or bad reading by health professionals3.
An appropriate training to the assistant personnel allows to know and practice the correct technology management which provides greater security to the patients, as well as better diagnostics and treatments. In long terms this helps to reduce the incidence of medical equipment failure, since a great percentage of accidents and damages originates from mistakes made by the operator when the implementation of biomedical equipment fails4.
Measure usability in health-care environments allows to optimize the benefits of technology implementation. Studies carried out in Finland about health-care personnel experience with the EHR (Electronic Health Record) demonstrate the need to optimize the implementation of health technologies. According to statistics reported in 2014, the knowledge using these Systems remains as critical as in 20105.
To achieve this objective, trained personal should give continuous training to health-care entities that are governed by mandatory regulations on technovigilance. One of them is about technological training on medical devices and services necessary to the correct functioning of medical equipment. In Colombia it is stablished by the Invima on the decree 4725 of 20051 and on the resolution 2003 of 2014 issued by the Colombian Ministry of social protection2 that is related to training protocols in companies providing health-care services. Other voluntary standards like ISO 9001 of 2015, establish a model to ensure a quality management system in products and services6. ISO 13485 of 2016 specifies requirements for a quality management system7 and national health-care accreditation with its technology standard focused on efficiency, effectiveness and safety8. All these regulations indicate the minimum requirements for a medical center due to the constant newtechnology acquisition, personnel exchange, or just by the inexperience on the correct equipment usage4.
There are several and accessible training models that can be carried out by determining the best way to do it. Based on this study it is intended, first, to incorporate training models by analyzing and coupling its results obtaining a structured and improved plan to perform this work in an optimal manner; and second, to assess the efficiency of different methodologies implemented in the training as well as their impact through some kirkpatrick-model parameters to afterwards analyze the results by quantifying the knowledge through written and practical tests.
II. Methodology
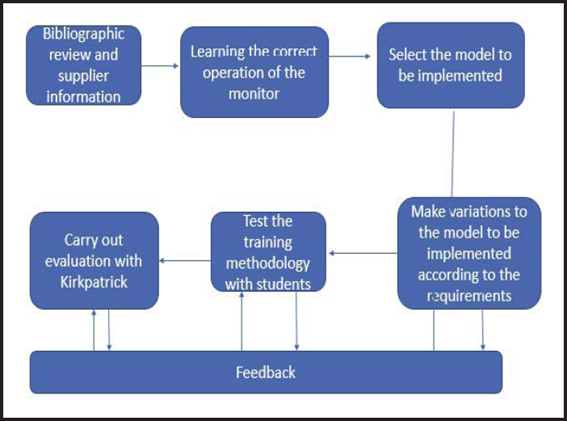
For the correct development of the project, it is intended as a first instance, to execute a management plan that will help us to solve the problem in the most appropriate way.
The project contains several stages. First of them is search bibliography regarding the basic concepts of healthcare personnel training, which is mainly emphasized in vital-sings monitors. Secondly, acquire excellent knowledge and skills to manage vital-sings monitor by applying theoretical resources to the practice. In third place, search various training models and chose one to apply. Accordingly, adjustment stage is the last one, executing variations to obtain different results that were analyzed based on the feedback received.
The process was divided into a theoretical and a practical test, both consist of a series of functions to perform or theory to know about the biomedical device of a document provided by the provider with some modifieds because the document was one of the reference of series but no with vital-signs monitor implemented, the final test consisted of 30 questions.
Based on different training methodologies implemented, were applied the first two levels of kirkpatrick model that are reaction and learning; the first one with the purpose of measuring the participants satisfaction, and the second one, of describing the increase of people’s knowledge and skills as a training consequence; in order to determine the process value9. The learning level was assessed by two parameters: right answer and response time. The right answer through a theoretical test and by right answer and response time through a practical test.
The training was made with a real vital-signs multiparameter monitor with 10 parameters (ECG, QRS detection range, ST ,arrhythmia detection, respiration, SpO2, temperature, NBP, invasive blood pressure, cardiac output) the display is a TFTLCD type with a diagonal size of 310 mm (12.2 in), resolution of 800 x 600 pixels and 6 standard or 8 optionals channels, the rotary knob and fixed keys allows easy to use menu structure ; physically the vital-signs monitor are H x W x D 272 x 384 x 190 mm (10.7 x 15.1 x 7.5 in) and 6.2 kg (13.6 lbs) weight and with external battery 6.8 kg (14.9 lbs)11 according to the expert´s advice, this type of monitors is generally used in intensive care units or surgeries. We took the answers from a vital-sings monitor expert as the reference to establish the assessment range (from 1 to 3, being 3 the highest level and 1 the lowest) based on rubrics.
The first part of the present project was made with students to strengthen their abilities as they will have to solve this type of situations in the future, wherefore bioengineers must impart training to assistance personnel in healthcare facilities. This is intended to increase the health-care personnel problem-solving skills with vital signs monitor.
Initially three sessions are held in which the population is characterized and describe the methodology to be performed Session I: group of 30 bioengineering students coursing the fifth semester.
Initially a global theoretical introduction is made about the monitor and why it is necessary to perform these procedures, later for the training of equipment management.
The session was divided into 2 parts in order to compare and analyze the results obtained from a subgroup of people who were statistically with non-probabilistic sampling10 chosen to perform the evaluation of theoretical or practical knowledge after the training.
In order to compare the results of session 1, a practical training session is held with a group of 20 bioengineering students coursing the eighth and ninth semester where a group of 10 people were statistically with nonprobabilistic sampling10 chosen to perform the practical test and a theoretical training session is held with a group of 10 bioengineering students coursing the six semester, in this session all population realized the theoretical test.
III. Results
The results obtained on the project were based, first, on the characterization of the population to be trained on biomedical technology; second, on the establishment of the training protocol implemented for each variation; and lastly, on the assessment of the established parameters.
The functions contained in the user manual provided by the medical device provider, were classified in two levels: basic and intermediate depending on the complex and number of steps that the user must follow to perform the basic functions that the health-care personnel must know in this case12,13, according to an expert from the medical device company, used as a reference.
The questionnaire was carried out after the training and consists of 30 questions about appropriate connections, functions or commands to perform some action or measurement of the body through the monitor and others about theoretical knowledge.
Table 1 Results of training 1, 2 and 3
| Session | 1.Theory practice | 2.Practice | 3.Theory |
|---|---|---|---|
| Number of participants evaluated | 16 | 10 | 10 |
| Duration of sesión (minutes) | 45 | 40 | 40 |
| Number of participants that realized theoretical test | 8 | - | 10 |
| Number of participants that realized practical test | 8 | 10 | - |
| Average of the correct questions answered from the theoretical test | 13/30 | 28/30 | 17/30 |
| Average of the correct questions answered from the practical test | 19/30 | 28/30 | 20/30 |
| Average time per question in practical test (seconds) | 69 | 60 | - |
| Frequently asked questions | Difficult visualization of the monitor and more specific procedures. | More training time, make more measurements. | Unfavorable methodology |
| Specific result | 1,97/3 | 2,62/3 | 1,25/3 |
Table 1 shows the different training sessions, the results and the characteristics of each one.
Based on the results obtained through the different sessions, a comparison is made between the performance and learning of the students in the two modalities of evaluation.
Session 1
The following figures represents the results obtained from the theoretical and practical part of session 1 that shows number of participants answer correctly each question.
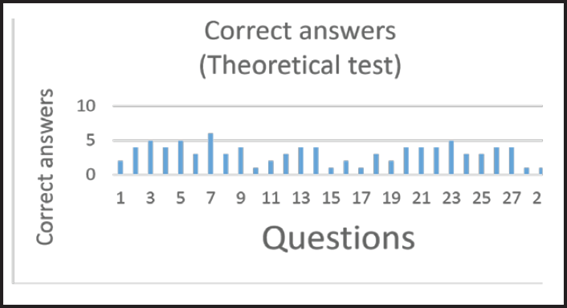
Figure 2 Number of subjects matching the right answer according to the theoretical trainning in session 1
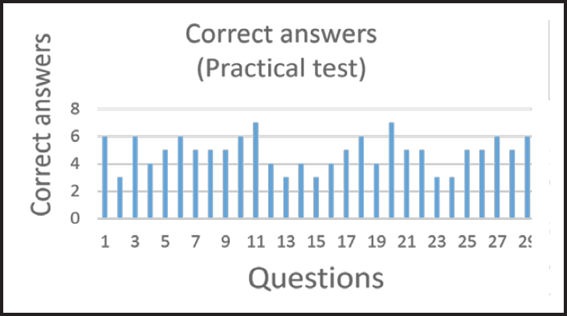
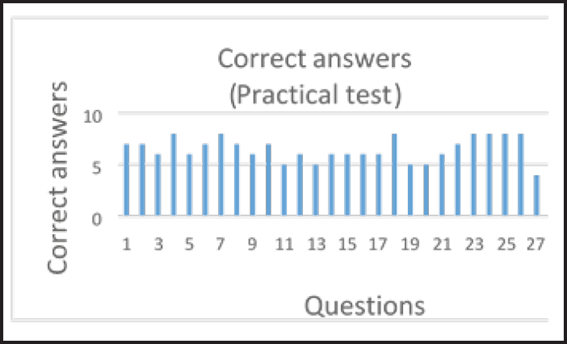
Figure 3 Number of subjects matching the right answer according to the practical training in session 1
Session 2
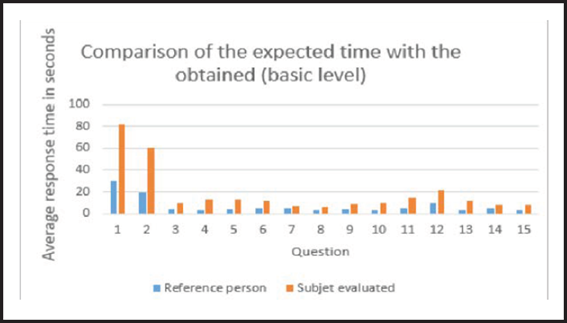
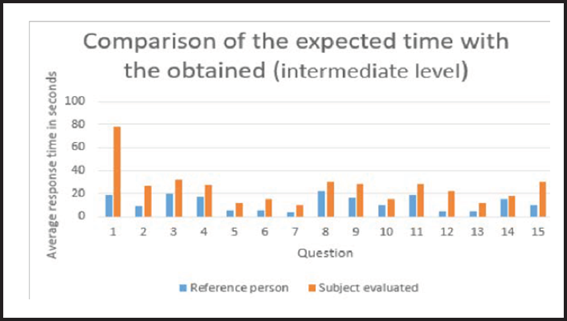
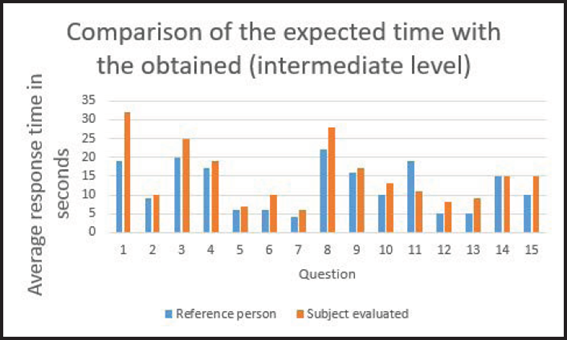
The next figures represents the resuls obtained from the practical part by session number 2, the first one shows number of participants answer correctly each question and the others show a comparison between the results obtained in sessions 2 in terms of the responses of the basic and intermediate level evaluations respectively, as well as in terms of the guidelines of the provider advisor taken as a reference to assess the knowledge level to manage vitalsings monitors.
From both graphs 2 and 3, it is possible to identify some questions in which knowledge should be reinforced, also, it should be noted that the results brought out from the theoretical training were not as satisfactory as the results from the practical training.
The Fig. 4 and 5 show a comparison between the results obtained in practical sessions 1 in terms of the responses of the basic and intermediate level evaluations respectively, as well as in terms of the guidelines of the provider advisor taken as a reference to assess the knowledge level to manage vital sings monitors.
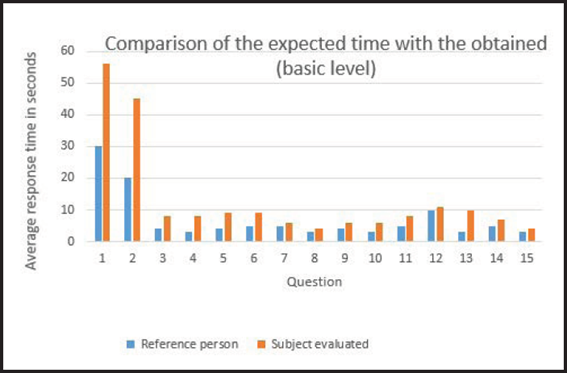
Figure 6 Number of subjects matching the right answer according to the practical training in session 2
Session 3
The last session corresponding to Fig. 9 that represents the results obtained from the theoretical session 3 that shows number of participants answer correctly each question.
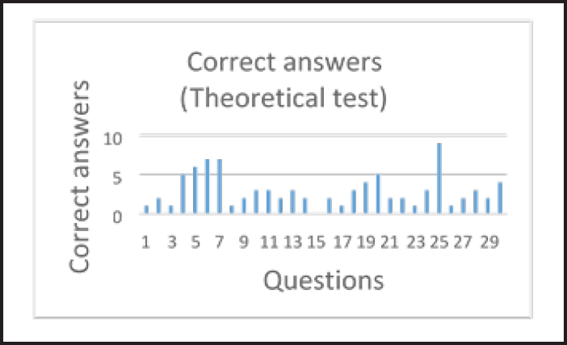
Figure 9 Number of subjects matching the right answer according to the theoretical training in session 3
By means of this last graph compared to the others we can see that it was the session with the worst results.
IV. Discussion
Session I
At the training beginning, the students were question about their knowledge on vital-signs monitors. Despite they had zero knowledge on this equipment, it was possible to obtain an optimal result in the training development, as shown in Table 1 presented in the results. Comparing Fig. 2 and 3 it was observed that the practical training is the best option to carry out the training.
Through the analysis of the response times we can observe the great need to strengthen these processes since it is remarkable the difference with respect to the expert and from the strengthening of the bases we get to broader knowledge that favor the implementation of technology in medicine.
On the part of the satisfaction responses on the part of the personnel, the change was observed in the good comments by the students trained under the practice that were motivated and interested in the subject with respect to the students trained under the theoretical modality Which made comments of dissatisfaction or constructive criticism for a next event.
Session II
Implementing a process with physical technology interaction contributes to a better development in the understanding of the trained participants, since this visual stimulus helps them to record in an easier way the procedure to be performed. All the results obtained in all the scenes made It is highlighted that in this section the results were obtained More optimistic of the project, in the graphs 6, 7 and 8 Evidence as the subjects in the question Answers to the different types of evaluation According to the satisfaction survey people were comfortable with the way of training, the comments were positive.
Session III
The graph 9 obtained in this series with graphs 6, 3 and 2 shows the unsatisfactory results obtained by means of the theoretical training, the correct answers are inferior in comparison with the result of the other interventions According to the satisfaction survey, trained subjects did not adequately assimilate the training process, comments were obtained such as “more iteration at the time of training”.
A future work should be focused on improving the training processes based on the results and its considerations; in order to guide a project aimed to healthcare personnel as well as to their needs in the different areas since the implementation of these monitors is broad and will depend on the professional’s needs.
V. Conclusion
Through the different bibliographic resources it can be see the great need to expand knowledge and to strengthen the training plans from the grassroots and then to lead to new projects that extend throughout the field of health-care because the ability to implement biomedical technology is proportional to the health-care services quality and it avoids accidents with patients and equipment.
The lack of information about this great problem minimizes the solutions that cover this great risk, therefore, to make aware personnel about risks from different factors like patient’s life, accidents, mishaps, costs, medical equipment preservation, is a key factor to offer training.
Based on the different graphics and on every process that represents the vital signal monitor trainning, it was found that the number of participants affects the training quality for different factors like: visibility and equipment interaction.

