











 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkI. Introduction
In august of 2015 the country had registered in Special Register of Health’s Service Providers (R.E.S.P) a total of 42.912 providers of which 23% are Health’s Provider Institution (I.P.S), 73% are independent, 3% are foundations or public companies and 1% are the patient’s transport service1. According to the World Health Organization (W.H.O), Colombia shows an increased offer of health services in the last 5 years, however the service is still in deficit1.
In Colombia the health’s architectonic projects are regulated by several standards, one of the most important is the law 9 of 1979 (about Sanitary measures for the environment and Sanitation of buildings) and the resolution 4445 of 1996 (rules for compliance of the 9th law) that regulates the design and the construction of hospitals. The actual regulations are considered outdated, in their conceptualization, management and application because in 20 years these have changed in technical, technological and scientific aspects boosted by the great advances of medical science and technology2. The National Administrative Department of Statistics (D.A.N.E) reported that in 2001 1 bed was registered per one thousand population, number that improved for 2011 where 1.4 beds per one thousand population were reported and a study of 2015 1.5 beds per one thousand population found it, that indicates that the number of beds is getting better but it didn’t meet the minimum amount recommended by the W.H.O yet there are 2.6 beds per one thousand population. Counting with more that 48 million population in 20163.
This project seeks to deliver information of a model for design and construction of third level complex Hospitals and Clinics in Colombia, making emphasis in the cost of design and construction stages. For that is necessary to tell the experience of personal vinculated with the medical and architectonic program in this kind of projects, searching the costs, time and personal workers that are necessary, also the disciplines and the normative that are involved.
A comparison method of design and construction cost is implemented in models of USA and Argentina countries. This result seeks to stand out the role of Bioengineer or Biomedical engineer into this labor, because that is the main bridge between the medical area, the technical area and the normative component that collects all the development of hospitality engineering project.
A search for recent private and public hospital construction projects in Colombia was carried out in order to identify the magnitude of health projects in the last ten years. Data from D.A.N.E show how the area under construction of hospitals and clinics has increased in recent years. Thus, by 2014, according to this statistical entity, 850 thousand square meters of health infrastructure were being increased4,9.
II. Methodology
In the diagram that shows the development of the methodology:
A. Investigation:
Technical rules for health’s centers construction.
Models used for national and international health centers development.
Life experiences of design and hospital’s construction.
B. comparison:
Advantages and disadvantages of models and its respective analysis.
Comparison and cost analysis of the different projects consulted.
Identify the bioengineers role in the all development of hospital’s design and construction.
C. Creation of new model
III. Background
Normative revision of Colombian legislation
An investigation was made of the Regulations that must be fulfilled in each of the technical studies for the construction of clinics and hospitals and it is found that they are about 20 sets of regulations applicable to the following technical studies necessary for the construction of clinics and hospitals:
Architectural design
Design and electrical studies
Design and studies of medical gases
Structural Design and Studies
Soil and topographic designs and studies
Environmental Studies
Legal, licensing, environmental and mobility studies
Design and study of communications, networks
Signal designs
Hydrosanitary designs and studies
Design and networks against fire and life safety
Design and study radiation protection
Evaluation of medical and non-medical technology
Risk management
Communication and Network Studies
For some of these studies the standards were created several years ago and it is possible that they will no longer apply the correct fulfillment by the development of new technologies and materials, for example Law 09 of 1979 where they talk about the architectural studies.
Finding that the main laws in the Colombian legislation are:
Law 9 of 1979: this law dictates sanitaries actions for edifications to prevent and control the physical, chemical and biological agents that could be dangerous.
Resolution 4445 of 1996: contains rules for accomplishment of law 9. NSR 10 of 1998: these are the colombian earthquake resistant normative for design and construction.
Resolution 2003 of 2014: It defines the procedures and conditions of inscription for health service providers and enabled their services.
Bibliographic revision of models
At this stage the investigation of some of the best known models in countries like Argentina and US is realized.
Table 1 Main data of the models consulted
| U.S MODEL | ARGENTINA MODEL |
|---|---|
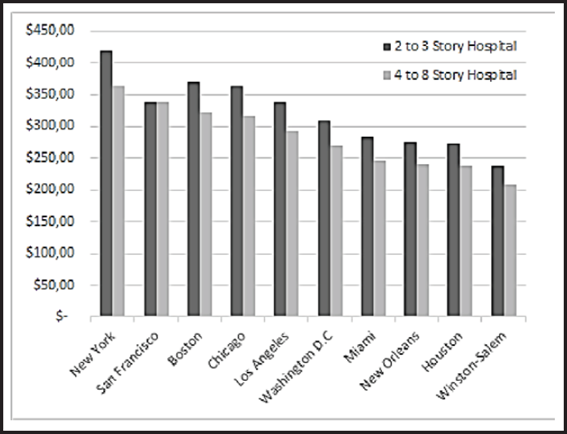
| Also known as Hospital of height, having characteristics like compact block, less path and optimized economy in their plant, hospitals with the shape like T, H, or Y. The definition of project needs, new materials and edge technology(6). The construction costs have great variety according to the place in which it is built. As it can be seen in Fig. 1. New York is more expensive than other places. Comparing the construction prices between one medium that has 2 to 3 floors and one large that has 4 to 8 floors (Fig. 1). For both kind of hospitals it could be seen that it is more expensive to build a medium-sized hospital between 2 and 3 floors(7). | The design model implemented is the organic model or No Model Topology, that is sustainable and respects the land on which the building is implanted(4). The Primary Health Care Government plan of Buenos Aires city, says that for every hospital there are 20 health centers that help to supply the population in need. Each health center has 300 square meters, and indicates that the construction cost per square meter is $ 2300(5). |
Construction forms in Colombia
In Colombia there is no defined model for design and construction, because the number of rules don’t facilitate the work, showing that existing buildings are adaptations of other countries, which have different geography, demography and standards.
The Colombian Association of architects and hospitalary engineers (ACAIH) and the Colombian Society of Architects actually are the specialized guilds in proper development planning processes, supervision, staffing, technical studies, architectural and construction design; one of his contributions was the updating of resolution 4445 by 1995 following the guidelines of the law 9 of 19798.
The construction cost of a third level hospital with an area of 20.000 m2 on an estimated time of 20 months is more or less 3 or 4 pesos millions for square meter.
As a result of the bibliographic search, it arrives at an estimated cost per square meter in the United States, Argentina and Colombia, the US being the country with the largest value of $ 3,021/m2, Argentina in second place with a value of $ 2,300/m2 and Colombia in the last place with a value of $1,400/m2, differences are shown in Table 1. The currency conversion rate was COP $ 3100 and the conversion into measures for 1 square meter are 10.7639 square feet.
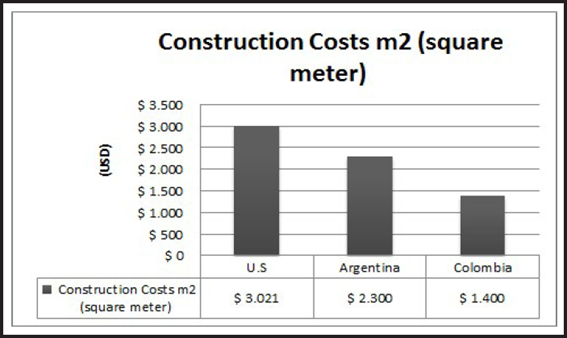
Table 3 Average cost of square meter design for hospitals of 3rd level of complexity
| Project | # of beds | Square meters | Year | Cost (COP) |
|---|---|---|---|---|
| Project 1 | 300 | 64000 | 2013 | $ 270.000.000.000 |
| Project 2 | 500 | 110000 | 2011 | $ 263.500.000.000 |
| Project 3 | 409 | 70000 | 2015 | $ 350.000.000.000 |
| Project 4 | 131 | 27000 | 2015 | $ 138.000.000.000 |
| Project 5 | 1.200 | 164000 | 2015 | $ 614.000.000.000 |
IV. Result
Field experiences, visits and interviews
The people and entities interviewed were, a technical project manager for construction (mechanical engineer), a construction company and a design company.
The interviewed parties gave details of the importance of knowledge and specialization to build hospitals, since these require a more detailed management as opposed to the construction of houses or buildings. In addition, it was found that the construction companies do not have this specialty in Colombia.
An investigation of construction and design costs of hospitals and clinics of level 3 in Colombia was carried out, in order to obtain an estimated average of the value of square meter.
Each of the data obtained was taken to the net present value by means of calculation to IPC for the corresponding periods that represent the inflation in that period. The calculation of the CPI for Colombia is done monthly in the National Administrative Department of Statistics (DANE).
This information was obtained thanks to the collaboration in some cases by project managers and others by means of web research.
Design:
The average value per square meter for design is $ 162,693, with a variance of 1397783576 and therefore a standard deviation of $ 37386.94; According to a renowned company in the architectural sector, the estimate value is between 3% and 5% of total project costs.
Table 4 Average cost of construction of square meter for hospitals of 3 level of complexity
| Project | Square meters | Year | Cost (COP) | VNA 2016 (COP) | Square meter cost (COP) |
|---|---|---|---|---|---|
| 1 | 50000 | 2016 | $ 5.034.341.351 | $ 6.959.735.557 | $ 139.195 |
| 2 | 72000 | 2013 | $ 13.687.000.000 | $ 15.513.217.935 | $ 215.461 |
| 3 | 20000 | 2014 | $ 2.400.000.000 | $ 2.668.457.184 | $ 133.423 |
| Average | $ 8.380.470.225 | $ 162.693 |
Construction:
The average value of construction per square meter is $ 4,505,520 COP, which corresponds to $ 1,454 US with a conversion rate of $ 3,100 COP which has concordance with the value found in the literature in Table 1; Table 5 shows the average cost of construction per square meter.
Table 5 Average VNA cost of square meter for third level complexity hospitals
| VNA 2016 (COP) | Square meters cost (COP) | Square meters cost per beds (COP) |
|---|---|---|
| $ 306.025.341.004 | $ 4.781.646 | $ 1.020.084.470 |
| $ 317.357.081.520 | $ 2.885.064 | $ 634.714.163 |
| $ 375.410.000.000 | $ 5.363.000 | $ 917.872.861 |
| $ 148.018.800.000 | $ 5.482.178 | $ 1.129.914.504 |
| $ 658.576.400.000 | $ 4.015.710 | $ 548.813.667 |
| Average | ||
| $ 361.077.524.505 | $ 4.505.520 | $ 850.279.933 |
Proposal of Hospital’s design and construction model
The proposed model is applicable only to clinics or third level hospitals.
Model features:
Hospital by specialties, connecting pavilions and expansion capacity.
Hospitalary’s hotelery, places of relaxation, comfort of patients, family and personal.
Interconnection, free of architectural barriers.
Digital Hospital, technological platform that facilitates the connectivity, automates and makes the processes more efficient.
Sustainable architecture: Energy efficiency, natural light.
The proposed model is composed of four main phases: Planning, design, construction and development.
1. Planning
1.1 Consult required information, documentation and necessary regulations that meet the minimum requirements established to carry out the construction of hospital.
1.2 Decide type of hospital to build, number of beds, specialties and the city of implementation.
1.3 Study necessary budget, costs, personnel, payroll and estimate of necessary time that the project would last.
1.4 Demographic study, study of rate and causes of mortality in the population of interest, construction needs and future achievements.
2. Design
2.1. Medical and architectonic program composed by:
1 Doctor
1 Bioengineer
2 Architects
4 Engineers (civil, mechanical, electrical and gases)
1 Financier
2.2. Analysis of construction materials and finishes.
2.3. Design of individual areas, define dimensions and distribution of spaces.
2.4. Architectural Design and approval.
3. Construction
3.1. Physical construction of the hospital.
3.2. Technology Assessment, the following committees are responsible for:
Medical and bioengineer committee; Security levels, regulatory compliance (10%).
Technical committee: Endowment (30%).
Financial committee: resource optimization (60%).
3.3. Review of minimum requirements.
4. Development
4.1. Acquisition process.
4.2. Startup of the hospital with accompaniment of biomedical engineer that guarantees compliance of standards, state of the hospital and integral development of quality.
An average of different bids for actual projects was obtained and an estimate of the percentages involved in the project is obtained. Table 5 shows this decrease in addition to estimating a 10% increase in project costs for expenses that imply the over cost and the overtime at the end of project development.
Taking the costs for design and construction in different projects, an estimate of costs was made for the square meter for construction and design in a project, in addition to the time and the necessary personnel workers, hospital of third level of complexity, and an area of more than 50000 square meters with approximately 600 beds, the design time for this hospital would be 2 years with 12 people in charge of different process, the construction would take 3 years with 1000 people in the work, it is clarified that of the estimated value of the project must estimate 10% in time and costs to correct the costs and time involved in the work.
V. Discussion
As can be seen in the results of Table 2, the country with the highest construction cost per square meter is US, followed by Argentina and the lowest cost of construction is on Colombia, this shows the greater investment in the sector Health in the first 2 countries, in which we seek higher quality in their hospitals through the implementation of new concepts and acquisition of new technology, unlike in Colombia where the main objective in these projects is optimization resources.
The bioengineer has the ability to handle key parts in the development of the project such as the provision of medical equipment in the hospital and the administrative part of this project, for this he must have experience and knowledge of the regulations, which should be constantly trained In the field of materials, medical and non-medical technology to optimize processes and reduce costs during project development.
It can be clearly seen in Tables 4 and 5 that of the projects consulted the price of the dollar inflows drastically in its stages and there is a considerable increase in prices for the last years.
VI. Conclusions
Colombia is currently in bed deficit, a possible solution is to develop structured models of design and construction of hospitals that optimize and encompass greater capacity of attention to the population.
The planning of a project is the most important phase since it is what determines the scope of the institution in addition to the endowment that helps to meet the objectives planned by the health center.
Is concluded with the research carried out on projects within reach, that the cost of square meter of construction is $ 4,505,520, and the design $ 162,693.
The Bioengineer is called to participate more formally in this type of hospital projects because it has the capacity to optimize processes of acquisition, management of technological devices and to manage in its totality the project having experience in similar projects.
Promoting research in hospital engineering is fundamental to increase public information in this type of projects and thus have more sources of knowledge.
It is important to know the costs of the average square meter in hospital construction and design in Colombia in order to compare them with respect to the costs handled in other countries and in this way to know how good the models are handled in those places and achieve Propose a suitable model that improves the shortcomings of the current design and construction.
The bioengineer is a professional called to investigate in appropriate forms of design and construction of hospitals to optimize costs and time to carry out these projects apart from knowing the world situation regarding the health sector to bring constant improvement to their environment.

