











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Intraoperative frozen section consultation has become an essential tool for making surgical decisions about treatment options, understanding whether a lesion is malignant or benign, ensuring the absence of tumor cells in the excision margins and identifying specific tissues (1). Intraoperative consultations must be done quickly in order to be useful for the surgeon’s decision process and to avoid unnecessary surgical procedures. Hence, it is recommended to send only samples that are representative for the frozen section (2).
Frozen section diagnosis is usually compared with the diagnosis of paraffin-embedded tissue, better known as permanent diagnosis, in order to determine diagnostic accuracy, evaluate discrepancies, identify deficiencies and solve associated problems, with the ultimate purpose of improving the quality of the intraoperative biopsy and diagnostic accuracy (3).
Many studies have reported the accuracy of biopsies from intraoperative consultation. However, in intermediate care institutions from medium-sized Colombian cities, there were no reports of this kind in our search; one study from Colombia was found, but it belonged to a tertiary care center (4). The objective of this study is to compare the accuracy of frozen section diagnosis in this institution with the results of other studies in the world and analyze the possible causes of discrepancy.
Materials and methods
The purpose and methodology of this study were approved by the Local Ethical Committee supported by the investigation program in genetic analysis of human diseases of the University of Tolima. All procedures and data collection were conducted in accordance with the Declaration of Helsinki.
A total of 417 cases in which frozen section was used between January of 2015 and November of 2019 in an intermediate care center were included in this retrospective study. From them, the following data were recollected: age of the patient, anatomic site, specimen size, histological results of the frozen section and the final report. The cases were classified in two categories: concordant and discordant. In addition, the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. Univariate analysis was performed in order to identify predictor factors for misdiagnosis in the general sample and in the ovary specimens. The data distribution was valued with X² and Fischer’s exact test. All the calculi were made with Vassarstats online software.
The literature search was performed in Pubmed using the criteria “frozen section” and “concordance”, and 277 articles were found. The search was confined to the last five years (89 articles), then filtered by “humans” and in English with full text available (54 articles). After reading the abstract, it was reduced to 9 articles that could be compared to this study, including the results of sensitivity and specificity for malignancies in different anatomical sites.
Results
From the 417 cases, 395 were female and 22 were male; the most frequent anatomical site of extraction was ovary with 300 cases, the median age of the sample was 50 years, and 276 of the total specimens were less than 10 cm in size; the clinical accuracy values are shown in Table 1. There were no false positives for malignancy, giving a 100% in specificity; borderline tumors had the worst accuracy (sensitivity: 72.7%; PPV: 61.5%); benign tumors did not present false negatives. Sensitivity for malignant neoplasm was 88.9% in our study.
Table 1 Diagnostic accuracy of frozen section
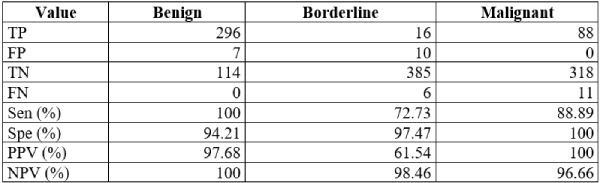
TP: true positives; FP: false positives; TN: true negatives; FN: false negatives; Sen: sensitivity; Spe: specificity; PPV: positive predictive value; NPV: negative predictive value
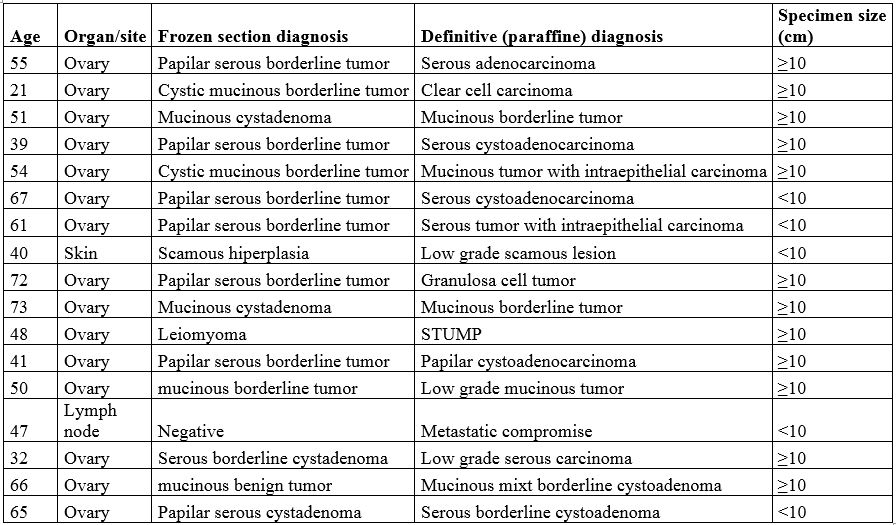
The attributes of the 17 discordant cases are shown in the Table 2. All of the discordant cases were female, the anatomical site for 15 of these cases was ovary and the specimen size was greater or equal to 10 cm in 12 of the cases.
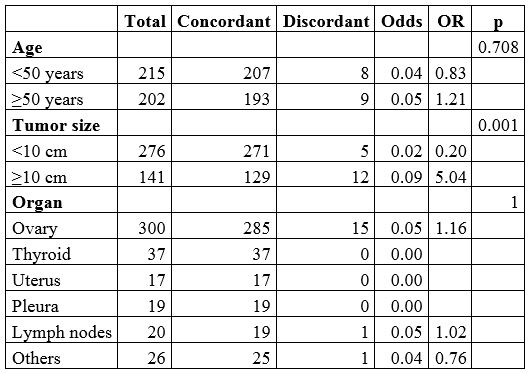
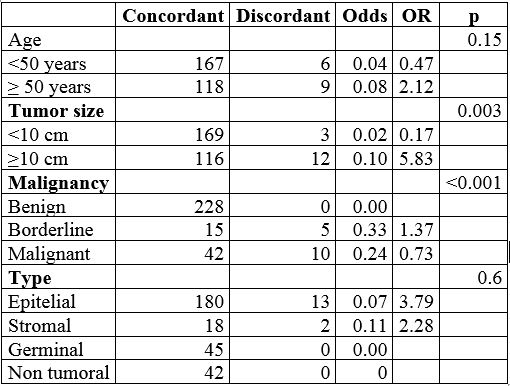
The univariate analysis for the general sample is shown in Table 3; it shows an association to misdiagnosis in age ≥ 50 years (OR = 1.21) and specimen size ≥ 10 cm (OR = 5.04). The specimen size showed more statistical significance (p = 0.001). In addition, the analysis showed a correlation with the anatomical size such as ovary (OR = 1.16) but with low statistical significance (p = 1). Table 4 shows the univariate analysis for the 300 ovary specimens. It revealed association to misdiagnosis in individuals 50 years or older (OR = 2.12; p = 0.15), size ≥10 cm (OR = 5.83; p = 0.003), borderline tumors (OR = 1.37; p < 0.001), and stromal epithelial histology (OR = 2.28 and 3.79; p = 0.6).
Possible biases include selection bias because ovary tumors are the most frequent cause of intraoperatory consultation in our center. There might be a bias due to the small sample size in the measurement of sensitivity and specificity.
Discussion
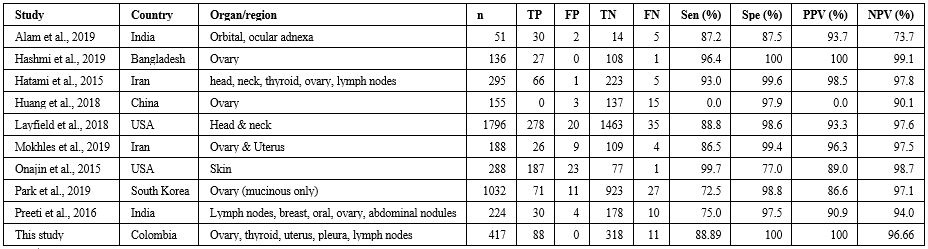
Frozen section is a commonly used tool for immediate diagnosis in multiple organs, but it has a particular widespread application in ovarian tumors, as shown in this study with a vast majority of cases with an ovarian origin. Therefore, the sample for this study was mainly female. The results of this study were compared with the results of other nine studies. The selected studies for comparison are shown in Table 5. The sensitivity for malignancy in this study varied from 99.7 to 72.5% (5,6). Interestingly, in four of the other studies, the main organ sampled was ovary (6-9). In one of these, the specificity and PPV was 100%, giving equal results as this study. One study did not present true positive cases for malignancy because its main focus was borderline tumors. Another study with low sensitivity was performed by Park et al. with a sensitivity of 72.5%. However, it only included mucinous tumors (6). The diagnostic accuracy of frozen section in this study had high values for malignant and benign lesions presenting flaws in borderline lesions, causing 10 cases of under-diagnosis, the sensitivity for malignancy is similar to the mean sensitivity in the studies listed in Table 5.
There are different factors that can be correlated with misdiagnosis in frozen section. This study showed an association with patient’s age ≥50 years and misdiagnosis with medium statistical significance. On the other hand, a larger specimen size (≥10 cm) correlates with misdiagnosis in addition to high statistical significance for both the general sample and the ovary cases. This agrees with previous studies (8). The anatomical site of extraction of the samples was not significant in this study. The tumor type in ovary as stromal or epithelial tumor were associated with misdiagnosis in a medium statistical significance. Other studies have shown that some histological types of tumors are more likely to be misdiagnosed. For example, ovarian clear cell carcinoma may be confused in first instance with borderline serous tumor (10). One of the discordant cases in this study had this characteristic. Mucinous tumors are the most frequently misdiagnosed type of tumor. (6). The misdiagnosis in stromal ovarian tumors has also been reported to be frequent (11). Another tumor characteristic related to misdiagnosis is borderline malignancy, with a high statistical value. Many studies also confirm this to be an important factor leading to discordances between frozen section and definitive diagnosis (12-14).
The importance of intraoperative consultation using frozen section comes from the fact that some tumors can only be diagnosed through surgery, mainly ovarian neoplasms (15). Thus, frozen section diagnosis becomes a guide for the surgeon, and studies report that it is an accurate modality for this purpose (16). Although the most common discrepancies occur between borderline tumors and real malignancy, fortunately this issue does not affect its usefulness as a guide in the choice of surgery, since to a large extent intraoperative treatment in borderline and malignant ovarian tumors includes bilateral salpingo-ophorectomy and appendectomy, and fertility preservation procedures are not performed in any of these tumors (15).
In conclusion, pathological diagnosis by frozen section has been and will continue to be the best tool for rapid diagnosis in intraoperative consultation, even though it may have its flaws in specimens that are too large or have specific characteristics for certain tumors and patients. The results of this study showed concordance with previous findings, in which the inaccuracy tend to be about diagnosis details more than in general diagnosis of malignancy, an event that does not usually impair surgical practice and the prognosis of the disease.

