










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkInternational Journal of Psychological Research
Print version ISSN 2011-2084
int.j.psychol.res. vol.8 no.1 Medellín Jan./June. 2015
Affective Control and Life Satisfaction in Thalassemics
Control Afectivo y Satisfacción con la Vida en Talasémicos
Carmela Mentoa,* Basília PirainoB, Amelia Rizzoc, Roberta Ventod, Luciana Rigolib, Emanuela Moschellae, Carmelo Salpietrob, Salvatore Settineric
a Department of Neurosciences, University of Messina, Messina, Italy.
b Department od Pediatrics, Unit of Pediatric Genetics & Immunology, University of Messina, Italy.
c Department of Human and Social Sciences, University of Messina, Italy
d Psychological Doctor, University of Messina, Italy
e Department of Sociology and Social Research, University of Trento, Italy.
* Corresponding author: Carmela Mento, Department of Neurosciences, University of Messina, Messina, Italy. Email address: cmento@unime.it
Received: 08-01-2014 Revised: 26-09-2014 Accepted: 12-12-2014
ABSTRACT
Background. Thalassemia is a chronic disease that can lead to an impact on psychological functioning and social behavior of patients. However, still little is known about the specific psychological aspects of the disease, such as the degree of tension, life satisfaction and affective control, especially in adult patients.
Aim. The purpose of this study is to investigate whether patients with thalassemia have specific psychological pattern relating to the dimensions of tension, satisfaction and quality of life, management of affection.
Method. We evaluated 31 patients with thalassemia major and intermedia (19 women and 12 men) aged between 18 and 50 years (M = 34 + 16), belonging to the Complex Unit of Medical Genetics. For the evaluation were used the Profile of Mood States (POMS), the Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q) and the Rorschach test.
Results. The findings show an inverse relationship between the levels of self-reported tension and the affective control indicators at Rorschach. Life satisfaction, instead, seems to vary according to the severity of the disease - major vs. intermediate - and the type of therapy.
Conclusions. An understanding of the psychological mechanisms involved in thalassemia, both self-reported and projective, can contribute to a wider patient takeover, by considering the subjective aspects related to the psychological and socio-emotional well-being, fundamental in the care compliance.
Key words: thalassaemia, Affective Control, Quality of Life.
RESUMEN
Antecedentes: La Talasemia es una enfermedad crónica que puede conducir a un impacto en el funcionamiento psicológico y el comportamiento social de los pacientes. Sin embargo, todavía se sabe poco sobre los aspectos psicológicos específicos de esta enfermedad, tales como el grado de tensión, satisfacción con la vida y el control afectivo, sobre todo en pacientes adultos.
Objetivo: El propósito de este estudio, es investigar si los pacientes con Talasemia tienen un patrón psicológico específico relacionado con las dimensiones de tensión, la satisfacción, calidad de vida y el manejo del afecto.
Método: 31 pacientes con Talasemia mayor e intermedia fueron evaluados: (19 mujeres y 12 hombres) con edades entre 18 y 50 años (M= 34+16), pertenecientes a la Unidad de Complejo de Genética Médica. Para la evaluación fueron utilizados el Perfil de Estados de Ánimo (POMS), la calidad de vida: Satisfacción y placer (Q-LES-Q) y el test de Rorschach.
Resultados: Los resultados muestran una relación inversa entre los niveles de tensión de auto-reporte y los indicadores de control afectivo en el test de Rorschach. La satisfacción con la vida, por el contrario parece variar según la gravedad de la enfermedad: major vs. intermedio - y el tipo de terapia.
Conclusiones: la comprensión de los mecanismos psicológicos implicados en la talasemia, tanto en el auto-reporte como en lo proyectivo, puede contribuir a una toma de control más amplia del paciente, considerando los aspectos subjetivos relacionados con el bienestar psicológico y socio-emocional, fundamentales en el cumplimiento del cuidado.
Palabras clave: talasemia, control afectivo, calidad de vida.
1. INTRODUCTION
The p-thalassemia (BT) is a genetically determined chronic disease, that involves an hematologic imbalance: anemia, namely a decrease in the presence of hemoglobin, useful in the oxygen transport in blood (Weatherall & Clegg, 2008). As such, it may lead to an impact on the psychological functioning and social behavior of the patients (Aydin et al., 1997).
Messina et colleagues (2008), in their study about the young adults thalassaemics' psychological aspects, found that the self-image was characterized by poor feeling and vulnerability; the quality of life showed that the emotional role and social function were considerably low in all of the domains; the coping strategy used was escape-avoidance and, finally, that thalassemics showed a personality characterized by somatization, depression and obsessive-compulsive traits.
Zani, Di Palma & Vullo (1995), instead, have investigated the quality of social relationships, the degree of social integration, different aspects of self-concept and the coping strategies used by thalassaemics. The authors found similar scores compared to healthy peers, hypothesising that chronic illness does not necessarily imply psychopathologies, but can strengthen individuals' resources, contrary to the traditional stereotype.
The theoretical issues raised by the studies reported in literature are numerous. Several studies have focused on children and adolescents (Shaligram, D., Girimaji, S. C., & Chaturvedi, S. K. 2007; Tsiantis, J., Dragonas, T. H., Richardson, C., Anastasopoulos, D. , Masera, G., & Spinetta, J.1996.) or on young thalassemics (Messina, G., Colombo, E., Cassinerio, E. , Ferri, F., Curti, R., Altamura, C., & Cappellini, M. D.,2008; Palma, A., Vullo, C., Zani, B., & Facchini, A., 1998). Therefore there are few empirical data that describe the psychological experience of adult patients, up to 50 years. In addition, there are few studies that have included in the assessment some projective method (Guasco, G., La Mantia, A., & Cuniolo, A., 1986; Messina, G., Colombo, E., Cassinerio, E., Cesaretti, C., Marcon, A., Zanaboni, L., & Cappellini, M. D.,2010), plausibly due to the difficulty of applying psychological and complex analysis of personality in these patients.
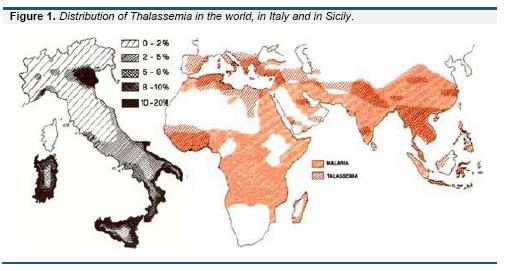
Even, the BT is prevalent in the Mediterranean countries, the Middle East, Central Asia, India, South China, North Africa and South America (Birgens & Lijung, 2007). The annual incidence of symptomatic cases of BT is 1/100.00 in the world, 1/10.000 in Europe. In Italy patients with thalassemia are about 7.000 and are mainly concentrated in areas of the Po Delta, Sardinia and Sicily (Figure 1). In our province, the thalassemia patients, taken into care by the University Hospital of Messina and the Microcythemia Center of S.Agata Militello are about 130 (Carbone, 2014).
To our knowledge, studies are also limited in our geographic region: Sicily, Meditterranean Island. Most of the studies carried out in our territory in fact have focused on the genetic aspects and not on the psychological ones (Powell, W. N., Rodarte, J. G., & Neel, J. V, 1950; Marzo, R. D., Dowling, C. E., Wong, C., Maggio, A., & Kazazian, H. H,1988; Maggio, A., Giambona, A., Cai, S. P., Wall, J., Kan, Y. W., & Chehab, F. F,1993).
Figure 1 - Distribution of Thalassemia in the world, in Italy and in Sicily.
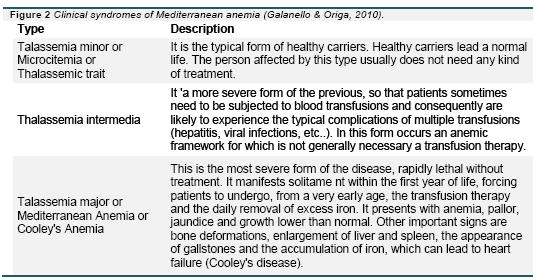
Finally, as we have seen, literature data are sometimes conflicting: some authors argue that there is a psycho-pathological impact, others that the disease may even reinforce individual resources. In conclusion, yet little is known about the specific psychological aspects of the disease, such as the degree of tension, life satisfaction and affective control, especially in adult patients, and also about the role of illness severity (major vs. intermedia) and therapy type (figure 2).
From these premises, the present study has the overall objective to explore any specific psychological pattern in patients with p-thalassemia. The specific objectives, instead, can be formulated as follows:
H 1: "A different level of tension correspond
to a different degree of the affective control"
H 2: "There is a difference based on the type of therapy about the overall satisfaction with
life"
H 3: "There is a difference between thalassemia major and intermedia on the three parameters considered"
Figure 2 - Clinical syndromes Mediterranean anemia (Galanello & Origa, 2010).
2. METHOD
2.1 Sample
The study was conducted on a sample of 31 subjects (19 females and 12 males) aged between 18 and 50 years (M = 34 + 16), all with a secondary school diploma and diagnosed with Thalassemia Major or Intermedia, treated at the University Hospital of Messina, Unit of Genetics and Pediatric Immunology. The sample is sufficiently representative. In the province of Messina there are about 130 persons, of which they are taken into care annually about 50: has therefore participated at the study the 62% of the elegibile population. The inclusion criteria for the study were: (1) Presence of Major or Intermedia Thalassemia requiring periodic transfusions; (2) Age not less than 18 years; (3) Taking charge of the patients during half 2014; (4) Absence of neurological or cognitive deficits ascertained.
2.2 Procedure
The study adhered to the ethical principles of research contained in the Declaration of Helsinki. The subjects agreed to participate in the study by signing an appropriate informed consent for the processing of data that emerged from the research. The administration of the tests took place in the moments before or after the transfusion therapy or follow-up visit. Each individual administration has provided a total duration between 30 and 50 minutes. After about a week each subject has read his/her results.
2.3 Instruments
The Profile of Mood States (POMS) is a self-assessment mood scale consisting of 58 items (McNair, D. M., Lorr, M., & Droppleman, L. F, 1971).
The subject must indicate on a Likert scale from 0 (not at all) to 4 (very much) as the last week has experienced the moods listed. The instrument consists of 6 subscales: (1) Tension - Anxiety; (2) Depression - Dejection; (3) Aggression - Anger; (4) Vigor - Activity; (5) Fatigue - Indolence; (6) Confusion - Bewilderment. The subject obtains a score for each subscale, which can be transformed into standard scores (points T).
The Q-LES-Q is a self-reported questionnaire, with 93 items (Endicott, J., Nee, J., Harrison, W., & Blumenthal, R, 1993). It evaluates overall enjoyment and satisfaction with physical health, mood, work, household and leisure activities, social and family relationships, daily functioning, sexual life, economic status, overall well-being and medications. Responses are scored on a 5-point scale ('not at all or never' to 'frequently or all the time'), where higher scores indicate better enjoyment and satisfaction with life. Fourteen summated items create the total Q-LES-Q score (possible range 14-70). Two last items, about medications and overall life satisfaction, are considered independently.
The Rorschach projective tecnique (Rorschach, 1927) is a psychological test, consisting of ten inkblot tables, that explores the subjective organization of the content and form of the ambiguous stimuli presented. Responses are recorded, analyzed and interpretated to examine personality characteristics and emotional functioning. Each Rorschach's table has a main theme, with an important interpretative value. Coding Rorschach responses requires taking all of the text transcribed during the test administration (qualitative material) and turning it into numeric scores (quantitative information) that will later be used in the structural summary, and ultimately, for interpretation (Bohm E., 1958; Passi Tognazzo D., 1994; Rose, T., Kaser-Boyd, N., & Maloney, M. P, 2001). In the present study the clinical method has been used: this approach is focused of the perception process of the patient and has to be considered as linked to the clinical symptomathology.
3. RESULTS
Data were analyzed using the statistical software SPSS 0.17. Because of the small sample size and the type of data non parametric tests are indicated. For the analysis were performed: the Spearman's rho correlation coefficient, the Mann & Withney test to compare groups and the Kruskall Wallis test to compare different conditions. The last has as result the chi-square represented in the table.
H 1: "A different level of tension correspond to a different degree of the affective control"
For the evaluation, we considered only the tension subscale Tension-Anxiety of the POMS. The subjects obtained an average of 53.10 + 11:23, from a minimum of 40 to a maximum of 86 T points. Considering on the average the scores included in the between 50 + 10, we found that: 80 .6% of subjects achieved scores in the average (between 40 and 60 points T), the 12.9% reported a moderate tension level (between 61 and 70 points T), the 6.5% reported scores that indicate clinically significative irritanility (higher than 81 points T). Scores in our sample are distributed in an almost normal curve (skewness = 1:33, kurtosis = 1.92).
Regarding the affective control, we have considered the Rorschach determinants that best reveal the capacity or inadequacy in the management of emotions, analyzed according to the directions of the Italian school (Passi Tognazzo, 1994): the answers F (Form), M (Human Movement), C (Pure Color), CF (Colour Form) and FC (Form Color). The total number of answers, for each patient and the whole sample, and the related percentages has been calculated. To verify the association of the variables considered Spearman's rho correlation coefficient was performed. The analysis revealed a significant negative association between the score of Tension-Anxiety and the answers FC [r = - .380; p <.05], but there were no other significant associations: the higher the tension level, the lower the affective control at the Rorschach and vice versa.
To better understand the relationship between the variables considered, we carried out a further qualitative analysis. Table 1 shows the percentage of Rorschach responses related to the control of affect, based on the levels of tension observed at the POMS (table 1).
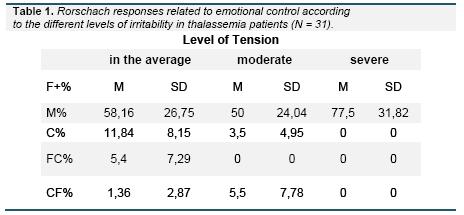
Table 1 - Rorschach responses related to emotional control according to the different levels of tension in thalassemia patients (N = 31).
As can be seen in Table 1, subjects showing an tension level in the average provided to the Rorschach an average number of responses F +, M, C and CF; subjects with a moderate level of tension show a lower average of F +, M and C, but a greater number of FC. Finally, subjects with clinically significant level of tension show an elevation of F + responses and a complete lack of M, C, CF and FC responses, resulting in a coarcted "erlebnistypus" (inner life experience).
H 2: "There is a difference based on the type of therapy about the overall satisfaction with life"
The Kruskal Wallis test (table 2) shows that the greatest satisfaction in the areas of quality of life considered are in favor of oral therapy (M = 47.85 + 4:39; 59%). The reduced quality of life and satisfaction is, instead, associated with the combined therapy (M = 33.00 + 2.94, 34%). The levels of satisfaction of patients receiving subcutaneous therapy (M = 44.58 + 6.83, 54%) obtained scores similar to patients not receiving any treatment (M = 42.50 + 3:54, 50%).
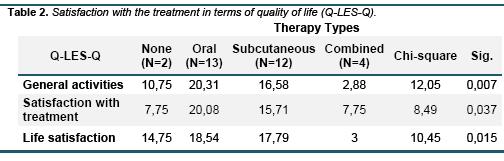
Table 2 - Satisfaction with the treatment in terms of quality of life (Q-LES-Q).
H 3: "There is a difference between thalassemia major and intermedia on the three parameters considered"
with regard to the level of the Tension-Anxiety of the POMS, no significant differences between the two groups emerged. Similarly, there are no statistical differences between the Rorschach responses. However, it should be noted (table 3) that subjects with thalassemia intermedia show an higher percentage of F + responses. For the level of satisfaction with life (QoL) the Mann & Withney test revealed that patients with thalassemia major, instead, report greater satisfaction with treatment [Major M = 70.0 + 16.6; Intermedia M = 54.2 + 22.2; U = 51.0 p <.05]. The majority of patients with thalassemia major essentially assume an oral administred therapy.
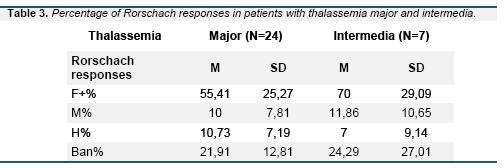
Table 3 - Percentage of Rorschach responses in patients with thalassemia major and intermedia.
As clinical psychologists we evaluated, at least, the most frequent contents of the whole sample that presents 365 complexive responses. Through a qualitative analysis, five prevalent images emerged: fire (7), monster (6), mask (5), elephants (4) and orchids (3). The response Fire is considered an emotional content without control (C pure). It refers to impulsiveness and affective lability (Sandler & Ackner, 1951). The Monster is instead a symbol of anguish and anxiety, that often emerges at the IV Rorschach table (Settineri S., Lo Presti E., Liotta M. & Mento C, 2013). It could refer to the Father Image and the Super-Egoic component experienced as a source of anxiety. The Mask is an archetypal figure emerged at the I and IX tables. It was been associated to the junghian concept of "Persona". It could represent the hiding of feelings and emotions in order to best adapt to the perceived social requests (Mento C., Galletti F., Galletti B., Longo P., Bitto E., Rizzo A., & Settineri S, 2014). The last two images are more rare (orig +).
Both have a connection to the oriental culture. The Elephant is sacre in India, it represents a royal symbol, is strong and powerful and is an archetype of the union between male and female (Goldfarb, 1945). The Orchid in Occident represents love, because of its capacity to grow everywhere; fertility and sexual beauty in Orient, where is utilized as a gift that symbolically represent sensuality and desire and perfection due to its symmetry (Jian-zhong, 2003). The emergence of the orchid at the VI table is therefore associated to the inner representation of sexuality, expecially as regards female subjects. Instead, the image of elephants emerge both in the III and the IX tables, in male subjects. The III table describe the images linked to self-image, interpersonal relationships and the representation of others (Passi Tognazzo, 1994). The response elephant at this table may evoke a sense of heaviness and discomfort in relationships.
4. DISCUSSION AND CONCLUSIONS
The present study had as its object the gain understanding of some aspects of the emotional experience of thalassemia patients, with particular reference to the levels of tension, the emotional control and the satisfaction with life and treatment.
The relationship between self-reported mood states and projective methods is quite complex. Bornstein et al. (1996) found that, in a non-clinical sample, the experimental induction of a mood state can modify projective responses, but not the answers given to the objective instruments, such as scales. These data demonstrate a deep connection between mood state and projection, which in our study is manifested as a significant inverse relation.
Previous research in the areas of social psychology, perception, memory, thinking, and creativity suggests that a happy mood promotes global, flexible, top-down processing, whereas a sad mood leads to a more analytic, less flexible, bottom-up processing (Dumitrascu, 2011). Effectively, in our study findings can be explained by this theoretical framework. Patients with thalassemia with normal levels of tension, on the other hand, show greater introspection, more affective lability and greater desire to adapt. Subjects with moderate levels of tension have less formal control, but a greater emotional control. Individuals with severe degree of tension prefer the interpretation of the form, without elements of affectivity and therefore tend to the emotional coarctation.
These key findings are useful to meet the overall aim of the research. Contrary to expectation, the specific pattern observed in thalassemia psychological attributable to the disease do not seem to be present. The statistical distribution of the scores of tension, in our sample, is similar to a normal distribution; projection by definition is associated with emotional states, as claimed by psychodynamic theories (Sandler, 2012), but still little studied from the empirical point of view.
We have reason to conclude that there is not a specific psychological pattern correlated to beta-thalassemia. It is plausible that each person may have a different impact on the disease on the base of personality traits and this could be the subject of future studies. At the moment, as pointed out by Telfer et al. (2006), in literature there are few studies on the evaluation of Quality of Life (QoL) in thalassemia. We think that this will be a valuable aid not only as an index of effective health care, ma anche come assessment that focuses on the individuals' own views of their well-being and assesses other aspects of life, giving a more holistic view of well-being.
To understand the impact of thalassemia on patients lives we explored their satisfaction in daily activities, towards treatment and life in general. Most of the subjects are placed in a normative range for the activities satisfaction, ranged between 50 and 59%. We noted, however, that individuals who swallow a combined therapy shows lower values of QoL (34%). Pakbaz et al. (2005) in a study on patients with thalassemia major and intermedia found that transfused patient had a poor quality of life and also feelings such as anxiety, depression, and concern of overall health status or indications of recent deterioration in health. Furthermore, the transfusion independent patients, in contrast with previous beliefs, suffered serious impairment in QoL too. This raises the question of the subjective condition of the thalassemic patient, depending on the severity of the disease and the possibilities of a minimally invasive medical treatment (Anie & Massaglia 2001; Daar & Pathare, 2006). However, we must not forget that the quality of life perception is a subjective state. Conflicting data on satisfaction with therapy may emphasize the need for attention to the individual experience of the subject, for whom the psychological evaluation during treatment may be an important resource for any programs of psychological support.
5. REFERENCES
Anie, K. A., & Massaglia, P. (2001). Psychological therapies for thalassaemia. Cochrane Database Syst Rev 3. [ Links ]
Aydin, B., Yaprak, I., Akarsu, D., Õkten, N., & Ülgen, M. (1997). Psychosocial aspects and psychiatric disorders in children with thalassemia major. Pediatrics International, 39(3), 354-357. [ Links ]
Birgens, H., & Ljung, R. (2007). The thalassaemia syndromes. Scandinavian journal of clinical & laboratory investigation, 67(1), 11 -26. [ Links ]
Bohm, E. (1958). A textbook in Rorschach diagnosis. New York: Grune & Stratton. [ Links ]
Bornstein, R. F., Bowers, K. S., & Bonner, S. (1996). Effects of induced mood states on objective and projective dependency scores. Journal of Personality Assessment, 67(2), 324-340. [ Links ]
Carbone, S. (2014). Thalassemia in Messina: a sociological approach to chronic disease. Thalassemia Reports, 4(1). [ Links ]
Daar, S., & Pathare, A. V. (2006). Combined therapy with desferrioxamine and deferiprone in beta thalassemia major patients with transfusional iron overload. Annals of hematology, 85(5), 315-319. [ Links ]
Dumitrascu, N. (2011). The Impact of Induced Mood on Visual Information Processing. The University Of Toledo. [ Links ]
Endicott, J., Nee, J., Harrison, W., & Blumenthal, R. (1993). Quality of life enjoyment and satisfaction questionnaire. Psychopharmacol Bull, 29(2), 321-326. [ Links ]
Galanello, R., & Origa, R. (2010). Review: Beta-thalassemia. Orphanet J Rare Dis, 5(11). [ Links ]
Goldfarb, W. (1945). The Animal Symbol in the Rorschach Test, and an Animal Association Test. Rorschach Research Exchange, 9(1), 822. [ Links ]
Guasco, G., La Mantia, A., & Cuniolo, A. (1986). [Psychological problems of thalassemic subjects]. La Pediatria medica e chirurgica: Medical and surgical pediatrics,9(3), 269-279. [ Links ]
Jian-zhong, Z. H. O. U. (2003). The Cultural Connotation of Orchid and its Orientation of Personality in Confucianism. Southeast Culture, 7, 009. [ Links ]
Maggio, A., Giambona, A., Cai, S. P., Wall, J., Kan, Y. W., & Chehab, F F. (1993). Rapid and simultaneous typing of hemoglobin S, hemoglobin C, and seven Mediterranean beta-thalassemia mutations by covalent reverse dot-blot analysis: application to prenatal diagnosis in Sicily. Blood, 81(1), 239-242. [ Links ]
Marzo, R. D., Dowling, C. E., Wong, C., Maggio, A., & Kazazian, H. H. (1988). The spectrum of p-thalassaemia mutations in Sicily. British journal of haematology, 69(3), 393-397. [ Links ]
McNair, D. M., Lorr, M., & Droppleman, L. F. (1971). POMS: profile of mood states. Educational and Industrial Testing Service: San Diego. [ Links ]
Mento C., Galletti F., Galletti B., Longo P., Bitto E., Rizzo A., & Settineri S. (2014). Representation, Projection and Cochlear Implant: a single case study. Mediterranean Journal of Clinical Psychology, vol. 2 n. 1. [ Links ]
Messina, G., Colombo, E., Cassinerio, E., Cesaretti, C., Marcon, A., Zanaboni, L., Baldini M., Cappellini, M. D. (2010). Pregnant women affected by thalassemia major: a controlled study of traits and personality. Journal of research in medical sciences 15 (2), 100-106. [ Links ]
Messina, G., Colombo, E., Cassinerio, E., Ferri, F., Curti, R., Altamura, C., & Cappellini, M. D. (2008). Psychosocial aspects and psychiatric disorders in young adult with thalassemia major. Internal and emergency medicine, 3(4), 339-343. [ Links ]
Pakbaz Z, Treadwell M, Yamashita R, Quirolo K, Foote D, ;Quill L, Singer T, Vichinsky EP (2005) Quality of Life in Patients with Thalassaemia Intermedia Compared to Thalassaemia Major. New York Academy of Sciences 1054 (1) 457-461. [ Links ]
Palma, A., Vullo, C., Zani, B., & Facchini, A. (1998). Psychosocial integration of adolescents and young adults with thalassemia major. Annals of the New York Academy of Sciences, 850(1), 355-360. [ Links ]
Passi Tognazzo, D. (1994). Il Metodo Rorschach, Manuale di psicodiagnostica su modelli di matrice europea. Firenze: Giunti Editore. [ Links ]
Powell, W. N., Rodarte, J. G., & Neel, J. V. (1950). The occurrence in a family of Sicilian ancestry of the traits for both sickling and thalassemia. Blood, 5(10), 887-897. [ Links ]
Rorschach, H. (1927). Rorschach Test -Psychodiagnostic Plates. Cambridge, MA: Hogrefe Publishing. [ Links ]
Rose, T., Kaser-Boyd, N., & Maloney, M. P. (2001). Essentials of Rorschach Assessment. Essentials of Psychological Assessment Series. John Wiley & Sons, Inc., 605 Third Avenue, New York, NY 10158. [ Links ]
Sandler, J. (Ed.). (2012). Projection, identification, projective identification. Karnac Books. [ Links ]
Sandler, J., & Ackner, B. (1951). Rorschach content analysis: an experimental investigation. British Journal of Medical Psychology,24(3), 180-201. [ Links ]
Settineri S., Lo Presti E., Liotta M. and Mento C. (2013). Trauma and the Father Image: Fantasies and Complexes in the Rorschach Test. The Open Psychology Journal vol. 6 p. 1 -5. [ Links ]
Shaligram, D., Girimaji, S. C., & Chaturvedi, S. K. (2007). Psychological problems and quality of life in children with thalassemia. The Indian Journal of Pediatrics, 74(8), 727-730. [ Links ]
Telfer, P., Constantinidou, G., Andreou, P., Christou, S., Modell, B., & Angastiniotis, M. (2005). Quality of life in thalassemia. Annals of the New York Academy of Sciences, 1054(1), 273-282. [ Links ]
Tsiantis, J., Dragonas, T. H., Richardson, C., Anastasopoulos, D., Masera, G., & Spinetta, J. (1996). Psychosocial problems and adjustment of children with p-thalassemia and their families. European child & adolescent psychiatry, 5(4), 193-203. [ Links ]
Weatherall, D. J., & Clegg, J. B. (2008). The thalassaemia syndromes. John Wiley & Sons. [ Links ]
Zani, B., Di Palma, A., & Vullo, C. (1995). Psychosocial aspects of chronic illness in adolescents with thalassaemia major. Journal of adolescence, 18(4), 387-402. [ Links ]
