











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Overweight or obesity refers to the abnormal or excessive accumulation of fat that can put a person at greater risk and harm their health (1). In relation to the classification of overweight and obesity proposed by the World Health Organization, the cut-off point to define overweight is a body mass index (BMI) value between 25 and 29.9 kg/m², and for obesity a BMI value ≥ 30 kg/m² (2,3).
Obesity affects people of all ages in both developed and low/middle-income countries, regardless of socioeconomic status (4,5). In 2016, more than 1.9 billion adults were overweight worldwide, of which more than 650 million were obese. Overweight represented 39% (39% of men and 40% of women) and obesity 13% (11% of men and 15% of women) (6).
Obesity is considered a disease that requires attention, in order to prevent premature death, as it has been identified as a risk factor for a number of diseases such as type 2 diabetes, arterial hypertension, heart disease, stroke, cancer, sleep apnea, etc. (3,7). On the other hand, overweight and obesity have been associated with excessive alcohol consumption, smoking and sedentary lifestyle habits (8).
Few data are available on the effect of excess weight on sexual function. However, it has been hypothesized that overweight/obesity has a negative impact on sexual function through hormonal, metabolic, and psychological parameters (9,10).
The Female Sexual Function Index (FSFI) is currently considered the best tool for assessing sexual function in women because it is consistent and reliable for screening sexual dysfunction in women of all ages (11). It is characterized by being self-administered and validated in several languages. It has six subcategories: desire, arousal, lubrication, orgasm, satisfaction and pain (12).
There are few studies on the impact of obesity on sexual function in women, and none have been identified in Colombia. Therefore, the aim of this study was to evaluate the prevalence of sexual dysfunction in women with obesity of reproductive age in Quindío, Colombia, in order to establish a first approximation to the magnitude of this problem in the country.
Materials and methods
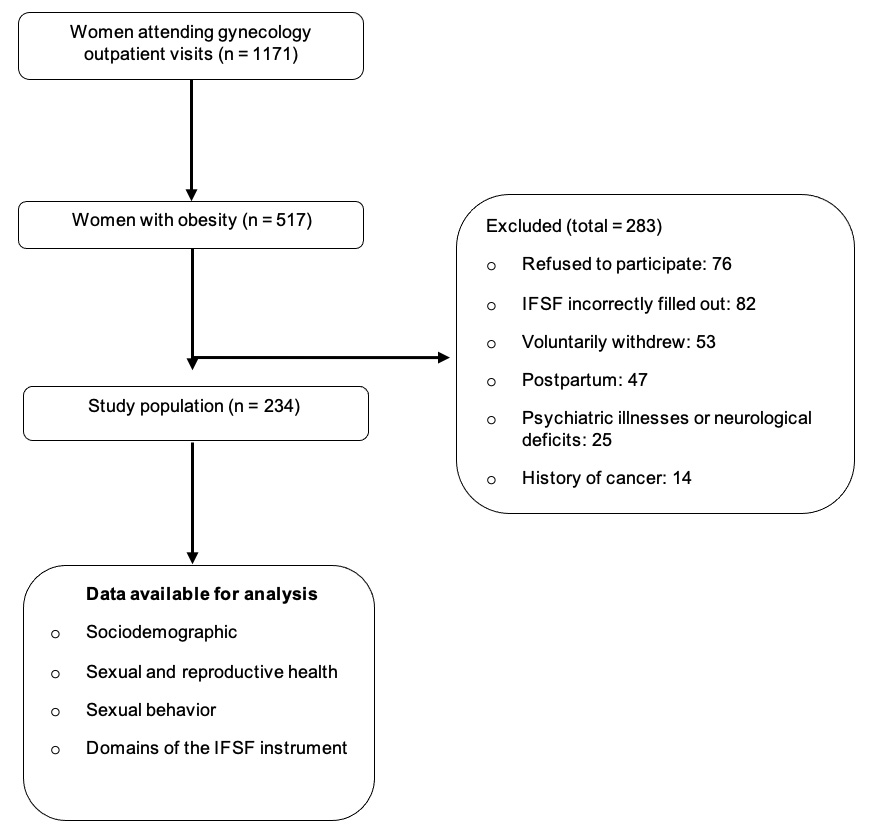
Design and population. A cross-sectional study was conducted which included women with obesity older than 18 years and younger than 40 years, who reported having had sexual activity in the last six weeks, with stable partner and residents of Quindío, who attended outpatient clinic in a private clinic, tertiary care university institution that serves population belonging to the contributory and subsidized regime in the General System of Social Security in Health in Colombia, between March 1, 2016 and February 28, 2019. Women who were pregnant or in their first six months postpartum, with psychiatric illnesses or neurological deficits, history of sexual dysfunction, mental retardation, history of cancer, low level of schooling (situations that did not allow the correct understanding or completion of the IFSF instrument) and those who did not wish to participate were excluded.
Sample size and sampling. A sample size of 203 women was estimated, based on a precision of 3%, a confidence level of 95% and an expected proportion of 5%. Simple random sampling was performed using a table of random numbers.
Procedure. Participants were identified from the gynecology outpatient clinic. Women with a confirmed diagnosis of obesity were invited to the study. Once the selection criteria had been verified, and after signing the informed consent form, a questionnaire was completed in which the sociodemographic and clinical characteristics of the women were recorded. Two nursing assistants, in charge of collecting the standardized instrument, gave each woman instructions for self-completion of the IFSF questionnaire, individually and in private. One of the nursing assistants collected the data and entered the information in a database developed in Excel® 14.0 (2011). The database was verified by a professional nurse specialist in health auditing.
The IFSF is a 19-item questionnaire that assesses six domains: desire (items 1 and 2), arousal (items 3 to 6), lubrication (items 7 to 10), orgasm (items 11 to 13), satisfaction (items 14 to 16), and pain with sexual activity (items 17 to 19). The response is measured according to the following score: 0: no sexual activity; 1: almost never; 2: less than half the time; 3: half the time; 4: more than half the time; and 5: almost always. The score for each domain is multiplied by a factor ranging from 0.3-0.6, considering the domain evaluated. In the end, the result is the arithmetic sum of the domains: the higher the score, the better the sexuality. The total IFSF score ranges from 2 to 36; a score ≤26.55 points, or when the score for any domain is less than 3.6 points, is considered a criterion for risk of sexual dysfunction (12-14).
Variables measured. The demographic variables evaluated were: age, race, marital status, level of schooling, socioeconomic stratum, type of social security (subsidized or contributory), occupation, religion and origin; habits (alcohol intake, smoking, psychoactive substance use, sedentary lifestyle); sexual and reproductive health variables: age of menarche, age of sexual debut, contraceptive use in the last year, sexual orientation, parity; sexual behavior: intercourse (vaginal or anal), oral sex, masturbation, average frequency of sexual intercourse per month, use of erotic toys, number of sexual partners, length of cohabitation, history of sexual abuse or sexual violence in marriage, partner with sexual dysfunction. The questions of the domains of the IFSF instrument were also evaluated.
Statistical analysis. Categorical data were analyzed using absolute and relative frequencies (percentages and proportions), and quantitative data were analyzed using measures of central tendency and dispersion —mean and standard deviation (SD), (minimum and maximum), median (range) —. The distribution of the data was evaluated using the Shapiro-Wilks test. The Wilcoxon test was used to compare two medians related to the same sample. The significance level was set at a p value <0.05. The analysis was performed with the SPSS Statistics 17.0.2 (2009) software. The results are presented in a grouped manner for the total population. The prevalence of sexual dysfunctions is presented globally and by IFSF domains.
Ethical aspects. The research was approved by the Ethics Committee of the participating institution, in accordance with Resolution 8430 of 1993 of the Colombian Ministry of Health, and complies with the guidelines of the Declaration of Helsinki of the World Medical Association on Ethical Principles for Medical Research Involving Human Subjects. Confidentiality of information and patient privacy were guaranteed.
Results
A total of 517 (44.15%) women with obesity, potentially candidates to be part of the study, were recruited; of these, 76 (14.7%) refused to participate, but for the final analysis a total of 234 (45.26%) forms were taken into account (Figure 1).
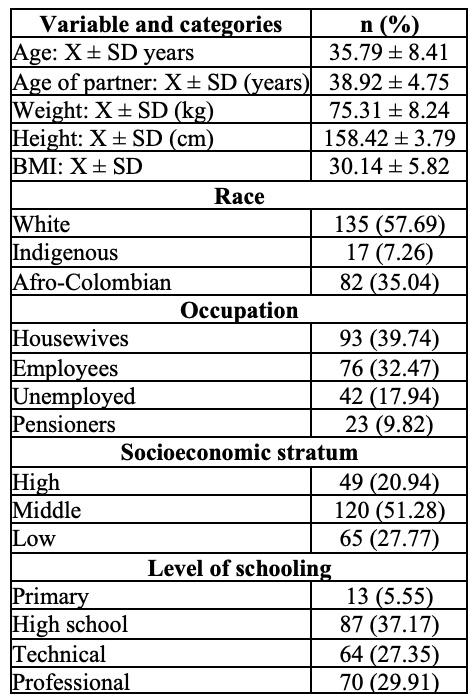
The mean age of the total population was 35.79 ± 8.41 years (minimum: 18 and maximum: 39). BMI reached a mean of 30.14 ± 5.82, and type I obesity predominated with 30.76%, with type IV (extreme) obesity being the least frequent, with 7.69%. Catholic religion was professed by 90.17% of them. 87.17% belonged to the contributory Social Security health system, 78.63% resided in urban areas, and 56.83% lived together with their partners. The sociodemographic characteristics are described in Table 1.
Table 1 Sociodemographic characteristics of women with obesity and sexual dysfunction in Quindío 2016-2019
In sexual and reproductive health history, the mean age of menarche was 11.27 ± 1.58 years. The mean age at the onset of sexual activity was 16.83 ± 2.45 years. The mean age at first childbearing was 19.75 ± 3.58 years. A median of 3 children (range 0 to 7) was found at parity. 71.79% had had more than two children and 62.82% had been pregnant more than three times. 81.19% used contraceptive methods, with a predominance of hormonal contraception (77.89%), with the pill in the first place (65.78%), followed by the implant (17.89%) and the intramuscular injection (6.84%).
Regarding habits, 15.38% were regular smokers (median of 5 cigarettes per day, range between 1 and 15), 85.89% consumed alcohol and 6.41% used psychoactive substances. Sedentary lifestyle reached 62.82%.
In terms of sexual behavior, the median number of sexual partners was 7 (range between 1 and 11). 35.89% of the total participating population stated that they had lived with their partner for more than 10 years. 20.51% reported that the partner presented some sexual dysfunction. The sexual orientation of the population is predominantly heterosexual (93.58%). The most frequent sexual practice is vaginal intercourse (100%), and the least common is anal intercourse (17.94%). Masturbation is considered common practice by 71.79% of the participants. Regarding oral sex, there was no significant difference between cunnilingus and fellatio, 8.97% versus 6.41% (p>0.05). The use of erotic toys was observed in 26.92% of the participants.
To the question “How many times did you have sexual intercourse in the past month (period defined as the previous thirty days)?”, a median of 4 times per month was reported (range between 0 and 9). 57.69% of the total number of participants reported a median of ≤3 times per month.
19.23% of women reported having suffered some form of sexual violence in their lifetime, while 12.82% reported sexual abuse by their partner. 80.76% reported having been verbally abused by their partners because of their body shape. 87.17% reported having suffered social stigma due to obesity.
The preferred coital position of the participants was the rear entry (“doggy style” position), with 48.71%; followed by the reverse “cowgirl” (the man lying on his back, while she sits on his lap, with her back to him, while being penetrated), with 37.17%.
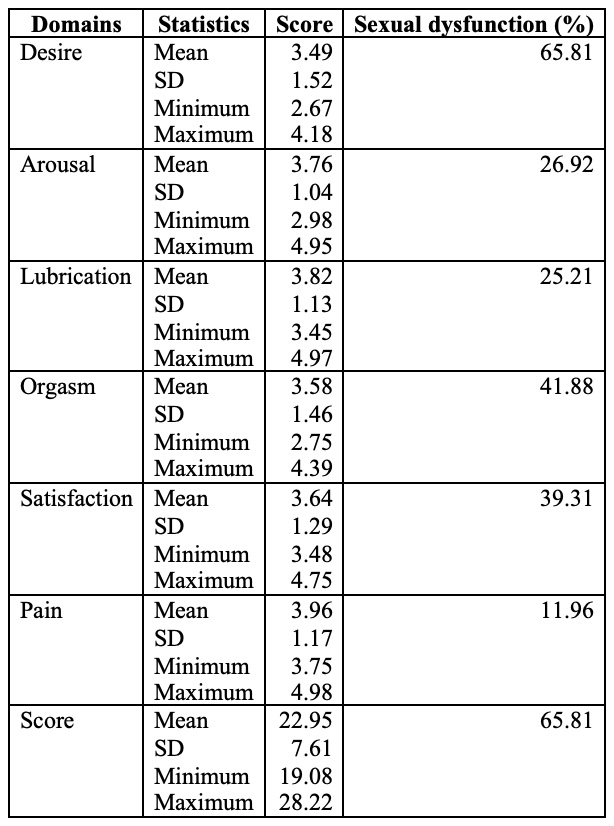
The average IFSF score in the total population was 24.07 ± 7.61 points (minimum: 19.08 and maximum: 28.22); while in affected women, it was 22.65 ± 6.18 points (minimum: 19.08 and maximum: 26.45). The prevalence of sexual dysfunctions in the total group reached 65.81% (n = 154/234), with alteration of desire (65.81%), followed by orgasm disorders (41.88%; n = 154/234) (Table 2). The median number of sexual dysfunctions in the group of affected women was 3 (range between 1 and 5). A total of 6.83% had one sexual dysfunction, 21.79% had two, and 71.36% had three or more.
Concerning orgasm disorders, 21.42% of the participants stated that they had never experienced orgasm, while the percentage of simulators was 38.77%. When asked about the frequency of orgasm, 12.24% said “always”, 35.71% said “at least half the time”, 29.59% said “more than half the time”; 5.12% of the total population said they were multi-orgasmic. 5.84% of women with sexual dysfunctions reported having attended a sexology consultation or sexual counseling, and 3.24% reported having received treatment for their sexual dysfunction at least once.
Discussion
In this research, a prevalence of sexual dysfunction of 65.81% was observed in women with obesity. Alteration of desire was found (65.81%), followed by orgasm disorders (41.88%) and sexual dissatisfaction (39.31%), as shown in Table 2. The median number of sexual dysfunctions in the group of affected women was 3, which was observed in 71.36%. The presence of only one sexual dysfunction was unusual (6.83%).
The present study contrasts with that by Kadioglu et al. (15), who reported that obesity has no significant relationship with the presence of sexual dysfunction, but found that women with obesity express a more depressive mood than their normal counterparts of the same age, which could become a factor in the deterioration of their sexual function. Similarly, Yaylali et al. (16) concluded in their study that, although obesity does not seem to be an important factor in the presence of sexual dysfunction, it does affect several aspects of sexuality.
In their research, Kirchengast et al. (17) state that reduced sexual interest is associated with a body type that does not correspond to society’s specific ideals of beauty. Kinzl et al. (18) indicate that many of the sexual problems in women with obesity are the result of an underlying lack of self-esteem, unsatisfactory relationships or collective stigmatization.
According to Kolotkin et al. (19), obesity is associated with lack of enjoyment of sexual activity, hypoactive sexual desire, difficulties with sexual performance, and avoidance of sexual encounters. In addition, they state that the quality of sexual life is more affected in women, in people with type III obesity and in patients seeking gastric bypass surgery.
In their review, Larsen et al. (20), in which they evaluated the relationship between sexual function and obesity, found no evidence to suggest that sexual dysfunction causes obesity. However, there was strong evidence to indicate that obesity caused sexual dysfunction, and this made it clear that there is a direct association between obesity and the presence of sexual dysfunction.
Body image, being the perception of one’s own body becomes an important component of self-esteem (21). In this regard, Lachowsky (22) has reported a positive correlation between body image and sexual function in a variety of population cohorts. Similarly, Seal et al. (23) show that body esteem is related to sexual responses to a standardized erotic stimulus, and particularly related to sexual desire. Thus, it can be deduced that there may be a link between body image and BMI (24), which affects both women and men, although women are more affected.
Although the relationship between sexual function and obesity is very complex, and although there are findings that support the association between these two variables, the reality is that there is little research on sexuality and the psychological impacts of obesity (specifically, anxiety, self-esteem, depression, stress, and body image) (25). Therefore, as described by Strain et al. (26), the interrelationship between body weight, mental health, and sexual function deserves further discussion and research, since in addition to improving mental well-being, reducing body weight appears to improve sexual functioning in people with obesity (27-30).
Regarding the positions preferred by the women in this study, at the time of intercourse (the “doggy style” and the reverse “cowgirl” position), the preference for these positions was attributed to “mechanical” reasons, since positional difficulties during intercourse affect patients with obesity, given the “physical problems of maneuverability”, which act as the main difficulty when it comes to sexual intercourse.
The main strength of this study is that it was the first to be carried out in Colombia and to have used the IFSF instrument, a recognized questionnaire of proven reliability and internal consistency, which is validated in Spanish. Among the limitations is that the IFSF questionnaire requires an adequate level of schooling to facilitate a proper understanding of the questions. Thus, it is not useful in illiterate populations or those with a low level of schooling, a situation that could lead to a bias in prevalence. In addition, 18.02% of the questionnaires were lost because they were incorrectly filled out, which could have affected the estimation of the prevalence of sexual dysfunctions.
Conclusions
A high prevalence of sexual dysfunctions was observed in obese women from Quindío, corresponding to two-thirds of the participants, characterized by alterations of desire, followed by orgasm disorders and sexual dissatisfaction. It is necessary to evaluate the effects of obesity in populations from different regions of the country and to implement interventions to know and mitigate its impact on the sexual function of women with obesity. Attention should be paid to the sexual problems faced by these patients to improve their quality of life.

