










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkInternational Journal of Psychological Research
Print version ISSN 2011-2084
int.j.psychol.res. vol.9 no.1 Medellín Jan./June 2016
Design and psychometric analysis of the Hopelessness and Suicide Ideation Inventory "IDIS"
Diseño y análisis psicométrico del Inventario de Desesperanza e Ideación Suicida IDIS
Ronald Alberto Toro Tobara,*, Bertha Lucía Avendaño Prietoa and Diego Alonso Castrillona
a Facultad de Psicología, Universidad Católica de Colombia, Bogotá, Colombia.
Corresponding author. Ronald Aberto Toro, Facultad de Psicología, Universidad Católica de Colombia, Bogotá, Colombia. Email ddress, tororonald@gmail.com
Article history: Received: 15-04-2015 Revised: 29-10-2015 Accepted: 1-12-2015
ABSTRACT
The objective was to design the Hopeless and Suicide Ideation Inventory, also know as IDIS - Sp anish acronym for inventario de Desesperanza e ¡deación Suicida - and to analyze its psychometric properties. A quantitative empirical research was conducted employing a non-experimental design, an instrumental variable and cross-sectional analysis. Ihree hundred and thirty-nine people participated in the study (67.6% females, 31.6% males), in which 54.6% were students and 34.8' % were employees. Participants completed the IDIS, the Beck Depression Inventory (BDI-II), the Po sitive and Negative Suicide Ideation Inventory, and the Beck Hopelessness Scale. The results indicated an inter-rater reliability and a positive convergent validity in both scales. Suicidal ideation revealed an internal consistency of α = .76, and α = .81 for hopelessness; a total variance of 41 .77% and 47.52% was obtained correspondingly. Based on the Item Response Theory (IRT), the adjustments for INFIT and OUTFIT fell under the expected range. It was concluded that the IDIS is a reli able and valid measure, however, further evaluations on sensitivity and specificity are encouraged.
Key words: Suicide, Suicidal ideation, Hopelessness, Psychometric, Classical Test Theory and Item Response Theory.
RESUMEN
Se diseñó el Inventario de Desesperanza e Ideación Suicida "IDIS" para identificar Ideación Suicida (IS) y Desesperanza (DS). El estudio fue cuantitativo, no experimental instrumental. Participaron 339 personas (67.6% mujeres y 31.6% hombres), entre estudiantes (54.6%) y empleados (34.8%), el 50.4% pertenecía a estrato medio-bajo. Los instrumentos aplicados fueron el IDIS, BDI-II, PANSI y BHS. Los re sultados obtenidos indicaron favorable armonía interjueces y validez convergente en ambas escalas. En IS se obtuvo una consistencia interna α = .77 con tres factores que explican el 57.87% de la varianza. En la escala DS se obtuvo un α = .86 con dos factores que explican el 57.32% de la varianza. Desde la TRI los ajustes en INFIT y OUTFIT quedaron en el rango esperado. Se concluye que el IDIS puede ser usado como medida confiable y válida, aunque se sugiere revisiones posteriores con la escala IS y estudios de sensibilidad y especificidad.
Palabras clave: Suicidio, Ideación suicida, Desesperanza, Psico metría, TCT y TRI.
1. INTRODUCTION
Suicide is defined as the act that results in fatal outcomes, it is anticipated and carried out by a person who aims to obtain a desirable change WHO, W orld Health Organization, 2012). To the International Classification of Diseases ICD-10 (OMS, 1992), suicide is caused by self-inflicted harm, deliberately initiated by a person as a means to obtain a desired, conscious, and social outcome, resulting from the interaction of biological, genetic, psychological, sociological, cultural, and environmental factors (OMS, 2006).
Reported to be the tenth cause of death worldwide, the World Health Organization recognizes suicide as a public health issue with a rate of 16 deaths per 100,000. It is estimated that this phenomenon occurs every 40 sec onds, and for each of these deaths there are 20 failed attempts. It is projected that suicide rates will increase by 50% by 2020, the total percentage of cases worldwide. According to the 2013 Forensis report of the National Institute of Legal Medicine and Forensic Sciences (INML, 2014) in Colombia, suicide ranked as the fourth most violent cause of death in the country, with a rate of 3.84 per 100,000 (1,810 cases). In 2011, suicide deaths increased by 7% resulting in 1,889 cases, with a suicide rate of 4.1 per 100,000 (2009, 2010, and 2011). These records represent a growing annual increase tendency of 0.21 % and 3.9% in the last seven years (Macana, 2011).
In 2002, the Pan A merican Health Organization included in its annual report suicidal behavior as a form of self-inflicted violence (OPS, 2002), and it was defined as "any driven action, directed implicitly or explicitly, with the sole purpose to commit suicide, including any intention, ideation, or thought that can lead to said purpose, even when there is no clear manifestation of suicide" (SDSRS-MS, 2012; p. 43).
This construct includes suicidal ideation (IS) - Spanish acronym for ideación suicida - which has been defined by the OMS as passiv e thoughts about wanting to died, or active thoughts of killing oneself; thoughts of preparation for suicide are not displayed In other words, thoughts or ideas of serving as an agent of death itself, which expresses the desire or intention of dying, can vary in severity depending on the specificity of the suicide plan and the degree of intent.
It has been identified that suicidal ideation is highly correlated with depressive disorders, that is to say, levels of IS increase considerably in acute symptoms of depression, which can lead to the act of committing suicide. Suicide increments have been recorded at mid, lower, and subclinical symptomatic levels of depression (Cukrowicz, et al., 2011). IS has been associated with different risk factors such as being a woman, being isolated, low academic performance, financial and interpersonal problems, hopelessness, vulnerability, and chronic pain (Abel, Sewell, Martin, Bailey-Davidson, & Fox, 2012; Cukrowicz, et al., 2011).
From a psychopathology perspective to the cognitive models derived from the information processing paradigm, including cognitive theories and cognitive therapy (Clark, Beck, & Alford, 1999), suicidal ideation according to Wenzel, Brown, and Beck (2009) is established as the manifestation of "thoughts, images, beliefs, voices, or other cognitions reported by the individual about intentionally ending his or her own life" (p. 18). Based on the cognitive theory of suicide and derived from the explanatory model of depression, IS is determined as "an extreme expression of the desire to escape from what appears to be insolvable problems or an unbearable situation" (Rush & Beck, 1978; p. 202). IS is the byproduct of the interaction between the components of the cognitive triad (negative view of the self, world, and future) and the cognitive distortion that results from biased information processing (Jager-Hyman, Cunningham, W enzel, Mattei, Brown, both components derive from the activation of dysfunctional schemes (Beck, Rush, Shaw, & Emery, 1979; Rush & Beck, 1978), a high risk factor to unipolar depression (Stoep, et al., 2011) and suicide attempts Brown, Berchick, & Steer, 1990).
Cognitions of hopelessness are presented within the dysfunctional cognitive contents found prior to the onset of IS. Hopelessness (DS) - Spanish acronym for desesperanza - is defined as a perspective or a wide range of negative future expectations (Clark, Beck, & Alford, 1999; Beck, Rush, Shaw, & Emery, 1979) in which case, if high levels are presented it can lead to isolation and the search for interpersonal assistance (Henriques, Beck, & Brown, 2003); an aspect that is significantly correlated with suicidal behavior (Beck, Brown, Berchick, & Steer, 1990). In later reviews, Wenzel, Brown, and Beck (2009), defined hopelessness as a cognitive ideation about the future, where problems are viewed as unsolvable and are derived from the activation of a suicidal scheme. Hopelessness has also been associated with the future component of Beck's model of cognitive triad (Beck, 1976; Abramson, Metalsky, & Alloy, 1989). Future expectation associated to negative outcomes and the individual's negative inferential style (global, stable, personal, and internal) are in turn derived from erroneous perceptions of what causes a given event (mediator). These perceptions are unrealistic and extreme, and it can lead the individual to poses an embellished view of challenging situations as much difficult to solve, resulting in a prolonged and indefinite suffering (negative view of the future). Also, there are tendencies to attribute the outcomes to mistakes and personal defects (negative view of the self), and to view the world as a place of high demands, insuperable obstacles, and unattainable goals (Possel & Thomas, 2011; Beck, Rush, Shaw, & Emery, ). Cases of affective bipolar disorder have recently reported that IS is associated with high levels of self-criticism, rumination, and negative cognitive stiles (Stange et al., 2015), supporting the cognitive model and the role of IS and DS in suicidal behavior.
1.1 Asses sment of suicidal behavior
W hen evaluating an individual with high suicidal risks, it is important not only to identify maladaptive cognitive processes (e.g. perceptual and confirmation bias, congruent memory, attentional focus, etc.) and dysfunctional beliefs (e.g. rules, attitudes, automatic thoughts, core beliefs, etc.), but also to consider the cognitive processes that are found when assessing depression (Batterham, Calear & Christensen, 2013). Nev ertheless, a review of the schematic content presented in suicidal behavior must be conducted, which for the purpose of this research suicidal ideation (IS) and hopelessness (DS) were considered.
Grounded in the cognitive model, one of the most implemented psychometric measures is the Scale for Suicide Ideation (SSI) (Beck, Kovacs, & Weis sman, 1979; Beck, & Steer, 1991). Accord ing to its correlation with other instruments this measure reports a high reliability (r scores are between .83 and .98); similarly, are the items on the BDI (Beck Depressi on Inventory) (Beck, Ward, M endelson, Mock Erbaugh, 1961 ) and the HRSD (H amilton Rating Scale for Depression) (Wenzel, Brown, & Beck, 2009).
Another well-known measure is the Suicidal Ideation Questionnaire (SIQ) developed by Reynolds (1987). T his test assesses the frequency and intensity of suicidal thoughts and suicidal behaviors. Reynolds (1991) rep orted a test-retest reliably measure (r - .86) and significant correlations between measures of depression, hopelessness, anxiety, and self-esteem (r - .38 and .60).
In Colombia, Villalobos-Galvis (2010) adapted the Positive and Negative Suicide Ideation Inventory (PANSI; O sman, Gutiérrez, Kopper, Barrios, & Chiros, 1998), which contains 14 items on suicide thoughts presented in the last two weeks. The measure uses a 0 (never) - 4 (always) rating scale and scores in a tw o -factor structure that illustrated the 64% of the total variance: protective thoughts against suicide and suicide ideation. The PANSI obtained an adequate reliability index (α - .90; negative ideation α - .93, and positive ideation α - .84), and appropriate correlations (p < .01) between the hopelessness, depression, IS, and self-esteem measures. Using a sample of 676 students of eight, ninth, tenth, and eleventh grade from three different cities of the region of Boyacá (Colombia), Avendano, Pérez, Vianchá and Martínez (2014) performed a psychometric analysis using the PANSI scale adapted by Villalobos. The results indicated an internal consistency of .83 and a factorial structure consistent with the framework.
Another measure designed to identify suicidal ideations and its prediction of suicide attempts is the Beck Ho pelessness Sc ale (BHS). This measure is key component to predict suicide ideation and suicide attempts, especially in adults with depression (Shahar, Bareket, Rudd, & Joiner, 2006). The BHS was developed by Beck, Weissman, Lester and Trexler (1974) to evaluate the degree of negative expectations part of an active suicide scheme. These are presented in three factors: feelings about the future, loss of motivation, and future expectations.
In the analysis of the main components of the BHS conducted by Dyce (1996), three factors were reported: expectations of success, failure, and uncertainty about the future. A year later, Steer, Beck, and Brown (1997) c oncluded that BHS was composed of two factors: pessimism about the future and resignation. They used a 20 -item scale that included true-false questions of approximately 5 minutes of duration. As for the psychometric properties, there was a reliability of KR-20 - .87 to .93 and a test-retest stability of one week of r - .69 in psychiatric samples; α r - .85 was revealed in college samples. It is important to emphasis that due its valid predictable characteristics (eight points or higher increase the possibility of suicide attempt by four times) and sensitivity to change (Brown, Beck, Steer, & Grisham, 2000), high scores in the BHS have been recognized as a suicide risk factor in different samples.
Considerably, aside from being a significate component of suicidal behavior, hopelessness has also been measured as one of the comprising factors of hopelessness depression, as it was presented in the Ho pelessness Depression Symptoms Questionnaires (HDSQ) developed by Metalsky and Joiner (1997). The HDSQ is α measure that indicates high internal consistency (α - .93), where SI becomes part of one of the nine evaluated factor, suicidal ideation/impulse subscale (α - .86).
The construct validity analysis demonstrated the applicability of the measures to specific regions of the country that hinder its general use; the PANSI and the BHS were validated, however, only one measure per region was employed (Pasto and Bogotá correspondingly ). While the BHS construct validity previously adapted did not correlate with the three components reported in the BHS, some items presented factorial loads in more than one factor, which could have compromised the factorial purity of the test. These implications suggest the development of a useful measure that is able to evaluate IS and DS in the Colombian population. This can be accomplished by combining theoretical and empirical characteristics of instruments that contain an appropriate index of internal consistency and validity.
Therefore, the aim of the present research study was to design the Hopeless and Suicide Ideation Inventory (IDIS) and establish its psychometric properties. The IDIS is a unique measure based on an existing theoretical model of psychopathology, empirically supported, and methodologically organized according to the standards required by the scientific community.
2. METHOD
2.1 Study and type of research
This study is a quantitative empirical research employing a non-experimental design and an instrumental variable and cross-sectional analysis, intended to establish the psychometric properties for the instrument designed (Montero & León, 2007 .
2.2 Participants
The sample consisted of 339 p articipants who volunteered from three different regions of the country (Cundinamarca, Antioquia, and Boyacá). In order to decrease Type I and Type II errors, the underlying assumptions to establish the construct validity of the exploratory factor analysis, such as having 10 participants for each item, were followed (McCallum, Wid aman, Zhang, & Hong, 1999). Each participant answered the measure under appropriate conditions, bearing in mind the code of ethics under the Law 1090 of 2006 for professional in the field psychology in Colombia. A contingency plan was taken into account in case any participant presented high levels of IS or reported previous suicide attempts. If necessary participants were immediately referred to the university's Outpatient Unit of Psychological Services where the research was conducted.
2.3 Measures
2.3.1 Suicide ideation measure
Positive and Negative Suicide Ideation Inventory, PANSI.
The version adapted by Villalobos-Galvis (2010) was implemented. This measure presented an index of internal consistency of α = .89 and was rated by adding the total item scores; the higher the score obtained the higher the suicide ideation.
2.3.2 Hopelessness measure
Beck Hopelessness Scale, BHS The version adapted in Spanish by Mikulic, Cassullo, Crespi and Marconi (2009) was used. This measure contains 20 true-false items that should be answered based on the cognitions associated with negative expectations for the immediate and long term future. The first nine items evaluate lack of motivation, the following six measure future expectations, and the last five inquires about feelings about the future.
2.3.3 Depression measure
Beck Hopelessness Inventory in Spanish – Second Edition, BDI-II.
The BDI-II was adapted to Spanish by Brenlla and Rodríguez (2006), but originally developed by Beck, Steer and Brown (2006). This measure is designed to evaluate the severity of depressive symptoms according to the DSM-IV (American Psychiatric Association, APA, 1994) and is composed of 21 items that are scored based on the severity of the symptoms in the last week. This measure is well-known not only for its high internal consistency (α = .94 and α = .88 in a previous analysis of major depression), but also for its significant correlation between depression, hopelessness, and IS (Cukrowicz, et al., 2011). Also, this instrument has demonstrated to be useful when detecting suicide risk in patients that report a high score in items 2 and 9, resulting as an indicator of convergence with hopelessness (i.e. item 2: pessimism) and IS (i.e. item 9: suicidal thoughts or wishes).
3. ANALYSIS
A descriptive analysis was conducted to examine the social-demographic data and the direct scores of the implemented measures. Then a psychometric analysis under the test classical test theory (CTT) was completed for piloting as well as for the applicability of the total sample. The content validity was obtained by consensus of 10 exp erts using the coefficient rwg (Finn, 1970). As for the criterion validity, a concurrent validity procedure was used based on the correlations between the IDIS and the PANSI plus the total score of the BDI-II, the Hopelessness Scale and the BHS, and finally the IS and the PANSI. An Exploratory Factor Analysis (EFA) was conducted to establish the construct validity and identify three underlying factors established by the test plan. In the EFA, the factor loading of each item was revised. The data presented in Bartlett test obtained a factorial structure, resulting in a significant and high levels of intercorrelation between the variables; according to the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy these had to be higher than .70.
A Confirmatory Factor Analysis (CFA) was employed for the one-dimensional model of each scale; the following criteria was used: the chi-square (X2) was used as an independent indicator of the model that should be significant (p < .05), the ratio of chi-square X2 to the degrees of freedom (CMIN/DF) that should be lower than 3, the comparative fit index (CFI) and the global goodness-of-fit index (GFI) that should be higher or equal to .95, and the root mean square error of approximation (RMSEA) that should fall between .05 and .08 (Hu & Bentler, 1995).
In order to conduct a Rash analysis following the IRT, previ ous assumptions required by this model were verified: local independence and one-dimensional. These were compared with the EFA and CFA, where the items with loading factors greater than .40 guaranteed the one-dimensional assumption, presenting an explained variation that, as specified by Reckase (1979), should exceed 25% in the first factor for each of the subscales in the inventory. Once the assumptions for the IRT were confirmed, the OUTFIT and the INFIT were identified using W insteps 3.69.1.13.; these should range between 0.7 and 1.3 (Barbosa & Reyes, 2007). Finally, a differential item functioning analysis (DIF) was employed in order to minimize Type I error in each scale of the IDIS (Gómez- Benito & Hidalgo-Montesinos, 2003). A X2 test was calculated for each group, proposing a null hypothesis of equality of the parameters obtained for each population group; this procedure was conducted by Lord (1980). Add itionally, to confirm whether there were any significant statistical differences at the p .05 level between the groups, the Mantel-Haenszel (MH) method (Mantel & Haenszel, 1959) was implemented; this measure requires the effect size to be greater than .25 in a confidence interval of 95%.
4. RESULTS
4.1 Descriptive results
The sample originally included 350 participants, however, 11 of the records were excluded due to inadequate completion of the measures. The mean age of participants was 27.72 years (SD - 12.15). Of the total number of participants 67.6% were females and 31.6% were males. Most of the participants were single (64.9%), 54.6% were students, and 34.8% reported to be employees. Participants also reported to come from a low (29.8%), lower-middle (50.4%), and middle (9.7%) soci o-economic status. These percentage distributions are consistent with the latest statistics report using the Mental Health Survey developed by the Ministry of Health and Social Protection & Colciencias (2015). Further, the BHS obtained a coefficient of α - .75, the PANSI &alp - .81, and the BDI-II α - .88; these were reliable indicators of measures.
4.2 IDIS Psychometric Analysis
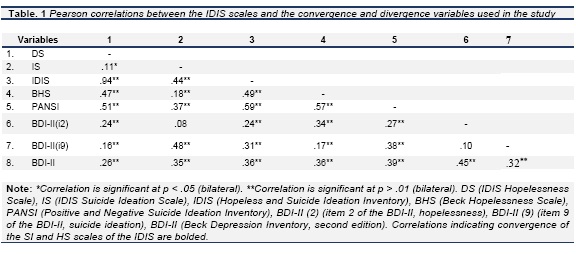
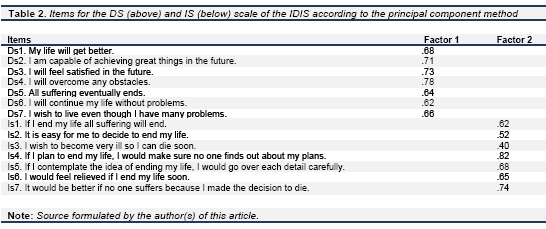
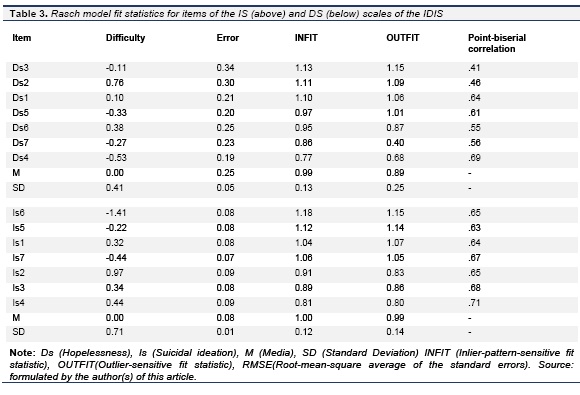
Using the Cronbach's Alpha, the IS scale revealed an internal consistence of α - .76, while the DS scale re sulted in a coefficient of α - .81. The criterion validity of the IS and DS was obtained through concomitant measures. Pearson's r revealed significant correlations for both scales of the IDIS as shown in Table 1. Significant sampling adequacy was found in both the KMO test and Bartletts Test of Sphericity. In other words, the composition of the data presented an adequate variance and was viable for the EFA. The DS scale displayed a significant factor that explains 47.52% of total variance. Table 2 shows the items for each scale of the IDIS. T he adjustment indicators employed in the CFA for the IS scale pres ented values of X2 - 25.24 (gl - 14, p - 0.03), CMIN/DF - 1.80, GFI - .98, CFI - .98 and RMSEA - .049. This data confirmed that the one-dimensional model of the IS scale with seven items revealed a favorable fit. Likewise, the DS scale also with seven items presented an acceptable one-dimensional adjustment with values of X2 - 38.06 (gl - 14, p - 0.01), CMIN/DF - 2.71, GFI - .97, CFI - .96 and RMSEA - .072. T he results of the EFA and the CFA complied with the one-dimensional characteristics of each scale. Table 3 illustrates the goodness-of-fit criterions of the Rasch model for each scale. The items for the IDIS were adapted to the parameters of the Rasch model in such a way that the INFIT for the items of the IS scale r anged from 0.81 to 1.18 (M - 1.00, SD- 0.12), and for the OUTFIT between 0.80 and 1.15 (M - 0.99, SD - 0.14), whereas the DS scale reported an INFIT r anging from 0.77 and 1.13 (M - 0.99, SD - 0.13), and the OUTFIT between 0.40 and 1.15 (M - 0.89, SD - 0.25). W hile the measure for parameter b of the IS scale r anged from 0.97 (item Is2) and 1.41( item Is6) logits, the DS scale pres ented a parameter b that ranged from 0.76 ( item Ds2) and -0.53 (item Ds4) logits. Also, biserial correlations were above .25, between .41 and .69, which indicates that they were above acceptable margins (Barbosa & Reyes, 2007).
The information function for each scale of the IDIS was estimated. In order to achieve an approximate consensus of the empirical and theoretical CCI's of each item, a goodness-of-fit test was implemented, which was favorable for the items of the DS and IS scales. In other words, the empirical data demons trated correlations between levels of traits (suicidal ideation and hopelessness) and the probability to answer the item while presenting a risk factor (Attorresi, Lozzia, Abal, Galibert, & Aguerri, 2009; Barbosa & Reyes, 2007). T he information function of the IS scale indicated that the maximum amount of information provided in the test is between Θ= -1.5 and Θ- 1.5 logits, and decreases at extreme scores. It can be stated that the IS scale is more accurate in measuring the construct IS between -1.5 and 1.5 logits. As for the DS scale, accuracy is found between Θ= -2 and Θ =2 logits. W hile response categories presented a favorable distribution for each possible answer in the DS scale, separations between alternatives 1 "I've thought about it occasionally" and 2 "I've thought about it often" in the IS scale suggest that participants had a tendency to answer in a dichotomous and differential way without intermediate categories in the trait levels of items Is2 and Is3.
Concurrently, no statistical significant differences were found in gender. Since the effect size was within the expected range (p. < .25) there was no DIF, with the exception of the items in the IS scal e with the indicator HS ( antel & Haenszel, 1959' in the item Is1 (p. - .027) and 30 (p. = .017). In regards to the x2 of Lord (1980), item Is5 was observed as the only one to reveal a statistical significant difference (X2 - 6.4407, gl - 1, p. - .01), therefore, the idea that this item measures the latent trait in men and women differently is supported. Ihe items in the DS scale did not report a statistical significant difference between men and women, neither in the HS factor nor the X2 of Lord. The probability was reported as p. - 43 and p. - .89, exceeding the expected minimum standard.
5. DISCUSSION
The objective of the present study was achieved; both of the scales implemented in the inventory are presented through a one-dimensional model and include the cognitive constructs, proposed by Wenzel, Brown, and Beck (2009), of hopelessness and suicidal ideation linked to high suicidal risk (Abel, Sewell, Martin, Bailey-Davidson, & Fox, 2012; Stoep, et al., 2011; Reinecke, Wa shburn, & Becker-Weidman; 2007; Shahar, Bareket, Rudd, & Joiner, 2006; Rush & Beck, 1978).
W hile employing an analysis based on the CTT, the IDIS revealed sampling adequacy and an appropriate factorial structure for both scales. Based on the internal consistency obtained for each scale (α - .76 in IS and α - .81 in DS), the IDIS is considered a reliable instrument to measure cognitive variables of suicidal behavior: IS and DS. The OUTFIT and INFIT measures for each item were within the parameters suggested by different authors (e.g. Muñiz, 2010; Attorresi, Lozzia, Abal, Galibert, & Aguerri, 2009; Barbosa & Reyes, 2007; K ohan, owever, the item Ds7 demonstrated a low adjustment in the OUTFIT; the standardized score was verified (OUTFIT ZSTD = -0.8), which ranged between -1.9 and 1.9; this is a data indicator that "allows reasonable predictions" (Linacre, 2002, p. 878), therefore the item was preserved.
Likewise, the separation index between the items indicated that the IS scale of the IDIS showed low discrimination among people who presented this trait, even though its approximation was near the suggested minimum (> 2). Similarly, the separation among people for the DS was 1.87 and for IS was 0.00. According to Linacre (1999), this is an unreliable indicator for discrimination among people for the IS scale since there is no fit to the parameter. From the IRT, these results suggest two findings; while the IS scale is not accurate to evaluate the trait from the IRT, the items in the DS scale adjusted to the expected parameters of difficulty and discrimination as suggested by Muniz (2010, 1997), pres enting an alignment of the items to the latent trait (hopelessness). This is a relevant aspect when considering cognitive symptoms of depression in a clinical context.
Due to the preliminary nature of the study, the results for both scales are interpreted as introductory, and normative comparisons are stablished based on the raw scores of each scale. The scores for the DS scale were studied using an accumulative frequency graph where the 10 points equivalent to 0.0 logits are reached around the 75th percentile. Therefore, it can be stated that based on the discrimination parameter of this scale, it is a significate score starting at 10 p oints. In the IS scale, the 98th percentile is reached at 0.0 logits with a score of 9, however, when the curves of the tests are observed in the graph, the upper percentiles are reached differently in both scales. For instance, the 96th percentile is reached after 3 points in the IS scale, where the same percentile in the DS scale is reached at 17 points. These results are attributed to the fact that a clinical sample was not included in the study, which indicates a significant drop in scores in extreme categories. This can serve as a screening method to detect individuals with high suicide risk. Clinical samples should be considered in future research studies.
6. LIMITATIONS
The above IDIS psychometric properties should be considered in light of the following limitations. First, it was found that the inverse items designed to evaluate hopelessness presented an adequate adjustment in both the CTT and IRT; this can be corroborated through the cognitive models supporting schematic activation and the primacy of suicide tendencies presented in suicidal behavior. Wenzel, Brown, and Beck (2009) indicated that suicidal tendencies lead to bias information processing where attentional processes are geared toward approving confirming cues while ignoring disapproving signals that part from dysfunctional content. This is achieved through the schematic conservation processes (Young, Klosko, & Weishaar, 1994) or the generation of defensive strategies (Beck J. S., 2005), where denying the content can be a source of variance in the evaluation presenting a heavy emotional burden for the individual. This constitutes a potential source of error for the development of the instrument and could justify why the responses of the items assessing hopelessness with reverse format had a better fit in terms of the construct validity based on the EFA. Coincidentally was the case of the direct and indirect items presented in BHS and other instruments that measure DS (e.g. González, 2009; Mikulic, Cassullo, Crespi, & Marconi, 2009).
Difficulties were presented when separating items from participants in the IS scale, a s well as in the information function of the response categories. In order to ensure advancement with enough separation and monotony in the assigned sequence of each trait in each answer choice, these are estimated from the data presenting a better response if they were to have a dichotomous answer format in the IS scale and three answer choice in the DS scale. This process will decrease the errors of each step for each category, preferably adjusting to the thresholds of Rash-A ndrich (Andrich, 1978; Andrich, 1978b). Lik ewise, this suggestion would go in accordance with Asún and Züñiga (2008) who recommend to use the Response Pattern of Graded Scores Model (Samejima, 1969) for its practical and functional characteristics when measuring social attitudes and evaluating if the answer choices are structuring the measure.
In regards to the differential item functioning, it was found that for the IS scale sex pres ented variations when measuring items Is1 ("If I end my life all suffering will end") and item Is5 ("If I contemplate the idea of ending my life, I would go over each detail carefully").
These results suggest further research with clinical samples by gender. However, results obtained in the present study support previous findings on IS and female gender bias (e.g. Gau, Chin-Hung, Charles, Jung-Chen, & Andrew, 2009; Cukrowicz, et al., 2011; Suominen, Isometsa, Ostamo, & Lonnqvist, 2004); among the Colombian population, no significate differences have been reported from the ministry of social protection as it was stated in 2003 ( et al., 2009). These recommendations will allow future development of specify and sensitivity analysis for the measure to determine their appropriate clinical use.
To conclude, the IDIS is a measure reliable and valid in development. It reveals a set of psychometric properties that should be reconsidered in future confirmatory analysis in order to ensure a more accurate measure, in particular the IS scale, gr ounded in the cognitive model to evaluate suicidal behavior.
7. REFERENCES
Abel, W., Sewell, C., Martin, J. S., Bailey-Davidson, Y., & Fox, K. (2012). Suicide ideation in Jamaican youth: sociodemographic prevalence, protective and risk factors. ///es Indian Medical Journal, 61(5), 521-525. [ Links ]
Abramson, L. Y., M etalsky, G. I., & Alloy, L. B. (1989). Hopelessness Depression: Theory-Based subtype of depression. Psychological Review, 96(2), 358-372. [ Links ]
Alloy, L. B., A bramson, L. Y., W hitehouse, W. G., Hogan, M. E., Tashman, N. A., Steinberg, & et al. (1999). Depressogenic cognitive styles: Predictive validity, information processing and personality characteristics, and developmental origins. Behavior Research and Therapy, 37, 503-531. [ Links ]
American Psychiatric Association, APA. (1994). Diagnostic and statistical manual of mental disorders (4a. ed.). Washington, DC, EE. UU.: Author. [ Links ]
Andrich, D. (1978). Application of a Psychometric Rating Model to Ordered Categories Which Are Scored with Successive Integers. Applied Psychological Measurement, 2(4), 581-594. [ Links ]
Andrich, D. (1978b). A rating ordered response categories. 43, 561-573. [ Links ]
Asún, R., & Zúñiga, C. (2008). Ventajas Politómicos de Teoría de Respuesta la Medición de Actitudes Sociales. El Análisis de un Caso. PSYKHE, 17(2), 103-115. [ Links ]
Attorresi, H. F., Lozzia, G. S., Abal, F. J., Galibert, M.S., & Aguerri, M. E. (2009). Teoría de Respuesta al Item. Conceptos básicos y aplicaciones para la medición de constructos psicológicos. Revista Argentina de Clínica Psicológica, 18(2), 179-188. [ Links ]
Avendano, B. L., Pérez, M. P., Vianchá, M. A. & Martínez, L. C. (2014). Análisis P sicométric o de la Escala PANSI e Ide ación Suicida en Adolescentes. Documento en preparación derivado del proyecto de investigación titulado: Ideación suicida en adolescentes de Tunja, Duitama y Sogamoso. [ Links ]
Barbosa, Y., & Reyes, J. F. (2007). MINISTEPS. Obtenido de Universidad Nacional de Colombia. Facultad de Ciencias Económicas. Unidad de informática y comunicaciones: http://fce.unal.edu.co/wiki/images/2/2d/MiniSteps.pdf. [ Links ]
Batterham, P. J., Calear, A. L., & Christensen, H. (2013). The Stigma of Suicide Scale. Psychometric Properties and Correlates of the Stigma of Suicide. Crisis, 34(1), 13-21. [ Links ]
Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York: International University Press. [ Links ]
Beck, A. T., & Steer, R. A. (1991). Manual for the Beck Scale for Suicide Ideation. San Antonio, TX: Psychological Corporation. [ Links ]
Beck, A. T., Brown, R. J., Berchick, B. L., & Steer, R. A. (1990). Relationship between hopelessness and ultimate suicide: A replication with psychiatric outpatients. American Journal of Psychiatry, 147, 190-195. [ Links ]
Beck, A. T., Kovacs, M., & Weissman, A. (1979). Assessment of suicidal intention: The Scale for Suicide Ideation. Journal of Consulting and Clinical Psychology, 47(2), 343-352. doi: 10.1037/0022-006X.47.2.343. [ Links ]
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive Therapy of Depression . Nueva York: The Guilford Press. [ Links ]
Beck, A. T., Steer, R. A., & Brown, G. K. (2006). BDI II, Inventario de Depresión de Beck, (2 ed.). Edición en Español. Argentina, Buenos Aires: Paidós. [ Links ]
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An Inventory for Measuring Depression. Archives of General Psychiatry, 4(6), 561-571. Doi:10.1001/archpsyc.1961.01710120031004. [ Links ]
Beck, A. T., Weis sman, A., Lester, D., & Trexler, L. (1974). The measurement of pessimism: the hopelessness scale. Journal of Consulting and Clinical Psychology, 42, 861-865. [ Links ]
Beck, J. S. (2005). Cognitive therapy for challenging problems, what to do when the basics don t work. New York: The Guilford Press. [ Links ]
Brenlla, M., & Rodríguez, C. (2006). Manual de Inventario de Depresión de Beck BDI II. Adaptación Argentina. Argentina, Buenos Aires: Paidós. [ Links ]
Brown, G. K., Beck, A. T., Steer, R. A., & Grisham, J.R. (2000). Risk factors for suicide in psychiatric outpatients: A 20 -year prospective study. Journal of Consulting and Clinical Psychology, 68, 371-377. [ Links ]
Clark, D. A., Beck, A. T., & Alford, B. A. (1999). Scientific foundations of cognitive therapy and therapy of depression. New York: John Wiley y Sons. [ Links ]
Cukrowicz, K. C., Erin, F., Schlegel, B. A., Phillip, N. S., Jacobs, M. P., VanOrden, K. A., ... Joiner, T. E. (2011). Suicide Ideation Among College Students Evidencing Subclinical Depression. Journal of American College Health , 59(7),575-581. [ Links ]
Dyce, J. A. (1996). Factor structure of the Beck Hopelessness Scale. Journal of Clinical Psychology, 52, 555-558. [ Links ]
Finn, R. H. (1970). A note to estimating the reability of categorical data. Educational and Psychological Measurement, 30, 71-76. [ Links ]
Gau, S., Chin-Hung, C., Charles, L., Jung-Chen, C., & Andrew, C. (2009). Development of a Chinese version of the Suicide Intent Scale. Suicide and Life - Thre atening Behavior, 39(3), 332-342. [ Links ]
Gómez-Benito, J., & Hidalg o-Montesinos, M. D. (2003). Desarrollos recientes en psicometría. Avances en Medición, 1(1), 17-36. [ Links ]
González, C. E. (2009). Propiedades psicométricas de la escala de desesperanza de Beck en una muestra bogotana. Psychologia, avances de la disciplina, 3(2), 17-30. [ Links ]
Henriques, G., Beck, A. T., & Brown, G. K. (2003). Cognitive therapy for adolescent and young adult suicide attempters. The American Behavioral Scientist, 46(9), 1258-1268. [ Links ]
Instituto Nacional de Medicina Legal -INML. (1 de septiembre de 2014). Medicina legal. Obtenido de http://www.medicinalegal.gov.co/documents/10180/145695/presentacion+forensis2014.pdf/3b0aa016-1a19-4322-9cf3-a9b9fd985978. [ Links ]
Hu, L. & Bentler, P. (1995). Evaluating model fit. In R. Hoyle (Ed.), Structural equation modelling, Concepts, issues and applications (pp.76-99). Thousand Oaks, CA: Sage Publications. [ Links ]
Jager-Hyman, S., Cunningham, A., Wenzel, A., Mattei, S., Brown, GK., & Beck, A. T. (2014). Cognitive Distortions and Suicide Attempts. Cognitive Therapy and Research, 38(4), 369-374. Doi: 10.1007/s10608-014-9613-0. [ Links ]
Kohan, N. (2004). Teoría de Respuesta al Item: Supuestos Básicos. Evaluar, 4, 95-110. [ Links ]
Linacre, J. M. (1999). Investigating rating scale category utility. Journal of Outcome Measurement, 3(2), 103-122. [ Links ]
Linacre J. M. (2002). What do Infit and Outfit, Mean-square and Standardized mean?. Rasch Measurement Transactions, 16(2). Available at http://www.rasch.org/rmt/rmt162f.htm. [ Links ]
Lord, F. M. (1980). Applications of item response theory to practical testing problems. Hillsdale, New Jersey: Lawrence Erlbaum Associates Publishers. [ Links ]
Macana, N. L. (2011). Comportamiento del suicidio en el 2011, FORENSIS. Bogotá, D.C., Colombia.: Instituto Nacional de Medicina Legal y Ciencias Forenses. [ Links ]
Mantel, N., & Haenszel, W. (1959). Statistical aspects of the analysis of data from retrospective studies of disease. Journal of the national cancer institute, 22, 719-748. [ Links ]
McCallum, R. C., Widaman, K. F., Zhang, S., & Hong, S. (1999). Sample size in factor analysis. Psychological Methods , 4(1), 84-99. [ Links ]
Metalsky, G. I., & Joiner Jr., T. E. (1997). The Hopelessness Depression Symptom Questionnaire. Cognitive Therapy and Research 21, 359-384. [ Links ]
Mikulic, I. M., Cassullo, G. L., Crespi, M. C., & Marconi, A. (2009). Escala de Desesperanza BHS (A. Beck, 1974): estudio de las propiedades psicométricas y baremización de la Adaptación Argentina. Anuario de investigaciones, 16, 365-373. [ Links ]
Ministerio de Salud y Protección Social & Colciencias (2015). Encuesta nacional de salud mental 2015. Tomo 1. Disponible en http://www.odc.gov.co/Portals/1/publicaciones/pdf/consumo/estudios/nacionales/CO031102015-salud_mental_tomoI.pdf. [ Links ]
Montero, I., & León, O. (2007). Guía para nombrar los estudios de investigación en Psicología. International Journal of Clinical and Health Psychology, 7, 847-862. [ Links ]
Muniz, J. (1997). Introducción a la teoría de respuesta al ítem. Madrid: Pirámide. [ Links ]
Muniz, J. (2010). Las teorías de los test: Teoría clásica y teoría de respuesta a los ítems. Papeles del Psicólogo, 31(1), 57-66. [ Links ]
OMS, Organización Mundial de la Salud. (1992). CIE 10. Trastornos mentales y del comportamiento. Décima revisión de la Clasificación Internacional de las Enfermedades. Descripciones Clínicas y pautas para el diagnóstico. Ginebra: OMS. [ Links ]
OMS, Organización Mundial de la Salud. (2006). Prevención del suicidio recurso para consejeros. Departamento de salud mental y sustancias trastornos mentales cerebrales. Ginebra: OMS. [ Links ]
OPS, Organización Panamericana da Salud. (2002). Informe mundial sobre la violencia y la salud, /orld Report on Violence and resumen. Health, Summary. Washington, D.C.: Organización Panamericana de la Salud, Oficina Regional para las Américas de la Organización Mundial de la Salud. [ Links ]
Osman, A., Gutiérrez, P., Kopper, B., Barrios, F., & Chiros, C. (1998). The positive and negative suicide ideation inventory: Development and validation. Psychological reports, 82, 783-793. [ Links ]
Posada-Villa, J., Camacho, J. C., Valenzuela, J. I., Arguello, A., Cendales, J. G., & Fajardo, R. (2009). Prevalence of Suicide Risk Factors and Suicide-Related Outcomes in the National Mental Health Study, Colombia. Suicide and Life-Threatening Behavior, 39(4), 408-424. [ Links ]
Possel, P., & Thomas, S. D. (2011). Cognitive Triad as Mediator in the Hopelessness Model? A Three-Wave longitudinal study. Jo urnal of Clinical Psychology, 67(3), 224-240. [ Links ]
Reckase, M. D. (1979). Unifactor latent trait models applied to multifactor test: Results and implications. Journal of Educational Statistics, 4(3), 207-230. [ Links ]
Reinecke, M. A., Washburn, J. J., & Becker-Weidman, E. (2007). Depression and Suicide. En F. M. Dattilio, & A. Freeman, Cognitive-behavioral strategies in crisis intervention (pp 25-67). New York: The Guilford Press. [ Links ]
Reynolds, W. M. (1987). Suicidal Ideation Questionnaire! Professional Manual. USA, Florida: Psychological Assessment Resources. [ Links ]
Reynolds, W. M. (1991). Psychometric Characteristics of the Adult Suicidal Ideation Questionnaire in College Students. Journal of Personality Assessment, 56(2), 289-307. [ Links ]
Rush, A. J., & Beck, A. T. (1978). Cognitive Therapy of Depression and Suicide. American Journal of Psychotherapy, 32(2), 201-219. [ Links ]
Samejima, F. (1969). Estimation of latentability using a response grades scores. Psychometrika Monograph, 17. Recuperado el 21 de 9 de 2014, de https://psychometricsociety.org/sites/default/files/pdf/MN17.pdf. [ Links ]
Secretaría de Determinantes de la Salud y Relaciones Sanitarias & Ministerio de la Salud de la Nación (SDSRS-MS). (2012). Lineamientos para la Atención del Intento de Suicidio en Adolescentes. Buenos Aires, Argentina: DCV Anahí Maronas. [ Links ]
Shahar, G., Bareket, L., Rudd, M. D., & Joiner, T. E. (2006). In severely suicidal young adults, hopelessness, depressive symptoms, and suicidal ideation constitute a single syndrome. Psychological Medicine , 36, 913-922. [ Links ]
Stange, J. P., Hamilton, J. L., Burke, T. A., Kleiman, E. M., O'Garro-Moore, J. K., Sengman, N. D., Abramson, L. Y., & Alloy, L. B. (2015). Negative cognitive styles synergistically predict suicidal ideation in bipolar spectrum disorders: A 3-year prospective study. Psychiatry Research, 226(1), 162-168. Doi:10.1016/j.psychres.2014.12.042. [ Links ]
Steer, R. A., Beck, A. T., & Brown, G. K. (1997). Factors of the Beck Hopelessness Scale: Factor artifact? Multivariate Experimental Clinical Research, 11(3), 131-144. [ Links ]
Stoep, A., Adrian, M., Mccauley, E., Crowell, S. E., Stone, A., & Flynn, C. (2011). Risk for Suicidal Ideation and Suicide Attempts Associated with Co-occurring Depression and Conduct Problems in Early Adolescence. Suicide and Life-Threatening Behavior 41(3), 316-332. [ Links ]
Suominen, K., Isometsa, E., Ostamo, A., & Lonnqvist, J. (2004). Level of suicidal intent predicts overall mortality and suicide after attempted suicide: A 12 -year follow-up study. BMC Psychiatry, 4(II). DOI:10.1186/1471-244X-4-11. [ Links ]
Villalobos-Galvis, F. H. (2010). Validez y fiabilidad del Inventario de Ideación Suicida Positiva y Negativa - PANSI, en estudiantes colombianos. Universitas Psychologica, 9(2), 509-520. [ Links ]
Wenzel, A., Brown, G. K., & Beck, A. T. (2009). Cognitive therapy for suicidal patients. Scientific and clinical applications. Washington, DC: American Psychological Association. [ Links ]
WHO, World Health Org anization. (2012). For strategies evidence suicide prevention is there effectiveness? Copenhagen, Denmark: WHO Regional Office for Europe. [ Links ]
Young, Y. E., Klosko, J. S., & Weishaar, M. E. (1994). Schema therapy: a practitioner's guide. New York: The Guilford Press. [ Links ]

