Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkInternational Journal of Psychological Research
Print version ISSN 2011-2084
int.j.psychol.res. vol.7 no.2 Medellín July/Dec. 2014
Research
Dental anxiety in relation to aggressive characteristics of patients
Ansiedad dental en relación a las características agresivas de pacientes
Carmela Mento a,*, Lara Gitto b,, Marco Liotta c,
Maria Rosaria A. Muscatello a, , Antonio Bruno a, and Salvatore Settineri c,
b CEIS Sanità, University of Rome "Tor Vergata", Roma, Italy.
c Department of Human and Social Sciences, University of Messina, Italy.
*Corresponding author: Carmela Mento, Department of Neurosciences, University of Messina, Psychiatric Unit, AOU Policlinico
"G.Martino", via Consolare Valeria n.1, 98124, Messina, Italy. Phone: +390902212978. Email address: cmento@unime.it
Article history: Received: 12-06-2014 - Revised: 15-07-2014 - Accepted: 01-08-2014
ABSTRACT
Dental anxiety is defined as the response to a stressful stimulus that is specific to a dental context. The dental treatment itself may provoke excitation and aggressive response relating to multiple sources of motivation that have been examined by the literature.
The hypothesis to test in the present paper is to what extent dental anxiety can be explained by looking at patients' characteristics solely or by considering latent aggressiveness that could be manifested before and during the dental treatment.
The results of the study should give some indications to dentists to better understand the presence of a greater or lesser anxiety associated with orthodontic treatment in order to provide an appropriate assistance and, eventually, to help patients in developing coping strategies. As a consequence, it should be clear how intervening on each component of dental anxiety and/or aggressiveness may have a positive impact on the outcome of dental treatment.
Key words: Dental treatments, Dental anxiety, Aggressive behaviour.
RESUMEN
La ansiedad dental es definida como la respuesta a un estímulo estresante que puede pertenecer a un contexto dental. El tratamiento dental puede provocar excitación y respuestas agresivas relacionadas a múltiples fuentes de motivación que han sido examinadas por la literatura.
La hipótesis a evaluar en el presente texto consiste en hasta que alcance la ansiedad dental puede ser explicada al observar solamente características del paciente o al considerar agresividad latente que podría ser manifestada antes y durante el tratamiento dental.
Los resultados de este estudio deberían dar algunas indicaciones a los dentistas para entender mejor la presencia de una mayor o menor ansiedad asociada a tratamientos ortodónticos para generar una asistencia apropiada y, eventualmente, para ayudar a los pacientes a desarrollar estrategias para superar tales dificultades.
Como consecuencia, debería estar claro como intervenir en cada componente de la ansiedad dental y/o agresividad podría tener un impacto positivo en el resultado de un tratamiento dental.
Palabras clave: Tratamiento dental, ansiedad dental, comportamiento agresivo.
1. INTRODUCTION
Dental anxiety is defined as the response to a stressful stimulus that is specific to a dental context. The notion of dental anxiety is common in the literature (Economou & Honours, 2003). It concerns two different interpretations: the first one sees anxiety as the expression of a normal anxious state, whereas, according to the second perspective, dental anxiety is a specific psychopathological condition (DSM, American Psychiatric Association, 1994).
According to the first interpretation of dental anxiety, oral procedures may provoke acute symptoms of anxiety such as excessive apprehension, irritability, tension and the willingness to avoid the treatment (Locker, 2003; Anttila, Knuuttila, Ylöstalo, & Joukamaa, 2006). More specifically, the dental treatment itself may cause excitation and aggressive response motivated by many causes: external objects, needles, noise of the drill, smell of teeth, etc. (Quteish Taani, 2002; Doebling & Rowe, 2000; Abrahamsson, Berggren & Carlsson, 2000; Van Toller, 1988).
In this study we assume that dental anxiety is a component of anxiety (Settineri, Mallamace, Muscatello, Zoccali & Mento, 2013).
We observed a random sample of patients undergoing dental treatment at several settings located in two regions in Southern Italy.
An econometric analysis has been run, considering, as dependent variable, the level of dental anxiety; patients' characteristics (gender and age) and single components of aggressiveness, as monitored by appropriate psychological scales have been included among the regressors.
The hypothesis to test is to what extent dental anxiety can be explained by looking at patients' characteristics solely or by considering also latent agressivness that could be manifested before and during the dental treatment.
2. METHOD
The presence of dental anxiety has been identified by administering the Dental Anxiety Scale (DAS) (Corah 1969; Corah, Gale & Illig, 1978). The scale contains 19 items and is divided into two parts.
The first part (DAS 1) is made up of six items: the first five items explore the traits of dental anxiety of the patient. The answers to the items are given using a score from 0 to 4, with a total range for this first part between 0 and 20. The total score defines a low anxiety level if it is lower or equal to 14 and a high level if it is equal or higher than 15, which is in line with Corah et al. (1978).
The item 6 of DAS 1 looks specifically at dental anxiety induced by specific stimuli using six items that include: injection needles (6a), drill noise (6b), pain of treatment (6c), the smell of teeth being drilled (6d), a feeling of suffocation/gagging/lack of air (6e), the reclined position of the dentist chair (6f). Each answer was scored from 1 to 7, where 1 = low anxiety, 7 = high anxiety.
The second part of the scale (DAS 2) contains 13 items and explores dental anxiety related to the relationship between dentist and patient. The score assigned to each item goes on a descending scale from 2 to 0, with a cumulative score range of between 0 and 26.
The use of the DAS allows the specific measurement of anxiety provoked by dental stimuli: this is demonstrated by its widespread use in the literature (Maggirias & Locker, 2002; Locker, Thomson & Poulton, 2001a; Locker, Thomson & Poulton, 2001b, Settineri et al., 2013).
The Aggression Questionnaire (AQ) (Buss & Perry, 1992) is a self-reported scale, assessing the feeling of aggressiveness. It considers two components: 1) a behavioral component, which is represented by the subscales of physical aggressiveness (PA), made of nine items (as an example: "Once in a while I cannot control the urge to strike another person"), and verbal aggressiveness (VA), made of five items (as an example: "I often find myself disagreeing with people"); 2) an emotional component that, in turn, can be distinguished into anger, defined through seven items (as an example: "I sometimes feel like a powder keg ready to explode") and a cognitive element, represented by the subscale of hostility, made of eight items (as an example: "I wonder why sometimes I feel so bitter about things").
Each item has to be assessed through a five-point Likert scale, whereas 1 stands for extremely bad conditions and 5 is equal to extremely positive. The total scores can be derived by the sum of the single items scores.
Other information has been collected through the Patient Health Questionnaire (PHQ), including 10 sub-scales that concern specifically depressive and somatic symptoms (Becker, Al Zaid & Al Faris, 2002; Settineri et al., 2013). In particular, mood disorders are evaluated through 18 items that include depression and dysthymia; somatoform disorders are assessed through 13 items related to somatization; anxiety disorders can be monitored through 12 items including panic attacks and other anxiety related syndromes; eating disorders can be derived by 8 items including bulimia and binge-disorders; and disorders linked to substance abuse are assessed through 3 items, including the frequent use of alcohol. The answers were given a score of 0 or 1 to indicate the absence or the presence of the disorder on the basis of diagnostic criteria.
In the presence study, the variable related to depressive symptoms has been employed.
3. RESULTS
Descriptive statistics can be seen in Table 1.
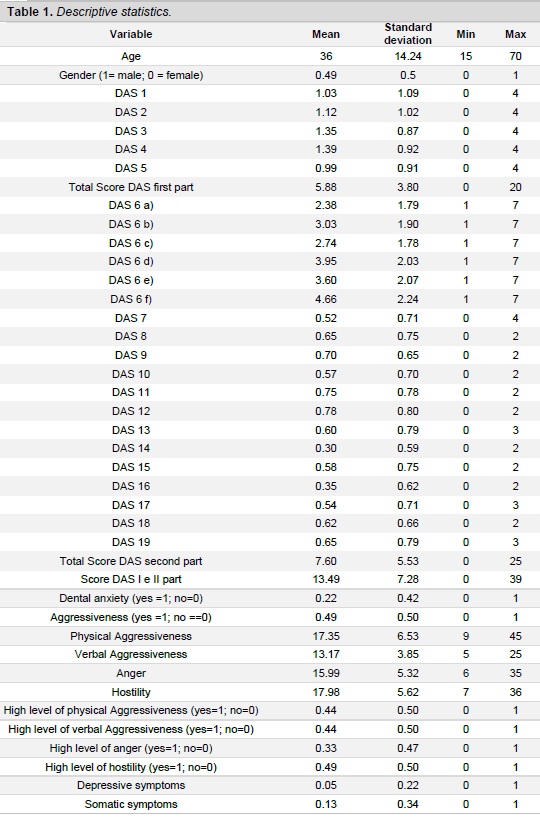
The final sample considered for the study included observations about 503 consecutive patients at dental settings. Patients were between 15 and 70 years old (mean age = 36, median = 34); 49% were male. Potential subjects were excluded from the study if they presented signs of neurological disease and were using psychoactive drugs.
The DAS and the AQ questionnaires have been administered while patients were in the waiting room of the dental settings after having obtained their consent and before the dental interventions. Prior consent was also obtained from the dentist.
A low dental anxiety level can be defined if the total DAS score is lower than 14; a high level occurs if the score is higher than 15, in line with Corah (1969) and Corah et al. (1978). Overall, 22.46% of interviewed people in dental settings presented a high level of dental anxiety.
Relating to AQ, instead, 49% of interviewed people manifested at least any dimension of aggressiveness: the dimension of "hostility" presented the highest average score (17.98 over 36).
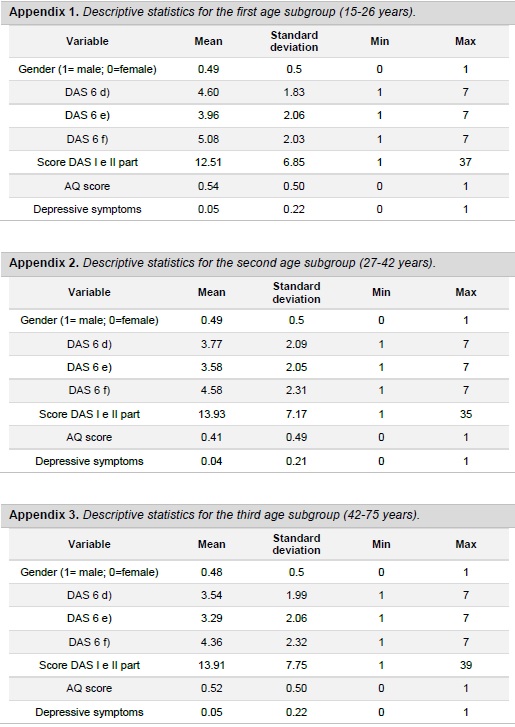
The sample was then split into three subsamples according to the age range: young people (between 15 and 26 years old), young adults (27-42 years old) and adults (43-70 years) (Table 2).

In Table 3, the variables related to dental anxiety and aggressiveness have been considered according to age and gender of interviewed people.
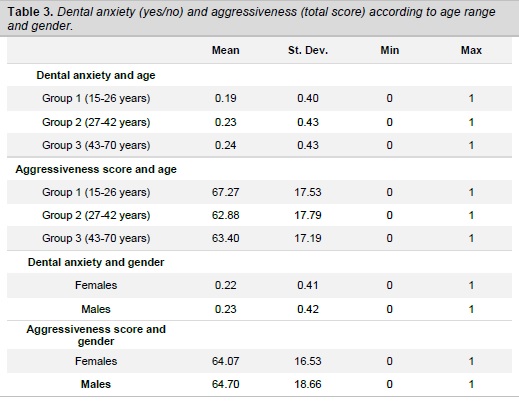
About 22% of women (23.07% of male patients) declare to be anxious with regards to the dental intervention. A lower level of dental anxiety characterizes young people (19.6% of people aged between 15 and 26 years old declares anxiety in medical settings) comparing to the oldest (24.37%).
Young people show a high level of aggressiveness according to the AQ (average score of 67.27 comparing to 62.88 reported by young adults).
Table 4 shows the pairwise correlations between the items proposed in the 6th question of DAS and the overall score recorded for aggressiveness.
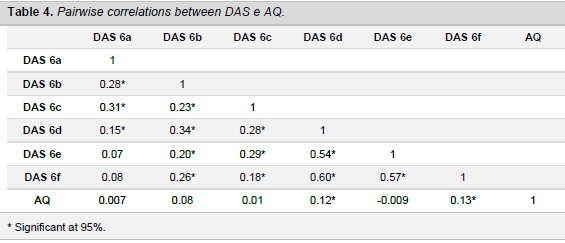
There is a positive and significant correlation of the AQ score with items d) and f) of DAS. Together with item e), these are the items more frequently reported by all the interviewed patients; moreover, the same items register the highest average scores and have therefore been considered among the explanatory variables in the estimations.
The nature of the dependent variable suggested us to employ, for the econometric analysis, a tobit model, which allows to deal with datasets in which some observations are not available over the entire range.
Let us consider the following equation:
- y*i = xi β + εi
where y*i is a “latent” variable, which is observed only if it takes a value that is lower than a constant α, x is the set of regressors and εi ∼ N (0, σ2) is the error term.
Here, the score for dental anxiety assumes the highest possible value of 51: as it has been said, in fact, it is obtained by adding the score reported in the first part of DAS, with the exclusion of question 6 (maximum score = 20), and the score reported in the second part (maximum score = 31). This is the censoring value for the dependent variable. Although, in theory, it could be possible to attribute whatever value to dental anxiety, the highest is set at 51: this “censoring” in the values, assumed by the dependent variable, justifies the choice for a tobit model.
While the dependent variable is the score reported for dental anxiety, the explanatory variables employed are related to age (and age squared, to see if this variable shows a linear relationship with the dependent variable), gender, presence of aggressiveness (the latter assumes value = 1 if the AQ score is higher than 61 and = 0 otherwise, over the maximum score recorded of 131), a control dummy related to the previous presence of depressive symptoms, and, finally, some DAS items related to the 6th question.
The first estimation was related to the whole sample. However, in order to take into account differences in aggressive behavior due to patients’ age, the estimations have been repeated for the three sub-samples.
Table 5 presents the estimation results.
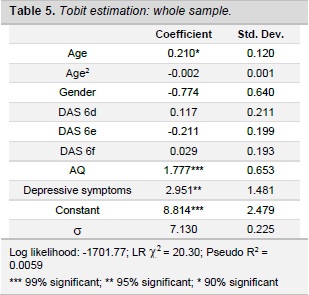
Age (and age-squared) shows a not linear correlation with the dependent variable. Gender is not significant as well as the DAS items most frequently reported. The overall score obtained from the AQ is positively and significantly correlated with the dependent variable: hence, there is a considerable impact of hostility on dental anxiety, although even a greater impact is exerted by the presence of depressive symptoms.
Repeating the estimations for each of the three age subgroups, it is possible to draw different conclusions about the significance of some DAS items.
In Table 6a, the results for the age group 15-26 years are shown. Age and age squared have not been considered among the regressors. AQ and depressive symptoms are not significant as they were in the overall regression. The coefficient related to the feeling of suffocation (DAS 6e) has, surprisingly, a negative correlation with dental anxiety: it would seem that the level of anxiety remains unaffected for young people.
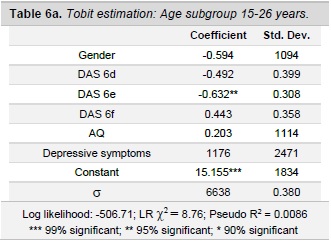
Hence, young people do not show a level of anxiety in dental settings likely to evolve in a specific psychiatric pathology.
Table 6b shows the results for the second subgroup (young adults aged between 27 and 42 years old). The coefficient of the DAS item related to the smell of teeth being drilled (DAS 6d) is positively and significantly correlated with the dependent variable.
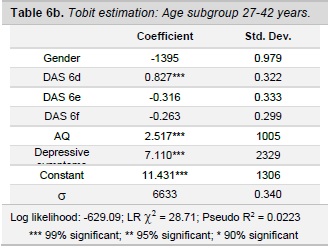
Dental anxiety is explained by the AQ score and by the presence of depressive symptoms, which present a positive and significant correlation with dental anxiety. It would seem that women may be more affected by dental anxiety, although this correlation is not significant, neither in the overall regression, nor in the estimations carried out for each of the three subgroups.
Table 6c presents the results for the third subgroup, related to people aged more than 42. In this estimation, the only relevant effect is exerted by the presence of aggressiveness. Depressive symptoms have not a significant effect on dental anxiety, although there is an inverse correlation between these two variables.
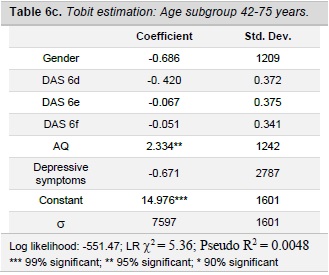
This result could be explained by considering that adult patients demonstrate a defensive behavior towards dentists, as a result of a cognitive evaluation.
4. DISCUSSION
This study has been aimed at testing to what extent dental anxiety can be explained by looking at patients’ characteristics solely or by considering also latent aggressiveness before and during the dental treatment.
Data retrieved by interviews done to 503 consecutive patients who went to dental settings have been employed.
Results of the estimations carried out show the relevance of aggressiveness in developing dental anxiety; a significant influence is exerted by the presence of depressive symptoms too. It would seem that there are no significant gender differences. There is a nonlinear relationship with age; the most significant findings emerge when the age group between 27 and 42 years is considered.
The regression carried out for the whole sample showed a nonlinear relationship between dental anxiety and patients’ age; while gender is not significant, it has been stressed the relevance of factors such as the presence of depressive symptoms and the AQ score in determining anxiety in dental settings.
The role of depression should not be neglected: dentists should pay more attention to those patients showing depressive symptoms. In other estimations, whose results are not reported here, it was seen that the introduction, among the covariates, of a dummy variable related to depressive symptoms for male patients, had a significant correlation with the presence of dental anxiety: men affected by depressive symptoms are, therefore, more likely to show dental anxiety (Kaspers, 2001; Settineri et al., 2013). Somatic disturbances, included in other estimations, whose results are no reported here, had no effect on dental anxiety.
5. CONCLUSIONS
This study has to be regarded as one of the first attempts to analyze the relationship between dental anxiety and aggressive behavior in dental settings. Such correlation has been demonstrated.
However, there are some limitations in the study. Some qualitative information related to dental settings are lacking, such as the type of setting, the medical staff and their competences, together with the population referring to each setting. Further studies could be based on the stratification of patients according, first of all, to age.
Nonetheless, the analysis leads to useful and interesting results. Moreover, the results confirm the relationship between dentistry and psychiatry (Jören, Jackowski, Gängler, Sartory & Thom, 2000 Settineri, Mucciardi, Leonardi, Mallamace & Mento, 2010). It would not seem that dental anxiety, as defined in this study, presents characteristics likely to let us to identify a specific psychiatric illness, as it was assumed here: rather, dental anxiety is seen as the manifestation of a general latent anxiety.
In order to estimate the probability for a specific psychiatric disorder to arise, it should be advisable to repeat the analysis on a wider population. In the case dental anxiety had to be considered as a specific anxiety, the dentist should make an accurate anamnesis and support patients, in order to enhance their compliance to any treatment.
6. REFERENCES
Abrahamsson, K.H., Berggren, U. & Carlsson, S.G. (2000). Psychosocial aspects of dental and general fears in dental phobic patients. Acta Odontologica Scandinavica, 58(1), 37-43. [ Links ]
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders (4th ed). Washington, DC: American Psychiatric Association. [ Links ]
Anttila, S., Knuuttila, M., Ylöstalo, P. & Joukamaa, M. (2006). Symptoms of depression and anxiety in relation to dental health behavior and self-perceived dental treatment need. European Journal of Oral Sciences, 114, 109-114. [ Links ]
Becker, S., Al Zaid, K. & Al Faris, E. (2002). Screening for somatization and depression in Saudi Arabia: A validation study of the PHQ in primary care. International Journal of Psychiatry in Medicine, 32, 271-283. [ Links ]
Buss, A. H. & Perry, M. P. (1992). The aggression questionnaire. Journal of Personality and Social Psychology, 63, 452-459. [ Links ]
Corah, N.L. (1969). Development of a dental anxiety scale. Journal of Dental Research, 48, 596. [ Links ]
Corah, N.L., Gale, E.N. & Illig, S.J. (1978). Assessment of a dental anxiety scale. The Journal of the American Dental Association, 87, 816-819. [ Links ]
Doebling, S. & Rowe, M.M. (2000). Negative perceptions of dental stimuli and their effects on dental fear. Journal of Dental Hygiene, 74 (2), 110-116. [ Links ]
Economou, G.C. & Honours, B. (2003). Dental anxiety and personality: Investigating the relationship between dental anxiety and self-consciousness. Journal of Dental Education, 267, 970-980. [ Links ]
Jören, P., Jackowski, J., Gängler, P., Sartory, G. & Thom, A. (2000). Fear reduction in patients with dental treatment phobia. British Journal of Oral and Maxillofacial Surgery, 38, 612-616. [ Links ]
Kaspers, S. (2001). Depression and anxiety-separate or continuum? World Journal Biological Psychiatry, 162, 162-163. [ Links ]
Locker, D. (2003). Psychological consequences of dental fear and anxiety. Community Dentistry and Oral Epidemiology, 31, 144-151. [ Links ]
Locker, D., Thomson, W.M. & Poulton, R. (2001a). Psychological disorder, conditioning experiences, and the onset of dental anxiety in early adulthood. Journal Dental Research, 80, 1588-1592. [ Links ]
Locker, D., Thomson, W.M. & Poulton, R. (2001b). Onset and patterns of change in dental anxiety in adolescence and early adulthood: a birth cohort study. Comm Denth Health 18 (2), 99-104. [ Links ]
Maggirias, J. & Locker, D. (2002). Five-year incidence of dental anxiety in an adult population. Community Dental Health, 19, 173-179. [ Links ]
Quteish Taani, D.S. (2002). Dental anxiety and regularity of dental attendance in younger adults. Journal Oral Rehabilitation, 29(6), 604-608. [ Links ]
Settineri, S., Mallamace, D., Muscatello, M.R., Zoccali, R. & Mento, C. (2013). Dental anxiety, psychiatry and dental treatment: How are they linked? Open Journal of Psychiatry, 3, 168-172. [ Links ]
Settineri, S., Mucciardi, M., Leonardi, V., Mallamace, D. & Mento, C. (2010). The emotion of disgust in Italian students: A measure of the Synthetic Disgust Index. International Journal of Psychological Research. 6, 1, 21-29. [ Links ]
Van Toller, S. (1988). Odours, emotion and psychophysiology. International Journal of Cosmetic Sciences, 10, 171-197. [ Links ]
APPENDIX