










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkInternational Journal of Psychological Research
Print version ISSN 2011-2084
int.j.psychol.res. vol.9 no.1 Medellín Jan./June 2016
Balloon Analogue Risk Task to assess decision-making in Acquired Brain Injury
Globo Analógo de Tareas de riesgo para evaluar toma de desiciones en lesiones cerebrales adquiridas
Marina Areny Balagueroa,*, Mercè Jodar Vicentea,b, Alberto García Molinac,d, Josep María Tormos and Teresa Roig Rovirac,d
a Departmento de Psicología Clínica y de la Salud, Universitat Autónoma de Barcelona, Barcelona, España.
b Unitat de Neurologia, Hospital Universitari Taulí de Sabadell, Sadabell, España.
c Institut Guttmann, Universidad Autónoma de Barcelona, Badalona, Barcelona, España.
d Fundació Institut d'Investigació en Ciéncies de la Salut Germans Trias I Pujol, Badalona, Barcelona, España.
Corresponding author: Marina Areny Balaguero, Departamento de Psicología Clínica y de la Salud, Univeritat Autònoma de Barcelona Campus de Bellaterra, Edifici B, Bellaterra (Cerdanyola del Vallès), 08193 Tel: +34 687979252. Email address: mabalaguero@hotmail.es
Article history: Received: 18-06-2015 Revised: 24-09-2015 Accepted: 11-11-2015
ABSTRACT
Introduction: Although impairment in decision-making is a frequent consequence of frontal lobe injury, few instruments evaluate decision-making in patients with acquired brain injury (ABI). Most are difficult to use and require a well-preserved ability of complex verbal comprehension and executive functions. We propose the Balloon Analogue Risk Task (BART) as an alternative instrument to evaluate decision-making in ABI. Material and Methods: Balloon Analogue Risk Task (BART) and Iowa Gambling Task (IGT) were administered to a clinical group of 30 patients with ABI and to a control group of 30 healthy participants; comparative study to assess possible differences in the results obtained; analysis to determine a possible correlation between the two tests between groups.
Results: The results showed that BART is a sensitive instrument to detect differences in performance between a control group and a group of patients with ABI, p < .001, 95% CI =537.21-1575.46, but do not correlate with IGT, p = .524, rab.c = -.134. Conclusions: Although IGT and BART were both designed to assess decision-making, the results obtained in our study show that the scores obtained by patients with ABI on both tests do not correlate. This clearly proves that IGT and BART measure different aspects of decision-making.
Key words: acquired brain injury, Decision-making, Balloon Analogue Risk Task, Iowa Gambling Task.
RESUMEN
Introducción: a pesar de que el deterioro en la toma de decisiones es una consecuencia frecuente en las lesiones del lóbulo frontal, pocos son los instrumentos que evalúan la toma de decisiones en pacientes con lesiones cerebrales adquiridas (ABI). La mayoría son difíciles de utilizar y requieren una capacidad bien conservada de las funciones de comprensión y ejecutivas verbales complejas. Proponemos el globo analógico de tareas de riesgo (BART) como un instrumento alternativo para evaluar la toma de decisiones en las ABI.
Material y métodos: globo analógica de tareas de riesgo (BART) y juego de azar de Lowa (IGT) se administraron a un grupo clínico de 30 pacientes con ABI y a un grupo control de 30 participantes sanos; se realizó un estudio comparativo para evaluar las posibles diferencias en los resultados obtenidos y un análisis para determinar una posible correlación de las pruebas entre los grupos.
Resultados: Los resultados mostraron que el BART es un instrumento sensible para detectar diferencias en el rendimiento entre un grupo control y un grupo de pacientes con ABI, p <0,001; IC del 95% = 537,21 a 1.575,46, pero no se correlacionan con IGT, p = 0.524, rab.c = -.134.
Conclusiones: a pesar de que IGT y BART fueron diseñados para evaluar la toma de decisiones, los resultados obtenidos en nuestro estudio muestran que las puntuaciones obtenidas por los pacientes con ABI en ambas pruebas no se correlacionan. Esto demuestra claramente que la pruebas IGT y BART miden diferentes aspectos de la toma de decisiones.
Palabras clave: lesion cerebral adquirida, toma de decisiones, balón análogo de tareas de riesgo.
1. INTRODUCTION
The term "acquired brain injury" (ABI) refers to any damage to the brain that occurs after birth. According to the figures published on disability in the Observatorio estatal de discapacidad Bulletin (2011), 420,064 people in Spain suffer from acquired brain injury. The large majority of these cases (78%) have been caused by stroke accidents, while 22% correspond to traumatic brain injuries, brain tumours, infectious pathologies, post-surgical patients, and neurodegenerative diseases.
Due to its high incidence and prevalence, ABI is a matter of public health. It has long-term effects on patients and their relatives and entails high economic costs. The consequences of ABI can vary widely depending on the aetiology, the extension and the location of the ABI: vegetative states, minimally conscious states, and a variety of physical and/or cognitive alterations. This wide range of deficiencies, disabilities and handicaps are difficult to classify (Alberdi, Iriarte, Gorostidi, Murgialdai & Marco, 2009).The neuropsychological sequelae of ABI can be numerous and varied, depending on multiple factors (type of injury, location, extension, countercoup lesion, or patient's characteristics), although the most frequent affect attention, memory and executive functions. These cognitive deficits affect functionality and capacity in problem-solving and cause disability (Livingstone & Skelton, 2007) due to alterations in executive functions. The term executive functions refers to a group of cognitive abilities that aim to facilitate our adaptation to new or complex situations, that override routine and automatic behaviours (Collette, Hogge, Salmon & Van Der Linden, 2006). This group includes different abilities such as the ability to set goals, the development of plans of action, cognitive flexibility, inhibition of automatic responses, self-control of behaviour and verbal fluency (Fisk & Sharp, 2004). Executive functions are particularly vulnerable to several mental disorders and neurological diseases (Biringer et al., 2005; Davidson, Gao, Mason, Winocur & Anderson, 2007), constituting an additional challenge for the acquisition of autonomy and functionality as well as for decision-making (García et al., 2008).
The decision-making process requires the involvement of executive functions, since they are responsible for initiating, supervising, controlling and evaluating human behaviour. Choosing from several options can be a very simple task, but triggers numerous cognitive processes such as processing the stimulus present in the task, the memory of previous experiences and the evaluation of possible immediate and future consequences of the different options.
The ventromedial prefrontal cortex is involved in decision-making (Martínez, Sánchez, Bechara & Román, 2006), and is related to the reinforcements and punishments associated to behaviour, in order to optimise future responses when faced with ambiguous situations. All these processes require the involvement of working memory and, in general, the activation of higher brain functions. Additionally, the dorsolateral prefrontal cortex permits a better coordination of risks taken in decision-making (Fecteau, Pascual-Leone, Zald, Liguori, Théoret, Boggio, & Fregni, 2007).
The somatic marker hypothesis is being increasingly used to understand the functioning of decision-making. This hypothesis, formulated by Damasio (1996), describes the role of emotions in decision-making and has served as a guide for the research in this field. The somatic marker hypothesis would be a signal in shape of a somesthetic feeling that contributes to optimising our decisions and our reasoning. According to Damasio, our previous experiences lead us to store a series of event-related pleasant or unpleasant feelings that influence decisionmaking. Although the alteration of the decision-making ability is one of the most frequent consequences following a frontal lobe injury, there are few known instruments to evaluate decision-making in patients with ABI (Strauss, Sherman & Spreen, 2006).
The most widely used and validated instrument for the evaluation of this ability is the IGT (Iowa Gambling Test), introduced by Bechara, Damasio, Damasio and Anderson, researchers from the University of Iowa. The IGT is a task designed to simulate real-life decision-making processes, in which the patient must face an activity of punishment and reward. The subject must be capable of understanding the logic of the game and of differentiating between favourable and unfavourable options of the activity, which contribute to or hinder the final objective of the test. Presently, IGT is sometimes difficult to use because of the complexity of its execution. This instrument requires the participants to have a well-preserved ability of complex verbal comprehension, as well as a good functioning of most executive functions.
More recently, Lejuez et al. (2002) designed the Balloon Analogue Risk Task test (BART), a simpler computerised task used in the field of addictions, psychopathology, risk behaviours and to evaluate decision-making. The main objective of this test consists of facing the patient with a risk situation, in which a simple decision must be taken in order to obtain as much money as possible. It is an easier test than the IGT, not only as far as its execution is concerned, but also for its comprehension, which is an enormous advantage for its application on patients with brain injuries.
For this reason, we hypothesised that the BART is an alternative instrument for the evaluation of decision-making in adult ABI. The aim of this study was to test whether the results obtained with BART to assess decision-making in ABI correlated with those obtained with IGT.
2. MATERIAL AND METHODS
2.1 Design
A non-experimental, transversal, correlational study to establish associations and relations between the variables studied.
2.2 Participants
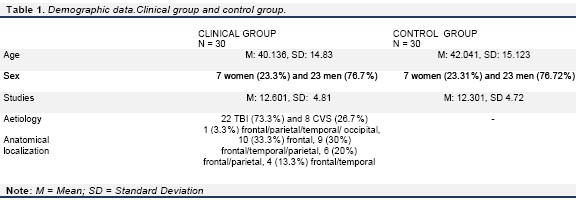
The clinical group consisted of 30 patients with ABI (7 women and 23 men), aged between 18 and 65 (M age = 40.136, SD = 14.83), with different types of brain lesions that were not only located in the frontal lobe, but also in other areas, due to the primary effects of the injury and secondary injuries (22 TBI and 8 Cerebrovascular Accidents (CVA). The education level of the participants varied (11 with primary education studies, 9 with secondary studies and 10 with higher education studies) (M studies = 12.601, SD = 4.811). The inclusion criteria for the clinical group were: patients with TBI or CVA with the presence of a frontal lobe lesion; age at the time of the injury between 18 and 65 years; no sensory and/or motor deficits that may impede the performance of any of the neuropsychological tests used in the study; and absence of difficulties in the understanding and expression of the language needed to follow instructions or coding the test items. The exclusion criteria were: acute confusional syndrome or post-traumatic amnesia; serious psychiatric disorder; behavioural changes that may make it difficult to administer the test.
The control group was made up of 30 healthy individuals with similar age and sociodemographic characteristics to the clinical group. The matched pairs method was used to select the voluntary control group (See Table 1).
2.3 Material
The Iowa Gambling Task (IGT) (Bechara, Damasio, Damasio & Anderson, 1994). The IGT is a computerised task which simulates the essential components of real-life decision-making situations. These components include the evaluation of reward and punishment in situations of uncertainty and risk. The task is based on a card game format to test decision-making. Participants are presented with 4 decks of cards (A, B, C, D) on a computer screen, each deck contains 60 cards. Participants must choose cards from these decks across 100 trials. The number of cards in each deck and the number of rehearsals is unknown to the participants. They are told that each time they choose a card, they will win some game money. The objective of the task is to try to win as much money as possible and try not to lose any. Each card is associated with an immediate economic reward. However, a lot of these cards also generate punishments in the form of money loss. Participants are unaware of the fact that two of the decks (A and B) are unfavourable because, despite generating larger immediate rewards, they also produce more severe losses and negative long-term results. The other 2 packs (C and D) are advantageous in the sense that they generate smaller rewards, but also give less severe punishments, generating long-term benefits. Therefore, in order to accumulate money in the task, the appropriate strategy is to consistently select more cards from packs C and D than from packs A and B.
The Balloon Analogue Risk Task (Lejuez et al., 2002). BART is a computerised task which simulates characteristics present in decision-making. The elements present in the task include the evaluation of gains and losses in situations of risk and uncertainty. The task consists of inflating some balloons which are presented visually. Participants must pump air into the balloons 30 times. Every time the balloon increases in size, the participant earns a fixed amount of money, but if the balloon bursts, the accumulated money is automatically lost. The probability that a balloon might explode is unknown to participants. The probability of explosion of each balloon every time it is inflated is 1/128. According to this algorithm, the average explosion point was 64 pumps for each balloon.
2.4 Procedure
Participants were either inpatients or outpatients. They were subjected to an extensive neurological and neuropsychological assessment, in which language and cognitive skills were evaluated, along with behavioural, motor and sensory aspects. All the evaluations were made from 6 months after the date of the brain injury (M = 222 days, SD = 32.05).Only those participants who fulfilled the inclusion and exclusion criteria were selected to form part of the clinical group. BART and IGT were administered exclusively to the clinical group to evaluate decision-making ability. These two tests were then administered to the control group, looking for paired participants. All the assessments were carried out by the same neuropsychologist. The time taken to collect the sample was one year.
2.5 Ethical considerations
Any information collected on participants was kept strictly confidential and anonymous. Written informed consent was obtained from all participants. As participation in the study was completely voluntary, eligible candidates were not obliged to participate and were free to withdraw from the study at any time.
2.6 Data analysis
The t-Student test for comparing the means of two independent samples was used to study the differences between groups (parametric tests). No statistical correction was used as a normality test performed prior to using the student t-test showed that our sample had a normal distribution. Partial correlations adjusted for the corresponding socio-demographic variables were used to observe the correlation of both samples in order to control for extraneous variables. Adjustments were made by sex, age, etiology, education and time elapsed after the session. In the control group, adjustments were made only by sex, age and education.
2.7 Description of variables
The variables used in BART were the following: Duration: Time that the participant takes to complete the test.
Pumps: T: Total number of pumps that the participant makes during the entire test in order to inflate the balloon.
Explosions T: Total number of exploded balloons in the entire test.
BART$: Total sum of money obtained. The studied variables in the IGT were the following: Net T: Packs of cards [(C + D) - (A + B)]. IGT$: Total sum of money obtained.
AB: Sum of cards lifted from Packs A + B.
3. RESULTS
3.1 Descriptive and comparative results between the clinical group and the control group in the BART
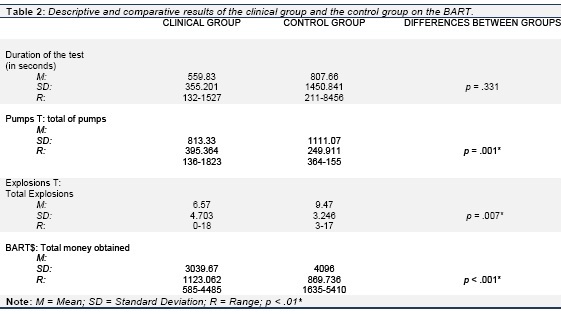
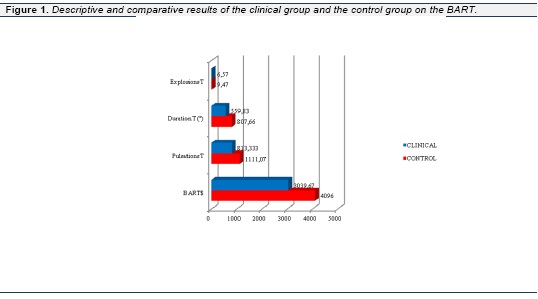
The BART was used to observe differences in the results obtained by the two groups studied. ABI patients performed the test in less time and made less Pumps T, Explosions T and BART$.
There were no significant differences between groups in the execution time of the task, p =.331, 95% CI = [-303.35, 804.43]. Differences were found in the total number of Pumps (Pumps T) between groups, p = .001, 95% CI = [126.12, 469.34], as healthy participants made a greater number of total pumps. There were also significant differences between the number of explosions (explosions T) between groups, p = .008, 95% CI = 0.812-4.988, with a greater number of total explosions in the control group. Finally, a difference in BART$ between groups was observed, p < .001, 95% CI = [537.209-1575.458]. Healthy participants accumulated more money at the end of the test than ABI patients (See Table 2 and Figure 1).
3.2 Descriptive and comparative results between the clinical group and the control group in the IGT
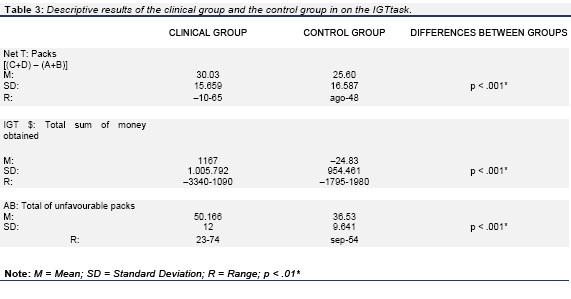
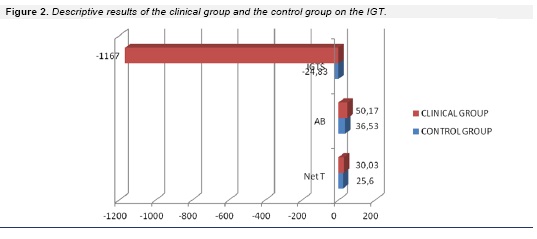
The control group, composed of healthy individuals, obtained normal scores according to normative data (Bechara, 2007), which, in general, was higher in Net T, IGT$ and AB.
A significant difference was observed between the Net T of the healthy group and the ABI group, p = .002, 95% CI= [-21.771 - -5.096], where the control group chose a larger amount of favourable cards. Similarly, a significant difference in IGT$ between groups was observed, p < 001, 95% CI =[ 637.6821646.652]. The control group accumulated more money at the end of the test than the clinical group. Finally, significant differences between groups were also observed in AB, p < .001, 95% CI = [-19.27, -7.10]. The clinical group tended to more unfavourable cards than the control group (See Table 3 and Figure 2).
3.3 Correlation between the administration of the BART and the IGT
No correlation was found between Net T and Pumps T in the clinical group, p = .315, rab.c= -.210. Similarly, there was no correlation between Pumps T and AB, p = .059, rab.c= .382, and finally, a correlation was observed between Total$ BART and Total$ IGT, p = .524, rab.c = -.134.
In the control group, no correlation was found between Net T and Pumps T, p = .725, r2 = ?.072 and there was no correlation between Pumps T and AB, p = .953, r2 = .012, or between Total$ BART and Total$ IGT, p = .814, r2 = ?.049.
4. DISCUSSION
The present study was carried out to determine whether the BART is a suitable instrument to assess decision-making in acquired brain injury. Our aim was to assess whether BART is able to detect differences between a group of ABI patients and a group of healthy subjects, and establish whether the BART correlates with IGT, which is the most widely used instrument to assess decision-making in patients with acquired brain injury.
Our results show differences in the scores obtained by the two groups, both on BART (ABI patients obtained less BART$), and in the number of pumps T and balloons exploded T in IGT, with a lower performance in the group of ABI patients.
Our findings are in line with a similar study performed by Young, Gudjonsson, Carter, Terry and Morris (2012) who used BART and also found that a clinical group (delinquents) made less pumps T than a control group.
Another study by Strenziok et al., (2011) indicated that participants with frontotemporal dementia with behavioural alterations made less pumps T at BART than a control group.
The research performed by Acheson, Richards and Wit, (2007) shows the existence of differences between a clinical group (women with sleep deprivation) and a healthy control group, as the latter made more pumps T and obtained more BART$. Comparable findings are reported in a study carried out by Lejuez et al. (2003) between a clinical group (smokers) and a control group.
Similarly to the results obtained in our study, Lighthall, Mather and Gorlick (2009) found differences in the BART between a control group and a clinical group (women with stress-related disorders), where the latter made less pumps and obtained less BART$.
In concordance with our results, healthy participants tend to select more cards from the advantageous decks (small wins and smaller losses) on IGT. Conversely, drug-dependent patients with orbitofrontal brain injury select more cards from disadvantageous decks (large wins and larger losses), due to the difficulties to process emotional signals associated with the affective value of the different options. Such patients are thus unable to anticipate the consequences of their choices (Alameda, Paíno & Mogedas, 2012; Mogedas & Alameda, 2011).
In a study performed by Broche, Cortés & Omar-Martínez (2015), youths with antisocial behavior have a worse performance on decision-making tasks on the IGT compared to a group of youths with adequate social behavior, which is in line with our findings.
The investigation carried out by Cardoso et al. (2014) concludes that participants with frontal lobe injury perform worse on IGT, as they select more disadvantageous decks than a healthy control group.
Several authors confirm that patients with TBI demonstrate poorer performance on IGT than a control group of healthy participants (Van Noordt & Good, 2011; Bonatti et al., 2008; Sigurdardottir Jerstad, Andelic, Roe & Schanke, 2010).
Miura et al. confirmed the poor decision-making capacity of adolescent males with antisocial behaviour with IGT in a study of 317 participants (Miura, 2009).
All these studies are in agreement with our findings, as in our sample, the group of healthy participants made more pumps and obtained more money on the BART and had a better performance on the IGT than the group of ABI patients.
Lastly, in our study, no correlation was observed between the capacity evaluated by IGT and BART. Although both tests were designed to assess decision-making, the results obtained in the present study indicate that they assess different aspects of decision-making competence. IGT requires preserved capacities on more complex cognitive abilities such as mnesic and attentional functions, executive functions and language, in order to understand the logic involved in the processes of reward and punishment of the task (Bechara, et al., 1994). Unlike IGT, BART, does not follow a predetermined logic, as the explosions occur randomly (Lejuez, et al., 2002). We are therefore faced with two tasks which evaluate different cognitive aspects.
BART seems to provide more direct information than IGT about the risk taken by the participants in decision-making. As Lejuez et al. (2002) concluded in their study, the BART was created to face the patient with a real risk situation.
Several studies have shown significant correlation between BART and self-report batteries related to sensation-seeking behaviour (Lejuez, Aklin, Zvolensky & Pedulla 2003; Killgore, 2007; Lejuez et al., 2007; MacPherson et al., 2010; Benjamin & Robbins, 2007). But in agreement with our results, no correlation was found between performance on BART and IGT (Lejuez et al., 2003; Buelow & Blaine, 2015).
In conclusion, BART is a sensitive instrument to detect differences between the control group and the clinical group, but the scores obtained with BART do not correlate with those of IGT.
It should be noted that the size of our sample is limited and that most of the participants are young with a medium level of education. It would therefore be interesting for future research to study the influence of schooling on BART performance on populations with different schooling levels and ages, as other studies have reported that age and level of education affect cognitive processes.
Another interesting variable to be considered is the influence of gender on cognitive alterations. This aspect was not assessed in this study due to the higher prevalence of males in our sample.
5. CLONCLUSIONS
In conclusion, our results show that the BART is a sensitive tool to detect differences in the decision-making capacity between a control group of healthy individuals and a group of patients with acquired brain injury. Nevertheless, it does not involve the same cognitive abilities that are required to execute the IGTt. While the BART is more directly related to risk, the IGT involves more complex cognitive functions.
In future investigations, it would be interesting to determine whether working memory and cognitive flexibility (abilities present in decision-making) can account for the changes in the BART performance of patients with acquired brain injury. If performance on BART depends on the working memory and cognitive flexibility of these patients, it is hoped that these cognitive functions would be good predictors of decision-making.
6. REFERENCES
Acheson, A., Richards, J.B. & Wit, H. (2007). Effects of sleep deprivation on impulsive behaviors in men and women. Physiol Behav, 91(5), 579-587. [ Links ]
Alameda, J.R., Paíno, S. y Mogedas, A.I. (2012). Toma de decisiones en consumidores de cannabis. Adicciones, 24(2), 161-172. [ Links ]
Alberdi, F., Iriarte, M., Mendia, A., Murgialda, A. & Marco, P. (2009). Prognosis of the sequels after brain injury. Medicina Intensiva, 33, 17181. doi:10.1016/S0210-5691(09)71213-6. [ Links ]
Benjamin, A. M., & Robbins, S. J. (2007). The role of framing effects in performance on the Balloon Analogue Risk Task (BART). Personality and Individual Differences, 43, 221- 230. doi:10.1016/j.paid.2006.11.026. [ Links ]
Bonatti, E., Zamarian, L., Wagner , M., Benke, T., Hollosi, P. & Strubreither, W. (2008). Making decisions and advising decisions in traumatic brain injury. Cogn Behav Neurol., 21, 164-175. doi doi: 10.1097/WNN.0b013e318184e688. [ Links ]
Buelow, M.T. & Blaine, A.L. (2015). The assessment of risky decision making: A factor analysis of performance on the Iowa gambling task, balloon analogue risk task, and Columbia card task. Psychol Asess, 27(3), 777-85. doi: 10.1037/a0038622. [ Links ]
Bechara, A., Damasio, A. R., Damasio, H. & Anderson, S. W. (1994). Insensitivity to future consequences following damage to human prefrontal cortex. Cognition, 50, 7-15. doi:10.10163/0010-0277(64)90018-3. [ Links ]
Bechara, A. (2007). Iowa Gambling Task: Professional Manual. Psychological Assessment Resourses, Inc. [ Links ]
Biringer, E., Lundervold, A., Stordal, K., Mykletun, A., Egeland, J., Bottlender, R., & Lund, A. (2005). Executive function improvement upon remission of recurrent unipolar depression. European Archives of Psychiatry and Clinical Neuroscience, 255, 373-380. doi:10.1007/s00406-0052-0577-7. [ Links ]
Broche-Pérez Y., Cortés-González, L. & Omar-Martínez, E. (2015). Toma de decisiones en jóvenes con conductas antisociales: Evidencias desde el Iowa Gambling Task. Neurología Argentina doi:10.1016/j.neuarg.2015.03.006. [ Links ]
Cardoso, C.O., Branco, L.D., Cotrena, C., Kristensen, C.H., SchneiderBakos, D.D.G. & Fonseca, R.P. (2014). The impact of frontal and cerebellar lesions on decision making: evidence from the Iowa Gambling Task. Front Neurosci, 8 doi: 10.1590/S0047-20852010000400003. [ Links ]
Collette, F., Hogge, M., Salmon, E., & Van der Linden, M. (2006). Exploration of the neural substrates of executive functioning by functional neuroimaging. Neuroscience, 139, 209- 221. doi:10.1016/j.neuroscience.2005.05.035. [ Links ]
Damasio, A. (1996). The somatic marker hypothesis and the possible functions of the prefrontal cortex. Philosophical Transactions of the Royal Society of London B, 351, 1413-1420. doi:10.1098/rstb.1996.0125. [ Links ]
Davidson, P. S., Gao, F .Q., Mason, W. P., Winocur, G., & Anderson, N. D. (2007). Verbal fluency, Trail Making and Wisconsin Card Sorting Test performance following right frontal lobe tumor resection. Journal of Clinical and Experimental Neuropsychology, 11, 1-15. doi:10.1080/13803390601161166. [ Links ]
Disability National Observatory (2011, January 20). New Data on the Incidence of DCA. Retrieved from: http://www.fedace.org/portal/index.php/noticias-de-actualidad/136-datosdca.html. [ Links ]
Fecteau, S., Pascual-Leone, A., Zald, D. H., Liguori, P., Théoret, H., Boggio, P. S., & Fregni, F. (2007). Activation of prefrontal cortex by transcranial direct current stimulation reduces appetite for risk during ambiguous decision making. The Journal of Neuroscience, 27(23), 6212-8. doi:10.1523/JNEUROSCI.0314-07.2007. [ Links ]
Fisk, J. E., & Sharp, C. A. (2004) Age related impairment in executive functioning: Updating, inhibition, shifting and access. Journal of Clinical and Experimental Neuropsychology, 26, 874-890. doi:10.1080/13803390490510680. [ Links ]
García Molina, A., Roig Rovira, T., Yuguero Rueda, M., Sánchez-Carrión, R (2008). Community integration as an outcome of traumatic brain injury neurorehabilitation. Rehabilitación, 42, 67-72. doi:10.1016/S0048-7120(08)73616-8. [ Links ]
Killgore, W. D. S. (2007). Effects of sleep deprivation and morningness-eveningness traits on risk-taking. Psychological Reports, 100, 613-626. doi:10.2466/PR0.100.2.613-626. [ Links ]
Lejuez, C. W., Read, J. P., Kahler, C. W., Richards, J. B., Ramsey, S. E., Stuart, G. L., Strong, D. R., & Brown, R. A. (2002). Evaluation of a behavioral measure of risk taking: the Balloon Analogue Risk Task (BART). Journal of Experimental Psychology: Applied, 8, 75-84. doi:10.1037//1076-898X.8.2.75. [ Links ]
Lejuez, W. C., Akalin, M. W., Zvolensky, J. M., & Pedulla, M. C. (2003). Evaluation of the Balloon Analogue Risk Task (BART) as a predictor of adolescent real-world risk-taking behaviors. Journal of Adolescence, 26, 475-479. doi:10.1016/S0140-1971(03)00036-8. [ Links ]
Lejuez, C. W., Aklin, W. M., Jones, H. A., Richards, J.B., Strong, D. R., Kahler, C. W. et al. (2003). The balloon analogue risk task (BART) differentiates smokers and nonsmokers. Experimental and Clinical Psychopharmacology, 11(1), 26-33. doi:10.1037/1064-1297.11.1.26. [ Links ]
Lejuez, C. W., Aklin, W. M., Daughters, S. B., Zvolensky, M. J., Kahler, C. W., & Gwadz, M. (2007). Reliability and validity of the youth version of the Balloon Analogue Risk Task (BART-Y) in the assessment of risk-taking behavior among inner-city adolescents. Journal of Clinical Child and Adolescent Psychology, 36, 106-111. doi: 10.1080/15374410709336573. [ Links ]
Lighthall NR, Sakaki M, Vasunilashorn S, Somayajula S, Chen E, Mather M. (2009). Sex differences in stress effects on brain activation and behavior during risk taking. Cognitive Neuroscience Society Annual Meeting. San Francisco, CA. [ Links ]
Livingstone, S. A., & Skelton, R. W. (2007). Virtual environment navigation tasks and the assessment of cognitive deficits in individuals with brain injury. Behavioural Brain Research, 185, 21-31. doi:10.1016/j.bbr.2007.07.015. [ Links ]
Madrazo, L. M., Machuca, M. F., Barrosso, J. M., Domínguez, M. D. & León-Carrión, J. (1999). Emotional changes after severe traumatic brain injury. Revista Española de Neurología, 1, 75-82. [ Links ]
Martínez-Selva, J. M., Sánchez-Navarro, J. P., Bechara, A., & Román, F. (2006). Brain mechanisms involved in decision making. Revista de Neurología, 42, 411-418. [ Links ]
MacPherson, L., Magidson, J. F., Reynolds, E. K., Kahler, C. W., & Lejuez, C. W. (2010). Changes in sensation seeking and risktaking propensity predict increases in alcohol use among early adolescents. Alcoholism, Clinical and Experimental Research, 34, 1400-08. doi: 10.1007/s11121 -010-0172-7. [ Links ]
Miura, H. (2009). Differences in frontal lobe function between violent and nonviolent conduct disorder in male adolescents. Psychiatry and Clinical Neurosciences, 63, 161-166. [ Links ]
Mogedas, A.I. & Alameda, J.R. (2011). Toma de decisiones en pacientes drogodependientes. Adicciones, 23, 277-287. [ Links ]
Rochat, L., Beni, C., Billieux, J., Azouvi, P., Annoni, J. M. & Van der Linden, M. (2010). Assessment of impulsivity after moderate to severe traumatic brain injury. Neuropsychological Rehabilitation, 20(5), 778-797. doi:10.1080/09602011.2010.495245. [ Links ]
Sigurdardottir, S., Andelic, N., Roe, C. & Schanke, A. K. (2009). Cognitive recovery and predictors of functional outcome 1 year after traumatic brain injury. Journal of the International Neuropsychological Society, 15, 740-750. doi:10.1017/S1355617709990452. [ Links ]
Sigurdardottir, S., Andelic, N., Roe, C. & Schanke, A. K. (2010). Cognitive recovery and predictors of functional outcome 1 year after traumatic brain injury. Journal of the International Neuropsychological Society, 15, 740-750. doi:10.1017/S1355617709990452. [ Links ]
Strenziok, M., Pulaski, S., Krueger, F., Zamboni, G., Clawson, D., & Grafman, J. (2011) Regional Brain Atrophy and Impaired Decision Making on the Balloon Analog Risk Task in Behavioral Variant Frontotemporal Dementia. Cognitive and Behavioral Neurology, 24(2), 59-67. doi:10.1097/WNN.0b013e3182255a7c. [ Links ]
Strauss, E., Sherman, E., & Spreen, O. (2006). A compendium of neuropsychological tests: Administration, norms, and commentary (3rd ed.) (pp. 32-37). NY: Oxford University Press. [ Links ]
Van Noordt, S. & Good, D. (2011). Mild head injury and sympathetic arousal: Investigating relationships with decision-making and neuropsychological performance in university students. Brain Injury, 25(7-8), 707-716. doi:10.3109/02699052.2011.580312. [ Links ]
Young, S., Gudjonsson, G., Carter, P., Terry, R., & Morris, R. (2012). Simulation of risk- taking and it relationship with personality. Personality and Individual Differences, 53, 294-299. doi:10.1016/j.paid.2012.03.014. [ Links ]

