











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Currently, older adults are susceptible to obesity-associated cardiovascular diseases, which are risk factors for developing frail elderly and decreasing their functionality (1). The functionality of older adults is altered in the frail elderly, which decreases their strength, endurance, and physiological functions, causes vulnerability, disability falls, long-term care, and mortality. Frail elderly have unintentional weight loss, low functional capacity, exhaustion, weak gripping force, and slow running speed (2).
Functionality promotes a better quality of life in older adults and is related to necessary daily life activities such as dressing, using instruments (phone, money), and performing advanced tasks (travel planning). Better quality of life is associated with functional capacity, normal nutritional status, lower comorbidity rate, and fewer locomotive or psychological problems (3, 4). Functionality is related to the quality of life and social participation. Functional capacity and social relations between the elderly are necessary (5). Functionality decreases with sarcopenia, which is an accelerated loss of skeletal muscle mass and strength, and is associated with multiple adverse outcomes such as falls, multimorbidity, deterioration of quality of life, disability, and mortality (6, 7). Similarly, obesity with sarcopenia has an increased risk in older adults. It is the combination of both entities, with a fat mass more significant than 37% in men or 40% in women (8), which pose a more significant challenge for geriatric rehabilitation and improved functionality.
Older adults’ functional capacity prevents cardiovascular, musculoskeletal, and cognitive impairment and improves aging impairment functionality. The programs developed are conservative in intensity, power, volume, and training (9, 10). Continuous moderate-intensity training significantly improves body weight, subcutaneous body fat, fat distribution, lipid profile, and glucose control. In older adults, high-intensity exercises promote increased cardiovascular capacity, muscle hypertrophy, and bone density. In turn, high-intensity interval training is more effective, faster, and has a more significant effect (11). To improve body mass index and bone mineral density in older adults, researchers recommend performing strength training exercises for 30 minutes, three times per week, with three series of 8–10 repetitions, with breaks of 1–2 minutes between series, with a load of 70% and 85% of 1RM, accompanied by cardiovascular resistance training three times a week for 30 minutes at the intensity of 70–89% of the reserve heart rate (12). In addition, resistance training has benefits for cardiovascular health, weight management, prevention of disability and falls, because the loss of muscle mass and strength is a determinant of functionality and reduction of quality of life (7).
In turn, nutrition is a fundamental part of treating a patient who is considered fragile. Malnourished and frail elderly are not the same entity. With age, there is a decrease in energy intake, secondary to a decrease in functional capacity, along with weight loss, at the expense of muscle mass and functional deterioration, which are fundamental points in the concept of sarcopenia. It is mostly the supply of proteins that allows to reverse malnutrition, in which anabolic resistance is predominant and accompanied by insulin resistance and endothelial dysfunction. For muscle synthesis, it is essential to reach an amount of protein intake of at least 1.2–1.5 g per kilogram of weight per day, with an adequate proportion of essential amino acids (8). Therefore, this study aimed to “determine the most effective planning of exercise and nutrition to improve functionality in older obese adults.”
Materials and Method
This systematic review respects the PRISMA declaration and Cochrane collaboration. The PICOS strategy was adopted and delimited the study’s scope. Population: aged, obese; intervention: exercise, diet; comparison: control groups; result: frail elderly; design: a randomized controlled trial.
The inclusion criteria for the article search were: 1. Population over 60 years of age with obesity was assessed by body mass index or fat mass percentage; 2. Results in functionality; 3. Clinical trials with a control group; 4. Study with exercise and nutrition; 5. Language of articles: Portuguese, Spanish, and English; 6. Publications until September 2020. The exclusion criteria were: 1. Absence of relevant information in the study; 2. Unsuitable design when reading the full text; 3. Data duplicated by the same author; 4. Displays inadequacy when reading the full text; 5. Unsuitable intervention when reading the full text; 6. Body mass index or incorrect fat mass percentage.
Search for studies: the research team searched until September 2020 by tracking summaries and articles in the databases (Pubmed, SciELO, BVSALUD, Medline/PMC, Science Direct, and Sport Discus/EBSCO Host). The following combination of terms (MeSH) was used: Population: aged, obesity; Intervention: exercise, diet; Results: frail elderly; Design: a randomized controlled trial.
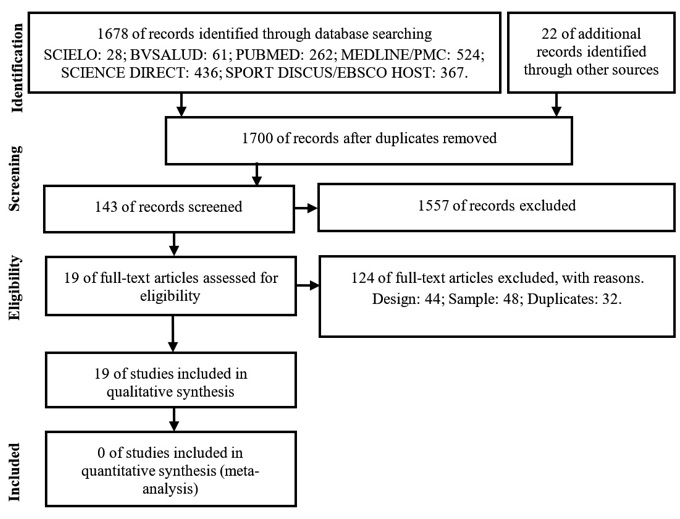
Study selection: The research team reviewed the titles and summaries by applying the inclusion criteria. Figure 1 shows the grounds for exclusion. Participants: older obese adults, verifying ethical compliance with research. Intervention: structured body movements that increase energy expenditure, practiced systematically (frequency, intensity, and duration), designed to maintain or improve health and supervised by health professionals, with cardiorespiratory or strength exercises, associated or not with a nutritional regimen, focused on energy or protein ratio, changes in macronutrient profile or proportion of additional macronutrients (mainly proteins and amino acids), in the form of whole foods orally.
Results measures: search for differences in operating averages, physical work, functional independence, geriatric assessment, activity rate, cardiorespiratory capacity, running speed, balance, gripping force, or leg strength (8).
Evaluation of the quality of the studies: a scale of 11 items “Physiotherapy Evidence Database” for internal validity of clinical trials and statistical information. Studies with scores equal to or greater than five can be considered to be studies of high methodological quality and low bias risk.
Data extraction: the research team reviewed the full text by extracting the data and performing the synthesis. The main result was the effect on functionality, including its standard deviation, with the descriptive characteristics of the article (year and sample), the characteristics of the interventions and the results.
Qualitative analysis of the data: the results of the studies were examined, presenting them in a summary table, looking for the means with their standard deviation, which presented statistical significance, in tests that measure functioning, physical work, functional independence, geriatric assessment, activity index, cardiorespiratory capacity, running speed, balance, gripping force, or leg strength.
Results
Characteristics of the studies: 1700 articles were identified by applying the selection criteria. A total of 19 studies met the inclusion criteria. Figure 1 shows the flowchart and the selection of studies, according to the PRISMA statement (13-31).
Characteristics of the participants: Table 1 presents 19 studies, with a total of 1310 participants. Fifty-seven per cent of the studies use body mass index to assess the nutritional status of older adults. The average body mass index of the elderly involved was 33.0 ± 3.8 kg/m (2).
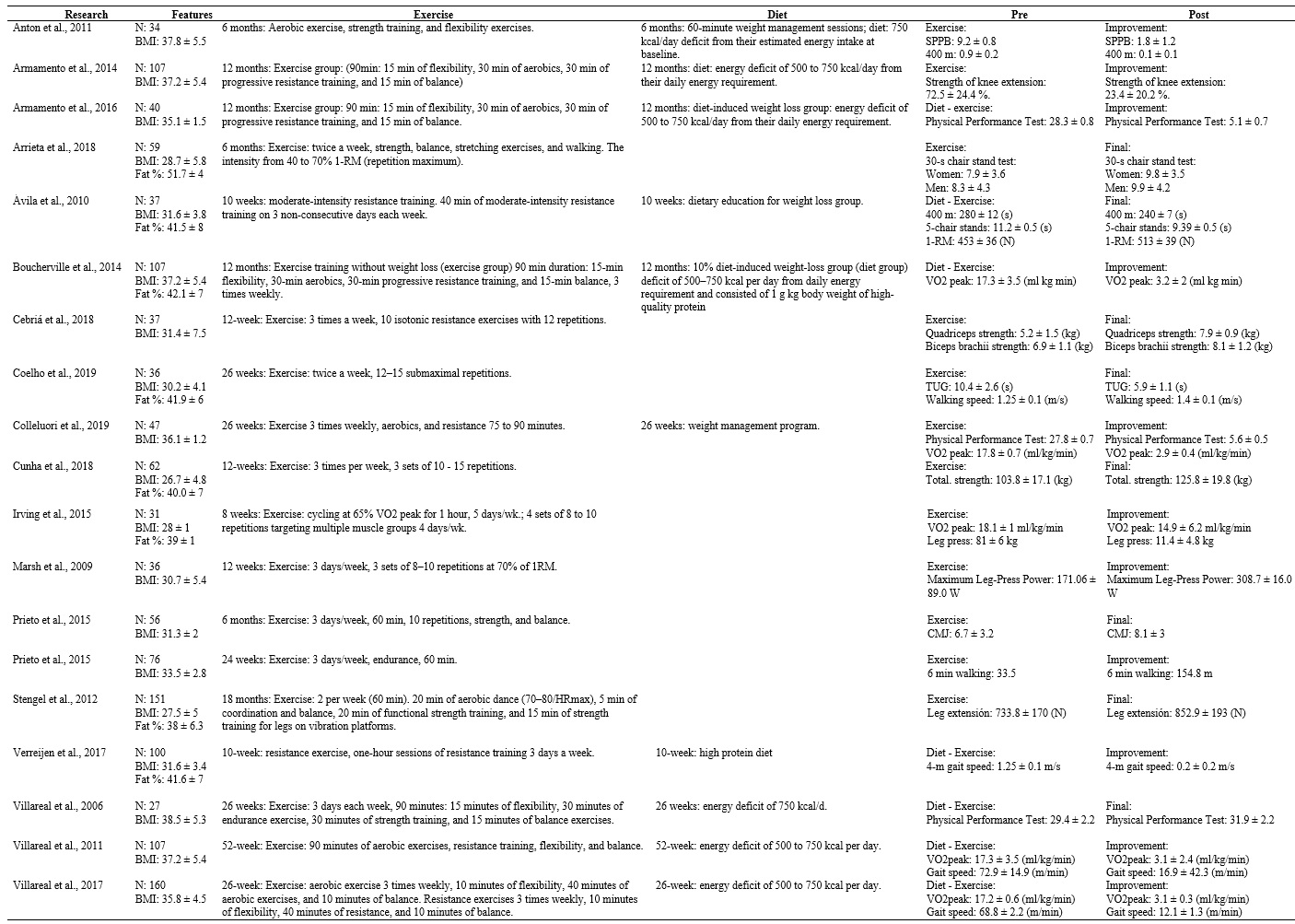
Characteristics of the interventions: The exercise regimen lasted for 8–78 weeks. Fifty-seven per cent of the studies use multi-component exercise to intervene with older adults (i.e., aerobic exercise, endurance exercise, balance exercise, and stretching). Thirty-seven per cent of studies use caloric restriction as nutritional intervention.
Description of the quality of the studies: Table 2 presents the evaluation of the studies, presenting a moderate methodological quality (PEDro 7.1 ± 1.1). The lowest scores on the PEDro scale in the analyzed research are obtained for the method of producing blindness of researchers concerning the subjects they were treating or evaluating, administering the therapy, and measuring a key outcome.
Table 2. Evaluation of the quality of the studies
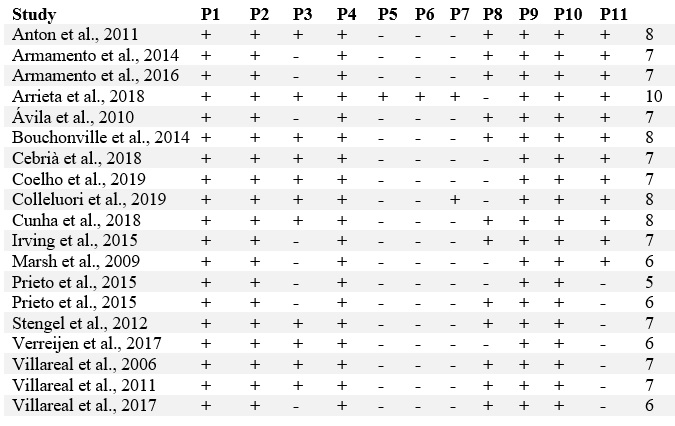
Notes:1. Eligibility criteria were specified; 2. Subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received); 3. Allocation was concealed; 4. The groups were similar at baseline regarding the most important prognostic indicators; 5. There was blinding of all subjects; 6. There was blinding of all therapists who administered the therapy; 7. There was blinding of all assessors who measured at least one key outcome; 8. Measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups; 9. All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat;” 10. The results of between-group statistical comparisons are reported for at least one key outcome; 11. The study provides both point measures and measures of variability for at least one key outcome.
Estimating the effect of exercise and nutrition: The 19 studies included in the qualitative analysis have different and heterogeneous results. Therefore, it is not possible to perform statistical analysis with meta-analysis. Therefore, a qualitative analysis of the articles was performed, and the results are presented in a summary table.
Discussion
This study aimed to determine the most effective exercise and nutrition planning to improve functionality of older obese adults. In our study, owing to an increase in life expectancy, it is necessary to assess older adults’ physical and functional capacities. A decrease in functional capacity predicts mortality, increased hospital income, and decreased quality of life (32). In the literature, there are different tests to evaluate functional capacity. It is possible to choose those that best fit the population to be evaluated. It may even be necessary to use several of them in combination to perform a complete study. Our review describes different results that are related to functionality and recommends to use the Short Physical Performance Battery (SPPB), a test used in geriatrics that allows to evaluate a greater number of patients with a decrease in their functional capacity and who are challenging to evaluate with other physical fitness tests (32).
The aging process is often associated with a deterioration in functional capacity, which can often cause problems in daily activities and lead to dependence. The help of another person is required to perform them. Therefore, we use different measures in our review to evaluate the results of interventions in older adults to assess the change in functionality. Functional ability is a combination of daily, raw, instrumental, and advanced activities. Daily activities may include getting up/lying down, maintaining body posture, walking or moving inside the house, walking or moving out of the house, moving in transportation, washing/showering, combing/cutting nails, controlling the need to urinate (bladder control), controlling the need to defecate (bowel control), dressing, eating, shopping, preparing food, and performing household chores. Therefore, these activities are essential in a geriatric evaluation and depend on the older adult’s physical condition related to health, i.e., body composition, cardiorespiratory capacity, strength, muscle endurance, and flexibility. Disability problems often start with instrumental activities, which are more complex and require more significant effort and skill to execute. They often end up in those necessary activities that are easier to execute but involve a more significant care burden. Therefore, our results include different measures to evaluate functionality such as the strength of the lower limbs or the gripping force of the upper limb (33).
In turn, frail elderly have a vulnerable situation that increases the likelihood of adverse health outcomes (34). It is closely related to age and the consequent loss of functional capacity. Therefore, it is a syndrome that may be present in older adults. It is also associated with significant health implications because fragile people have a high risk of institutionalization, hospitalization, disability, and death. SPPB is a validated and standardized test that combines balance, speed of travel, and the test of getting up from the chair (35). It is validated for the frail elderly in primary care and has high reliability in predicting disability. A score of 10–12 is non-fragile, 4–9 is fragile, and 0–3 is disabled. We recommend using this evaluation in older adults to define exercise-based intervention. Speed of travel is the most common objective functional limitation assessment test. In longitudinal studies, it has demonstrated the ability to predict adverse events such as hospitalization, frail elderly, falls, dependence, and mortality; it is also a component of the frail elderly phenotype. Running speed greater than 1 m/s is standard, while values between 0.8 and 0.9 m/s indicate pre-frail elderly, and values less than 0.8 m/s indicate frail elderly. Therefore, SPPB is a valid test for determining exercise prescription programs with an individualized prescription according to the functional capacity and monitoring of the subject over time; the disadvantage is that its realization requires more time and greater patient collaboration (34). In patients with Alzheimer’s disease, 6 weeks of aerobic, strength, balance and coordination exercises improve fat mass, muscle strength, balance, and fall prevention. In our review, 57% of the studies use multi-component exercises and show improvements in the functionality of obese elderly (36).
Nutritional recommendations for older adults are to maintain the calorie balance to reach and maintain a healthy weight and to limit the intake of sodium, solid fats, added sugars and refined cereals. In addition, the focus should be on consuming nutrient-rich beverages and foods such as milk and dairy products, lean poultry and meats, eggs, legumes, nuts, and seeds. Likewise, it is necessary to consume vegetables, fruits, whole grains, milk, and dairy products to obtain more potassium, dietary fiber, calcium, and vitamin D. Similarly, it is essential to consume a wide variety of vegetables (e.g., dark green, red, and orange), beans, and peas. At least half of all cereals in the diet should be in the form of whole grains. Thus, our review concludes that the consumption of these foods, together with caloric restriction and suppression of high energy-power foods, is the most useful nutritional intervention in older obese adults (37). Nutrition professionals should perform these nutritional interventions to avoid health consequences for the obese elderly.
Changes in body weight and composition have implications for the health status and functional efficiency in advanced age populations (38). These changes include decreased fat-free mass, bone mineral density, and increased fat mass as age progresses. Older people with excess fat have an increased risk of knee osteoarthritis, sarcopenia, physical deterioration, reduced quality of life, and present risk factors that are commonly associated with coronary heart disease, stroke, and other disorders such as dementia. Cossio et al. have indicated that the body mass index is a predictor of fat in old age, with a variance between 79% and 80% and a standard estimation error of less than 3%. Therefore, this review used body mass index and fat percentage to assess the nutritional status of older adults (38).
Fitness assessment is essential in promoting functional capacity and health because it can identify people who are at risk for chronic diseases and the frail elderly (39). Physical performance decreases with age mainly due to deterioration of aerobic endurance, flexibility, strength, speed, agility, and balance. Therefore, for older obese adults, we recommend multi-component exercises accompanied by caloric restriction, which is reflected in most of the results of this review, with interventions ranging from 8 weeks to 78 weeks. It is necessary to plan and distribute training loads by following the principles of training in search of improving the physical and functional performance of older adults (39).
The population of Latin American has increased. Because functionality is critical to the quality of life, preventing and reversing dependence should be the priority of the public agenda. Therefore, this review outlines exercise and nutrition plans for older obese adults (40).
In Colombia, research using SPPB established benchmark values for Colombian seniors living in the community. The evaluation of physical function with SPPB (provides information on the functional decline of elderly people). It also allows to evaluate the effect of interventions on the functional state of the elderly. SPPB is calculated based on the time required to complete a 4-meter walk, time to get up from a chair five times, and the ability to stand up to 10 s in three different ways. This evaluation can detect ≤9 points between vigorous and fragile people. This approach has been validated in studies in Brazil and Colombia. In this study, the SPPB score was 8.7 (2.0) points and suggests that age, body mass, height, body mass index, and leg perimeter contribute to gait speed (p < 0.001) after controlling for confusing factors including ethnicity, socioeconomic status and urbanity. Therefore, the diet, health status, race, and geographical location of Colombian populations, in general, greatly affect anthropometric and physical performance. We encourage the use of this test in experimental studies with the elderly to analyze the results. In our study, the evaluation of studies is heterogeneous. Using SPPB, the meta-analysis of results provides more information (35).
This approach evaluates the effectiveness of nutrition and exercise on body composition and strength in older adults with obesity and sarcopenia. In only two trials with 61 participants, with nutrition of 15 grams of protein per day (cheese consumption) and resistance training with high-speed circuits, it was determined that exercise improves muscle strength. In our study, caloric restriction and multi-component exercise improved functionality in obese older adults. However, protein intake needs to be considered to improve muscle protein synthesis in obese older adults to improve functionality. Our review includes a healthy protein intake of 1 g/kg plus multi-component exercise, improvements in cardiorespiratory capacity, high protein consumption, endurance exercises, and walking speed improvements (41).
Future research should focus on aging, frail elderly, cognitive decline, and improving functionality, disability, and quality of life, with multidomain exercise interventions, nutrition, and cognitive training, improving the functional decline and quality of life of older people (42). In addition, the results of our research indicate that inequalities in older adults, between men and women, depending on the economic status, access to public services, family environment, and health conditions should be considered in Latin America to improve living conditions and health of aging people because these methodologies must be available to all older adults in public service and primary care (43).
The limitation of our research is the language due to the lack of accurate translations that allow us to evaluate and analyze other databases. Another limitation is that functionality is a complex variable, and different evaluation methodologies are used. We propose to use SPPB to evaluate functionality in obese older adults, which would make it easier to perform a meta-analysis to obtain quantitative results. We use qualitative analysis due to the heterogeneity of tests used to evaluate functionality in older obese adults.
Conclusion
Our work allows us to conclude that multi-component exercises and caloric restriction provide benefits for older, obese adults and improve their functional capacity. We hope that these results will help plan and structure exercise for primary care of older adults. In addition, we note that caloric restriction is a strategy that can be used in older obese adults. However, additional studies on older, obese adults with sarcopenia are needed to analyze nutritional interventions in these patients.

