











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink1. Introduction
Adolescence is a period of increased vulnerability to depression because of complex changes in biology, cognition, and social domains. According to the 2019 National Survey on Drug Use and Health (NSDUH), in 2018, 14.4% (3.5 million) of adolescents aged 12 to 17 in the United States had at least one major depressive episode (MDE), and 70% of these adolescents had an MDE with severe impairment. Adolescent depression is associated with a number of negative functioning. For example, depression may impair adolescents cognitive functioning, relationships with parents and peers, academic performance, and even suicide attempt (e.g., Clayborne et al., 2019). Moreover, depressed adolescents are more likely to develop depression in adulthood (Benjet et al., 2020; Rutter et al., 2006). For example, Johnson, Dupuis, Piche, Clayborne, and Colman (2018) found that adolescents with depression had 2.78 times increased odds of depression in adulthood. Not surprising, adolescent depression is also associated with poor outcomes in adulthood, such as low-income levels, low educational aspirations, and high substance use (e.g., Howard et al., 2019; McKenzie et al., 2010). Most clinical depression starts in middle adolescence, which makes it a particularly vulnerable time for adolescent depression. For example, one-year point prevalence rate of major depressive disorder (MDD) is much higher in middle adolescence (ages 15-18) than in early adolescence (ages 13-15) (Kessler et al., 2001). Given the severity, chronicity, and long-term negative consequences of depression in middle adolescence, it is important to investigate the protective factors of depression from early to middle adolescence.
Social skill deficit theory of depression (Lewinsohn et al., 1985) and competence-based theory of depression (Cole, 1991) illustrate that social skills are important protective factors for depression. According to social skill deficit theory of depression, social skill deficit is an antecedent of depression. On one hand, social skill deficit is associated with negative self-views of competence and worth in relationships, ineffective self-regulation abilities (e.g., lack of resilience), and high levels of perceived stress (Fehlinger et al., 2013; Schnell & Herpertz, 2018), which may directly contribute to depression. On the other, social buffering theories posit that social skill deficit may indirectly increase ones vulnerability to depression by reducing social support or positive social reinforcement (Cohen & Wills, 1985; Moeller & Seehuus, 2019; Nilsen et al., 2013), as social support acts as a buffer against stressful events. Especially for adolescents who spend much time with age-mates and put great stock in the expectations and opinions of peers, lack of social support from peers may particularly exacerbate adolescent depression. In addition, competencebased theory of depression also posits that, social skill, as a competence in social domain, is a protective factor of depression (Cole, 1991). According to this theory, individuals receive competence feedback from many informants and internalize the feedback into the perception of self, and self-perception function as a strong influencing factor of depression. Basedon it, adolescents with high levels of social skills would receive more positive feedback in social interactions, and the positive feedback helps them build a positive perception of self (e.g., I am liked by others), which may protect them from depression.
Although there aresubstantial empirical research studies demonstrating the association between social skills and adolescent depression (e.g., Feldman et al., 2017; Nilsen et al., 2013; Schiltz et al., 2018; Singh et al., 2019), there does not appear to be any work investigating how the change in social skills influence the change in depression from early to middle adolescence. As discussed above, the prevalence of adolescent depression increases dramatically in middle adolescence. Thus, in order to develop effective preventions for adolescent depression, researchers should not only depend on an understanding of the links between social skills and adolescent depression at given time, but also on an understanding of how the change in social skills is related with the change in adolescent depression from early to middle adolescence. In addition, the prior work has not paid sufficient attention to the different domains of social skills and their specific influences on adolescent depression. Social skill has been defined as a class of learned, socially acceptable behaviors across a wide array of functional domains that allow an individual to positively interact with others (Gresham et al., 2011). It is possible that different domains of social skills have different change trajectories and different influences on the change trajectory of depression. The current research focused on the domains of cooperation, assertion, responsibility, and self-control in social skills, based on the suggestion of Gresham and Elliott (1990). The research question in the current research was how the changes in cooperation, assertion, responsibility, and self-control influence the changes in depression from early to middle adolescence.
1.1 The Current Research
To answer the research question, the first step was to investigate the intra-individual changes in adolescent depression and the intra-individual changes in different domains of social skills from early to middle adolescence. Based on existing research, we hypothesized that there would be an increase in depression as participants progressed from early to middle adolescence. However, there are inconsistent views on the changes of social skills during adolescence. Some researchers believed that social skills increased in adolescence with the maturation of cognitive and emotional capabilities (e.g., Kilford et al., 2016), whereas other researchers argued that the performance of social skills might decrease in adolescence because adolescents become more self-conscious and tended to achieve social dominance with more coercive strategies (e.g., Padilla-Walker & Christensen, 2011; Reijntjes et al., 2016; Yu et al., 2018). Moreover, some studies found that social skills are relatively stable across development (e.g., Bornstein et al., 2010; Crocetti et al., 2019). In spite of the inconclusiveness in the literature regarding the social skill development during adolescence, there are few studies examining how specific domains of social skills change from early to middle adolescence. Thus, no specific hypotheses were proposed regarding how cooperation, assertion, responsibility, and self-control would change across early to middle adolescence. After the growth trajectories of each construct were identified, we examined how the changes in cooperation, assertion, responsibility, and self-control would influence the changes in depression. Based on the discussed theoretical and empirical research on the link between social skills and depression, it was hypothesized that the changes in cooperation, assertion, responsibility, and self-control would negatively influence the change in depression.
2. Method
2.1 Participants and Procedures
Participants of the current study were drawn from the National Institute of Child Health and Human Development Study of Early Child Care and Youth Development (NICHD SECCYD). The NICHD SECCYD was a multisite, prospective, longitudinal study that began in 1991 with the recruitment of 8.986 mothers at 10 hospital sites across the United States. Factors such as location, availability, previous working relationships with site investigators, and patient population contributed to the selection of hospitals at each site. Enrollment in the NICHD SECCYD involved three steps: (1) a hospital screening of mother-newborn dyads within 48 hours after birth. Subjects were excluded from the sample if a) the family planned to move, b) the mother was not sufficiently conversant in English, c) the child was hospitalized for more than 7 days following birth or had obvious disabilities, d) the mother had a known or acknowledged substance abuse problem, or e) the mother was less than 18 years old. A total of 8.986 mother-newborn dyads were screened in the hospital. (2) A 2-week phone call to mothers found to be eligible at screening. Of the 8,986 eligible mothers, 5.416 (60%) agreed to be telephoned in 2 weeks. Of that group, 3.015 (56%) were selected using a conditional random sampling plan. Finally, (3) a 1-month interview with families that remained eligible after the 2-week phone call, agreed to the 1-month interview, and kept the interview appointment. Of the 3.015 families selected for participation, 1.526 (51%) agreed to participate and 1.364 (89%) actually participated in the initial data collection visit and gave signed consent when the child was 1 month old. Of the 1.364 families, 51.7% were boys, 19.6% were ethnic minority children, 10.2% mothers had not complete high school, and 21.4% families were classified as living in poverty. NICHD SECCYD data was collected from the study children, the study children’s families, after-school caregivers (if used), and teachers. Children were also assessed by research assistants at home, in child care (if used), in school, and in a laboratory playroom. Prior to the start of formal schooling, data were collected on an age-based chronological schedule. With the onset of formal schooling, data were collected on a year-in-school basis.
Four phases of data collection occurred subsequent to recruitment. During Phase I (1991-1994), children and their families were recruited when children were one month old and studied through 36 months. During Phase II (1995-1999), children and families were followed from 54 months old to 1st grade. During Phase III of the study (2000-2004), children and families were studied from 2nd grade to 6th grade. Phase IV (20052008) followed enrolled children and families from 7th grade to 9th grade. Data were collected from the study children, the study children’s families, after-school caregivers, and teachers. Prior to the start of formal schooling, data were collected on an age-based chronological schedule. With the onset of formal schooling, data were collected on a year-in-school basis. Details about all data collection procedures during Phase III, psychometric properties of the instruments, and descriptions of composites are documented in the studys Manuals of Operation and Instrument Documentation.
The current study focused on Phase III data with two time points (5th grade, and 6th grade) and Phase IV data with one time point (9th grade). For nearly all analyses presented below, the working sample comprised 1.061 of the 1.364 participants, which included participants with valid data for at least one of the core indicators used in the analyses from at least one time point of 5th grade, 6th grade, and 9th grade. Of the current sample, 50% were boys; 18.6% were ethnic minority children, 8.5% mothers had not complete high school, 8.2% families were classified as living in poverty.
2.2 Measures
2.2.1 Social Skills
Social skills were measured by mother-report Social Skills Rating System (SSRS; Gresham & Elliott, 1990). SSRS is a standardized assessment that documents the perceived frequency of target behaviors under four subscales: Cooperation (10 items), Assertion (10 items), Responsibility (10 items), and Self-Control (10 items). Cooperation includes behaviors such as helping household members and following rules. Assertion includes initiating behaviors, such as introducing oneself to others and joining group activities without being told. Self-Control includes appropriate responds in different situations, such as receiving criticisms well and politely refusing unreasonable requests. Responsibility includes behaviors that require children to communicate with adults and regard for property or work, such as asking permission before using others property and requesting permission before leaving house. Mothers rate the frequency of target behaviors within these four domains on a 3-point scale (0= never, 1 = sometimes, 2 = very often). The reliability and the validity (content, criterion, and construct) of the SSRS have been demonstrated as good (Gresham & Elliott, 1990). In the sample for the current study, alphas for SSRS from 5th grade to 9th grade ranged from .88 to .91.
2.2.2 Depression
Depression was measured by the Short Form Childrens Depression Inventory (CDI; Kovacs, 1992) in 5th grade, 6th grade, and 9th grade. The CDI has good testretest reliability, internal consistency, and construct validity (Sitarenios & Kovacs, 1999). The Short Form Childrens Depression Inventory comprised of 10 items assessing the degree of childrens sadness, low self-esteem, and dysphoric mood over the last two weeks. Children were asked to select the statement that best describes them within the past two weeks. An example item is “I do most things O.K.” (scored 0), “I do many things wrong” (scored 1), “I do everything wrong” (scored 2). In the sample for the current study, alpha for the Short Form Childrens Depression Inventory from 5th grade to 9th grade ranged from .73 to .81.
2.3 Statistical Analysis Plan
Missing data across measures and grades ranged from 3.9% (social skills in 5th grade) to 9.8% (depression in 6th grade). It occurred due to attrition and failure to complete all assessments. All missing data will be treated as ignorable (missing at random), and full information maximum likelihood (FIML) will be used to handle the missing data. Descriptive statistics also indicated that several of the indicators were skewed. To account for the issue of non-normality, maximum likelihood estimation with robust standard errors (MLR) will be used.
The data analyses are developed in-depth. First, latent growth analyses will be conducted to model the intra-individual changes in childrens social skills and depression, and to investigate the relationships between these changes. LGMs permit researchers to describe the within-individual development over time by modeling the intercept (initial status) and slope factors (rate of change) (Grimm et al., 2017). In the current study, the intercepts correspond to the initial level of childrens depression and four domains of social skills (cooperation, assertion, responsibility, and self-control) in 5th grade (Time 1). The slopes correspond to the rates of change in depression and the four domains of social skills over the period from 5th grade to 9th grade. The first aim of the current study was to determine the best fitting univariate latent growth models of each construct (depression and the four domains of social skills). The best-fitting univariate latent growth models describe the suitable form of the growth trajectory of each construct. Three unconditional models will be fit: (1) intercept only, (2) intercept and linear slope, (3) intercept and unspecified slope. With three waves of data, the quadratic factors will not be considered in the current research. The “intercept only” model can also be seen as “nogrowth” model, which indicates that no growth occurred from 5th grade to 9th grade. The “intercept and linear slope” model is specified as a linear pattern of intraindividual change over time. A linear trajectory model fixes the slope factor loadings corresponding to the time intervals. In the current study, the slope loadings would be fixed at 0, 1, 4 for 5th grade, 6th grade, and 9th grade. The “intercept and unspecified slope” model allows the shape of the trajectory determined by data. All latent growth models are assumed that errors for the same observed variables over time are equal and uncorrelated across time. Best-fitting univariate models will be carried forward into multivariate model-fitting.
The second aim of the current research was to examine the influences of the changes in social skills on the changes in depression from 5th grade to 9th grade. Multivariate latent growth models will be used to address the second research question. The advantage of multivariate latent growth models is that it can address how the growth trajectory of one construct influences the growth trajectory of another construct. In the current research, we aimed at investigating whether the initial status and the changes of the four domains of social skills would influence the initial status and the change of depression. The effects of four-domain social skills on depression will be revealed by the parameter estimates in the beta matrix. Specifically, to assess the influence of initial levels of social skills, the intercepts and slopes of depression will be regressed on the intercepts of cooperation, assertion, responsibility, and self-control; to examine the influence of rates of change of social skills, the slope of depression will be regressed on the slopes of cooperation, assertion, responsibility, and self-control. Gender (0=female, 1=male) and race (0=others, 1=White) will be included in the multivariate latent growth modelling as the time-invariant control variables. Figure 1 shows a representation of a basic multivariate latent growth model, taken one domain of social skills (cooperation) as an example.
Statistical analyses were conducted using Mplus software version 7 (Muthén & Muthén, 2012). For all models, three fit indices will be presented for the absolute fit: chi-square test of significance, the comparative Fit index (CFI), root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). A model is assumed to show acceptable fit when the CFI is larger than .90, RMSEA is smaller than. 08, and the SRMR is smaller than .08 (Browne & Cudeck, 1992). The chi-square test of significance is reported but not used as a measure of model fit, because it is highly sensitive to sample size. To compare the three unconditional univariate models, the relative fit of the models will be evaluated using the Bayesian Information Criterion (BIC; Raftery, 1995). The best fitting model has the lowest BIC value, but a BIC difference of 2 or less is considered to have equivalent fit (Burnham & Anderson, 2004).
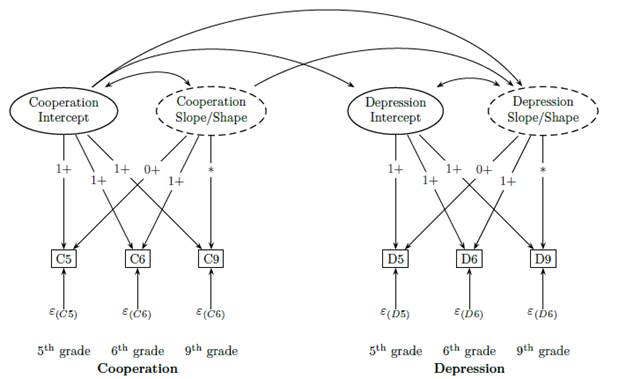
Note. Slope/Shape factors are not included in the intercept model. A parameter value with a plus sign indicates the parameter value is fixed. *indicates that the factor loadings may be fixed to 4 (linear trajectory model) or freely estimated (unspecified model).
Figure 1 Representation of a basic multivariate latent growth model
3. Results
3.1 Descriptive Statistics
Table 1 presents the descriptive statistics and bivariate correlations between the main variables across all assessments. As shown in the table, overall observed means showed rises in depression, responsibility, declines in cooperation and assertion, and remains relatively constant in self-control. Depression was negatively correlated with cooperation (mean r = .09), assertion (mean r =-.15), responsibility (mean r = .11), and self-control (mean r = .16) concurrently in each grade, such that students with higher social skills were less likely to experience depression. Four domains of social skills were positively correlated with each other (r = .37 to .69, p < .01) concurrently in each grade.
3.2 Univariate Latent Growth Models
Three unconditional models (intercept only; intercept and linear slope; intercept and unspecified slope) were fit for the univariate growth models of depression, cooperation, assertion, responsibility, and self-control, respectively. The intercept model provided a poor fit to the depression data, χ 2(6) = 99.10, p <.01, CFI=.34, TLI=.67, RMSEA=.12, SRMR=.17, indicating that some form of growth occurred from 5th grade to 9th grade. The linear slope model provided an acceptable model fit, χ 2(3) = 11.97, p <.01, CFI=.94, TLI=.94; RMSEA=.05, SRMR=.07. To identify the unspecified slope model, we fixed the Time 1 (5th grade) slope/shape to 0 and the Time 3 (9th grade) slope/shape factor loading to 10.5, based on the maximum likelihood estimate from the initial unspecified model. Time 2 (6th grade) slope/shape factor loading was freely estimated. The unspecified slope model also provided a reasonable model fit, χ 2(2) = 5.4, p = .07, CFI=.98, TLI=.97, RMSEA=.04, SRMR=.05. The BIC of unspecified model (12905.63) is smaller than the BIC of linear model (12915.32), suggesting that a curvilineargrowth trajectory is better than a linear growth trajectory to represent the intra-individual depression change from 5th grade to 9th grade. The slope/shape loadings are 0, 1.003, 10.5 for 5th grade, 6th grade, and 9th grade. The 6th grade loading (1.003) did not depart significantly from 0 (p = .09), indicating that the level of depression remained relatively constant from 5th grade to 6th grade. The intercept factor mean of depression revealed significant level of depression in 5th grade (µ = 1.30, p < .001), and the estimate of the slope factor was significantly positive (µ = .07, p < .001). The variance of intercept factor (σ 2 = 2.09, p < .001) and the variance of slope/shape (σ 2 = .04, p < .001) factor were significantly different from zero, showing that there were individual differences in depression at the initial status (5th grade) and at the rate of change from 5th grade to 9th grade. The factor covariance between intercept and slope/shape was significant (σ 2 = .06, p = .01), indicating that adolescents who had a lower depression in 5th grade increased faster in depression through 9th grade, which reflects the phenomenon of regression to the mean.
Table 1 Bivariate Correlations between the Main Variables across All Assessments
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
| 1.Depression5 | - | ||||||||||||||
| 2.Depression6 | .50** | - | |||||||||||||
| 3.Depression9 | .25** | .33** | - | ||||||||||||
| 4.Cooperation5 | -.08** | -.09** | -.03 | - | |||||||||||
| 5.Cooperation6 | -.08** | -.11** | -.01 | .69** | - | ||||||||||
| 6.Cooperation9 | -.06 | -.07* | -.09** | .53** | .54** | - | |||||||||
| 7.Assertion5 | -.13** | -.13** | -.09** | .37* | .27** | .19** | - | ||||||||
| 8.Assertion6 | -.14** | -.16** | -.13** | .29** | .34** | .21** | .68** | - | |||||||
| 9.Assertion9 | -.11** | -.18** | -.16* | .24** | .26** | .33** | .50** | .58** | - | ||||||
| 10.Responsibility5 | -.11** | -.10** | -.02 | .46** | .34** | .30** | .60** | .47** | .42** | - | |||||
| 11.Responsibility6 | -.09** | -.07* | -.04 | .37** | .49** | .34** | .48** | .60** | .42** | .67** | - | ||||
| 12.Responsibility9 | -.11** | -.15** | -.15** | .34** | .36** | .54** | .40** | .41** | .55** | .43** | .46** | ||||
| 13.Self-control5 | -.18** | -.13** | -.10** | .48** | .38** | .32** | .45** | .35** | .26** | .54** | .45** | .45** | - | ||
| 14.Self-control6 | -.15** | -.15** | -.08* | .42** | .52** | .37** | .36** | .44** | .27** | .43** | .59** | .48** | .74** | - | |
| 15.Self-control9 | -.13** | -.14** | -.14** | .31** | .33** | .49** | .25** | .28** | .37** | .31** | .36** | .69** | .59** | .63** | - |
| Mean | 1.95 | 2.15 | 2.64 | 1.23 | 1.20 | 1.18 | 1.70 | 1.68 | 1.50 | 1.51 | 1.52 | 1.73 | 1.39 | 1.39 | 1.40 |
| SD | 2.60 | 2.76 | 1.78 | .33 | .35 | .35 | .26 | .28 | .34 | .26 | .28 | .26 | .33 | .34 | .35 |
Note. All correlations are significant at p < .05 ∗ ∗ p < .01.
For the cooperation data, the intercept model provided apoor fit, χ 2(6) = 95.22, p <.01, CFI=.87, TLI=.93, RMSEA=.12, SRMR=.11, indicating that some form of growth occurred from 5th grade to 9th grade. The linear model also provided a poor fit, χ 2(3) = 26.55, p < .01, CFI=.96, TLI=.96, RMSEA=.09, SRMR=.09, showing that curvilinear growth occurred from 5th grade to 9th grade. The unspecified slope model (the slope loadings of are fixed at 0, 4, for 5th grade and 9th grade, but the slope factor loading of 6th grade is freely estimated) provided an acceptable model fit, χ 2(2) = 14.37, p < .01, CFI=.98, TLI=.97, RMSEA=.08, SRMR=.07.
The slope/shape loadings are 0, .05, 4 for 5th grade, 6th grade, and 9th grade. The 6th grade loading (.05) did not depart significantly from 0 (p = .87). The intercept factor mean of cooperation revealed significant level of depression in 5th grade (µ = 1.22, p < .001), and the estimate of the slope factor was significantly negative (µ = .09, p < .001), indicating that decrease in cooperation occurred from 6th grade to 9th grade. The variance of intercept factor (σ 2 = .77, p < .001) and the variance of slope/shape factor (σ 2 = .25, p < .001) were significantly different from zero, reflecting that there were individual differences in cooperation at the initial status (5th grade) and at the rate of change from 5th grade to 9th grade. The factor covariance between intercept and slope/shape was significant (σ 2 = .37, p < .001), indicating that adolescents who had a lower level of cooperation in 5th grade decreased slower through 9th grade.
For the assertion data, the intercept model provided a poor fit, χ 2(6) = 624.52, p < .01, CFI=.09, TLI=.54, RMSEA=.31, SRMR=.56, indicating that some form of growth occurred from 5th grade to 9th grade. The linear model provided an acceptable fit, χ 2(3) = 29.23, p < .01, CFI=.96, TLI=.96, RMSEA=.09, SRMR=.06.
The unspecified slope model (the slope loadings of are fixed at 0, 1, for 5th grade and 6th grade, and the slope factor loading of 9th grade is freely estimated) provided an acceptable model fit, χ 2(2) = 5.92, p = .05, CFI=.99, TLI=.99, RMSEA=.04, SRMR=.09. The BIC of un-specified model (14002.73) is smaller than the BIC of linear model (14024.69), suggesting that a curvilinear growth trajectory is better than a linear growth trajectory to represent the intra-individual assertion change from 5th grade to 9th grade. The slope/shape loadings are 0, 1, 8.31 for 5th grade, 6th grade, and 9th grade. The 9th grade loading (8.31) departed significantly from 0 (p < .001), showing that the level of assertion decreased substantially from 6th grade to 9th grade. The intercept factor of assertion revealed significant level at 5th grade (µ = 1.70, p < .001), and the estimate of the slope factor was significantly negative (µ = .24, p < .001), indicating that decreases in assertion occurred from 5th grade to 9th grade. The variance of intercept factor (σ 2 = .51, p < .001) and the variance of slope/shape factor (σ 2 = .07, p = .03) were significantly different from zero, revealing that there were individual differences in assertion at the initial status (5th grade) and at the rate of change from 5th grade to 9th grade. The factor covariance between intercept and slope/shape was nonsignificant (σ 2 = .03, p = .40).
For the responsibility data, the intercept model provided a poor fit, χ 2(6) = 668.94, p < .01, CFI<.001, TLI=.48, RMSEA=.32, SRMR=.45, indicating that some form of growth occurred from 5th grade to 9th grade. The linear model also provided a poor model fit, χ 2(3) = 78.24, p <.01, CFI=.88, TLI=.88, RMSEA=.15, SRMR=.21. To identify the unspecified slope model, we fixed the Time 1 (5th grade) slope/shape to 0 and the Time 3 (9th grade) slope/shape factor loading to 50, based on the maximum likelihood estimate from the initial unspecified model. Time 2 (6th grade) slope/shape factor loading was freely estimated. The unspecified slope model provided an acceptable model fit, χ 2(2) = 9.94, p = .007, CFI=.99, TLI=.98, RMSEA=.06, SRMR=.09, suggesting that a curvilinear growth trajectory is better than a linear growth trajectory to represent the intraindividual responsibility change from 5th grade to 9th grade. The slope/shape loadings are 0, .998, 50 for 5th grade, 6th grade, and 9th grade. The 6th grade loading (.998) did not depart significantly from 0 (p = .51). The intercept factor of responsibility revealed significant level at 5th grade (µ = 1.51, p < .001), and the estimate of the slope factor was significantly negative (µ = .04, p < .001), showing that increases in responsibility occurred from 5th grade to 9th grade. The variance of intercept factor (σ 2 = .49, p < .001) and the variance of slope/shape factor (σ 2 = .01, p < .001) were significantly different from zero, indicating that there were individual differences in assertion at the initial status (5th grade) and at the rate of change from 5th grade to 9th grade. The factor covariance between intercept and slope/shape was nonsignificant (σ 2 = .04, p < .01), revealing that adolescents who had a higher level of responsibility in 5th grade increased slower in responsibility through 9th grade.
For the self-control data, the intercept model provided an acceptable fit, χ 2(6) = 77.53, p < .01, CFI=.93, TLI=.97, RMSEA=.11, SRMR=.07. The linear model also provided a better model fit, χ 2(3) = 15.97, p < .01, CFI=.99, TLI=.99, RMSEA=.06, SRMR=.08. The un-specified slope model (the slope loadings of are fixed at 0, 1, for 5th grade and 6th grade, but the slope factor loading of 9th grade is freely estimated) provided an acceptable model fit, χ 2(2) = 9.82, p = .007, CFI=.99, TLI=.99, RMSEA=.06, SRMR=.06. The difference between the BIC of unspecified model (14601.35) and the BIC of linear model (14602.20) was less than 2. Thus, the linear model was accepted as the best-fitting model to represent the intra-individual self-control change from 5th grade to 9th grade. The intercept factor of assertion revealed significant level in 5th grade (µ = 1.39, p <.001), and the estimate of the slope factor was nonsignificant (µ = .03, p = .18), indicating that there was no change occurred from 5th grade to 9th grade. The variance of intercept factor (σ 2 = .85, p < .001) and the variance of slope/shape factor (σ 2 = .23, p < .001) were significantly different from zero, showing that there were individual differences in self-control at the initial status (5th grade) and at the rate of change from 5th grade to 9th grade. The factor covariance between intercept and slope/shape was nonsignificant (σ 2 = .38, p < .01), indicating that adolescents who had a higher level of self-control in 5th grade increased slower in self-control through 9th grade.
3.3 Multivariate Latent Growth Models
To investigate the effects of cooperation, assertion, responsibility, and self-control on the growth trajectory of depression, four multivariate latent growth models were conducted. The multivariate latent growth model of cooperation and depression had an acceptable model fit, χ 2(18) = 59.85, p < .01, CFI=.97, TLI=.95, RM-SEA=.05, SRMR=.06. The intercept of cooperation negatively predicted the intercept of depression (β =.17, p < .001), such that adolescents who had a higher level of cooperation were less depressive in the 5th grade. The influence of the intercept of cooperation on the slope of depression was nonsignificant (β = .02, p = .78), and the influence of the slope of cooperation on the slope of depression was significant (β = .19, p < .001). The result indicates that the level of cooperation in the 5th grade does not have a significant effect on the rate of change of depression from 5th grade to 9th grade, but adolescents who had a decrease in cooperation tended to experience a faster increase in depression over time.
The multivariate latent growth model of assertion and depression had an acceptable model fit, χ 2(18) = 81.48, p <.01, CFI=.95, TLI=.92, RMSEA=.06, SRMR=.07. The intercept of assertion negatively predicted the intercept of depression (β = .26, p < .001), such that adolescents who had a higher level of assertion were less depressive in the 5th grade. The influence of the intercept of assertion on the slope of depression was nonsignificant (β = .01, p = .82), and the influence of the slope of assertion on the slope of depression was significant (β = −.18, p < .001). The result indicates that the level of assertion in the 5th grade does not have a significant effect on the rate of change of depression from 5th grade to 9th grade, but adolescents who had a decrease in assertion tended to experience a faster increase in depression over time.
Table 2
| Model | df | χ2 | CFI | TLI | SRMR | RMSEA | BIC |
| Depression | |||||||
| 1. Intercept Model | 6 | 99.10 | .34 | .67 | .17 | .12 | 13136.21 |
| 2. Linear Model | 3 | 11.97 | .94 | .94 | .07 | .05 | 12915.2 |
| 3. Unspecified Model | 2 | 5.34 | .98 | .97 | .05 | .04 | 12905.63 |
| Cooperation | |||||||
| 1. Intercept Model | 6 | 95.22 | .87 | .93 | .11 | .12 | 15004.87 |
| 2. Linear Model | 3 | 26.55 | .96 | .96 | .09 | .09 | 14948.94 |
| 3. Unspecified Model | 2 | 14.37 | .98 | .97 | .07 | .08 | 14940.62 |
| Assertion | |||||||
| 1. Intercept Model | 6 | 624.52 | .09 | .54 | .56 | .31 | 14700.94 |
| 2. Linear Model | 3 | 29.23 | .96 | .96 | .06 | .09 | 14024.69 |
| 3. Unspecified Model | 2 | 5.92 | .99 | .99 | .09 | .04 | 14002.73 |
| Responsibility | |||||||
| 1. Intercept Model | 6 | 668.94 | .00 | .48 | .45 | .32 | 14376.77 |
| 2. Linear Model | 3 | 78.24 | .88 | .88 | .21 | .15 | 13642.05 |
| 3. Unspecified Model | 2 | 9.94 | .99 | .98 | .09 | .06 | 13575.41 |
| Self-Control | |||||||
| 1. Intercept Model | 6 | 77.53 | .93 | .97 | .07 | .11 | 14644.96 |
| 2. Linear Model | 3 | 15.97 | .99 | .99 | .08 | .06 | 14602.20 |
| 3. Unspecified Model | 2 | 9.82 | .99 | .99 | .06 | .06 | 14601.35 |
The multivariate latent growth model of responsibility and depression had an acceptable model fit, χ 2(18) = 102.75, p < .01, CFI=.92, TLI=.89, RMSEA=.07, SRMR =.08. The intercept of responsibility negatively predicted the intercept of depression (β = .20, p < .001), such that adolescents who had a higher level of responsibility were less depressive in the 5th grade. The influence of the intercept of responsibility on the slope of depression was significant (β = .15, p = .02), and the influence of the slope of responsibility on the slope of depression was also significant (β = .38, p < .001). The result indicates that adolescents who have more responsibility in the 5th grade and adolescents who had an increase in responsibility tended to experience a slower increase in depression over time.
The multivariate latent growth model of self-control and depression had an acceptable model fit, χ 2(18) = 62.72, p < .01, CFI=.97, TLI=.96, RMSEA=.05, SRMR =.06. The intercept of self-control negatively predicted the intercept of depression (β = .25, p < .001), such that adolescents who had a higher level of self-control were less depressive in the 5th grade. The influence of the intercept of self-control on the slope of depression was nonsignificant (β = −.01, p = .86), and the influence of the slope of self-control on the slope of depression was significant (β = .18, p < .001). The result indicates that the level of self-control in the 5th grade does not have a significant effect on the rate of change of depression from 5th grade to 9th grade, but adolescents who had an increase in self-control tended to experience a slower increase in depression over time.
4. Discussion
The findings of the current research showed that there was a curvilinear growth trajectory of depression from 5th grade to 9th grade. To specify, adolescent depression remained from 5th grade to 6th grade and increased significantly from 6th grade to 9th grade. This result supported the hypothesis that there was an increase in depression as participants progressed from early to middle adolescence. In terms of the growth trajectory of different domains of social skills, the present study found that different domains of social skills have different growth trajectories. From 5th grade to 9th grade, there were intra-individual decreases in cooperation and assertion, intra-individual increase in responsibility, and intra-individual stability in self-control. The decreases in cooperation and assertion can be explained by the theory of adolescent egocentrism (Elkind, 1978). According to the theory, adolescents possess an imaginary audience that is more attentive and critical than the case, believe the self is unique and special, and focus their thoughts and attention toward the self rather than outward. Thus, the decline in cooperation and assertion from early to middle adolescence might reflect adolescents increasing self-consciousness and egocentrism. Moreover, with the increasing academic demand and changing support networks in high school, adolescents experience more stress and competitiveness, which might result in decreases in cooperation and assertion. The increase in responsibility is consistent with cognitive development theories and moral development theories. Cognitive development theories suggested that with the development of formal operations, adolescents cognitively consider the potential consequences of a behavior and reflect on how a behavior can influence themselves and others (Gullota et al., 1999; Keating, 1980; Mergler & Patton, 2007). Moral development theories indicated that the developing cognitive sophistication allows adolescents to demonstrate more moral autonomy and deeper personalandsocialawareness (Fowler & Dell, 2004; Kohlberg, 1981). With cognitive and moral development, adolescents may have a better understanding of personal responsibility and will act according to it.
The hypothesis that the changes of cooperation, assertion, responsibility, and self-control would negatively influence the change of depression was supported by the results. That is, adolescents who had more increase in responsibility and self-control from 5th grade to 9th grade tended to experience a slower increase in depression; while adolescents who had more reduction in cooperation and assertion from 5th grade to 9th grade tended to experience a faster increase in depression. Moreover, among the different domains of social skills, only the level of responsibility in 5th grade had a significant effect on the change of depression from 5th grade to 9th grade. To specify, adolescents who behaved more responsible in 5th grade tended to experience a slower increase in depression over time. Compared with cooperation, assertion, and self-control, responsibility has been paid less attention in the research of adolescent depression. Even though, some clues can be found in the literature indirectly proving the protective role of responsibility for adolescent depression. Middle adolescence is a period of heightened vulnerability to risktaking behaviors and problematic behavior. Previous research has indicated that adolescent depression was associated with risk-taking and problematic behaviors such as norm-breaking behavior, substance use, and sexual activity (e.g., Brooks et al., 2002; Hallfors et al., 2004; Rector et al., 2003). Personal responsibility, which is a form of psychosocial mature, can protect adolescents from risk-taking behaviors (Monahan et al., 2009). In a word, responsibility in early adolescence may decrease adolescent depression by protecting adolescents from risk-taking and problematic behaviors in middle adolescence.
Findings of the current research had profound implications for practices in prevention science. As discussed above, adolescence is a period of heightened vulnerability to egocentrism and risk-taking behaviors, which may exacerbate adolescent depression. Thus, promoting adolescents social skills may be particularly salient for the prevention of adolescent depression. Existing interventions for adolescent depression are primarily based on Interpersonal Psychotherapy-Adolescent Skills Training (IPT-AST; Young & Mufson, 2003) and Skills for Academic and Social Success (SASS; Masia Warner et al., 2007) which emphasize in different social skills. For example, the research of La Greca et al. (2016) found that the intervention aiming at increasing adolescents communication strategies and interpersonal problem-solving skills was effective to reduce adolescent depression. Social skill training may also benefit for children with special needs to alleviate depression. For example, Schiltz et al. (2018) found that bolstering social skills among adolescents with autism spectrum disorder (ASD) positively influenced their mental health. Social skills can be facilitated by practice and exercise (Wilson, 2002). That is, the development of behavioral patterns can be shaped by the continued enactment. With repeatedly and successfully performing specific social skills, similar patterns would be carried out in the future. However, a meta-analytic review of Stice et al. (2009) found that relatively shorter prevention programs produced significantly larger intervention effects than did longer prevention programs. Stice et al. (2009) assumed that extremely long programs may not appeal to adolescents, which causes greater attrition and decreased intervention effects. Therefore, practitioners should consider the suitable intervention duration for the participants. Despite practicing social skills, researchers and practitioners should also, more deeply, focus on cultivating adolescents value orientation, underlying judgements, and character. For example, to facilitate adolescents cooperative and assertive behaviors, the ethic of care should be emphasized in community and school context. The ethic of care is characterized by a desire to maintain relationships, caring about and responding to others needs, and a responsibility not to cause harm (Gilligan, 1982). With a care orientation, adolescents would be more likely to make connections with others and to embrace cooperation for mutual benefit. Intervention programs emphasizing creating caring school communities, such as The Child Development Project, have been demonstrated as effective in improving childrens social attitudes, values, and skills (Battistich, 2008). In addition to cooperation and assertion, self-control and responsibility also protect adolescents from depression by decreasing their involvements in risk-taking and problematic behaviors (Monahan et al., 2009). Promoting the development of self-control and responsibility is a critical goal in many youth programs. According to a review of responsibility intervention programs (Wood et al., 2009), the consideration of the long-term consequences and the adherence to commitments in the demanding situations would make adolescents more likely to control their impulses and behave with responsibility. Thus, practitioners should not only clarify the social controls but also inspire young peoples active and willful commitment to the demands.
Despite the current studys contributions, its limitations warrant attention in future research. First, besides gender and race, social economic status, such as maternal education and family income, may also influence adolescents social skills and depression. Thus, future research should include indexes of social economic status as covariates for a better understanding of the link between social skills and depression. Another limitation concerns the measurement. It is known that one limitation of utilizing secondary data is that we have to settle for the original measurement. In the current research, only mother-report social skill measurement was available across the study time span. Mother-report method cannot provide a comprehensive picture of childrens behavioral patterns, because mothers assess the child within the context of home. Future research should combine mother-report methods with other assessment methods, such as teacher-report and peer-report methods. In addition, only three-point data (5th grade, 6th grade, and 9th grade) was available across 5th grade to 9th grade in the dataset; thereby making it limited to accurately discern the shape of developmental changes. For example, in this study, the result showed that there was an increase in depression from early adolescence to middle adolescence, but it is not clear whether this increase is continuous or discontinuous. Specifically, the trajectory may show a smooth and monotonic increase with age, proceeding at a steady pace, or show discontinuities such as abrupt, stage-like increase. In the future, the assessments of social skills and depression should be conducted with more time points to provide a more accurate portrayal of developmental pattern.

