










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkCES Psicología
On-line version ISSN 2011-3080
CES Psicol vol.8 no.1 Medellín Jan./June 2015
Falls of older people living in the community- A critical review
Las caídas de las personas mayores que viven en la comunidad: Una revisión crítica
Carmen De la Cuesta-Benjumea1, Brenda Roe2
1 Phd. Department of Health Psychology, Faculty of Health Sciences. University of Alicante. ccuesta@ua.es, España
2 Evidence-based Practice Research Centre Edge Hill University Ormskirk England and Personal Social Services Research Unit University of Manchester Manchester England. Brenda.roe@edgehill.ac.uk
Forma de citar: De la Cuesta, C., & Roe, B. (2015). Falls of older people living in the community- A critical review. Revista CES Psicología, 8(1), 21-36.
Abstract
Falls are the most prevalent and serious accident older people suffer in their homes and also, they are the main reason for their hospital admission. In a great part of the cases falls expose at risk elderly people's well-being and quality of life. A critical narrative literature review was undertaken to inform research in the area of falls in older people living in the community. Articles were retrieved from Medline and Scopus data bases from November 2011 to January 2013. Citation searching was also used as a complement by hand searching of relevant journals. Additionally, an alert mechanism was established in Scopus for a period of one year to identify relevant studies or literature. Reviewed studies have provided valuable evidence about falls in older people and potential prevention strategies. However, evidence from relatives, caregivers and significant others is conspicuously absent. Falls in the community and falls prevention happen in social and family contexts that must be empirically studied and reported.
Keywords: Caregivers, Carers, Critical Review, Elder Care, Falls, Family Care, Gerontology, Primary Health Care, Public Health.
Resumen
Las caídas son el accidente más serio y prevalente que los mayores sufren en sus domicilios y son la principal razón de ingreso hospitalario. Las caídas ponen en riesgo el bienestar y la calidad de vida de los mayores. Se llevó a cabo una revisión narrativa crítica de la bibliografía a fin de informar estudios de investigación en el área de las caídas de los mayores que viven en la comunidad. Se recuperaron estudios de las bases de datos Medline y Scopus de Noviembre 2012 a Enero 2013. Se usó también búsqueda de citaciones que se complementó con búsqueda manual en revistas relevantes. Se estableció un sistema de alertas en Scopus a lo largo de un año para identificar estudios relevantes o bibliografía. Los estudios revisados han proporcionado una evidencia valiosa sobre las caídas de las personas mayores y las estrategias potenciales de prevención. No obstante, evidencia proveniente de sus familiares, cuidadores y otros significativos esta notablemente ausente. Las caídas en la comunidad y su prevención suceden en contextos familiares y sociales que deben ser empíricamente estudiados y registrados.
Palabras claves: Cuidadores, Revisión Crítica, Caídas, Cuidado Familiar, Gerontología, Atención Primaria, Salud Pública.
Introduction
Nowadays in Europe, falls are considered the most prevalent and serious home accident among elderly people, they are the main reason for their hospital admissions (European Innovation Partnership on Active and Healthy Ageing [EIP], 2012). Among Latin American and Caribbean countries the prevalence of falls in older people has a substantial variation. It ranged from 21.6% in Bridgetown, Barbados, to 34.0% in Santiago, Chile (Reyes-Ortiz, Al Snih & Markides, 2005). Falls are commonly defined as "inadvertently coming to rest on the ground floor or other lower level, excluding intentional change in position to rest in furniture, wall or other objects" (WHO, 2007, p.1). Falls are a threat to active ageing (World Health Organization [WHO], 2007) and put at risk older people's well-being and quality of life. Falls and falls related injuries are expected to increase unless action is taken (Todd & Skelton, 2004; WHO, 2007).
From the World Health Organization to the European Parliament documents, policy statements and research programmes have been issued and initiated (Comunicación de la Comisión Europea [COM], 2012; EIP, 2012; WHO, 2007; Salud, Bienestar y Envejecimiento [SABE], 2005). Successful interventions for falls prevention have been identified from systematic reviews and guidelines of good practice developed (Cameron et al., 2012; Gillespie et al., 2012; Registered Nurses' Association of Ontario [RANO], 2005). Approximately one in three 65 year-old individuals and over who live in the community, fall each year (Gillespie et al., 2012). If we consider that between 75% and 89% of these falls are not injurious and are not reported to health care professionals (Roe et al., 2009; Todd & Skelton, 2004), being the case that these falls in the community are more frequent than realised or reported.
Falls prevention is one of the activities of the Europe 2020 research strategy (COM, 2012) that has motivated the establishment of a specific European plan that aims to validate operational programmes for early risk identification and prevention of falls in at least 10 European countries by 2015 (EIP, 2012).
According to the 2000 Round of Population and Housing Censuses, in Europe people at the age of 65 and above live mostly in family households, and the most common feature is to live with their spouse or partner (Carrascosa & Sancho Castiello, 2012). However there are differences across Europe. For instance, in Denmark nearly 50% of 65 year-old people and over live on their own, while in Spain, Italy and Greece older adults comprise less than 20% (Carrascosa & Sancho Castiello, 2012). While the general figures indicate that 6.2% of older people live in households of five or more members of the same family, in Spain and Greece this figure goes up to 10% (Carrascosa & Sancho Castiello, 2012). In Southern Europe, older people living alone is least frequent. This is also the case of Latin America and the Caribbean where older adults living alone is not as common as it is in North America and Western Europe (Pelaez et al., 2005). Even so, living alone does not mean that older people are alone; in community neighbours, they care for each other and provide support to each other (Roe et al., 2009). Before and after a fall, older people relied on their informal networks (Roe et al., 2009). The role that communities can have in supporting and empowering frail elders and their caregivers have been recently acknowledged (Alzheimer's Society, 2013).
It has been estimated that informal care across Europe is five times more than formal services (Glendinnig, 2010). Southern Europe has a family welfare system to respond to the dependency needs of their older people population (Oudijk et al., 2011), this is labelled as a Mediterranean model of dependency protection. Its main characteristic is the practical absence of a systematic development of public services for dependent people and the greater role played by informal care with class and gender differences (Rogero Garcia, 2010). This is clearly evidenced in a recent comparative study of caregiving in national databases from Spain, England and USA (Sole-Auro & Crimmins 2014). In this model it is assumed that families should provide the majority of long term care with a minimum support (Glendinning, 2010) and this most likely includes falls prevention activities and care for those who have fallen. In Latin America and the Caribbean this is likely to be the case where strong familial relations are providing a safety net for older persons (Pelaez et al., 2005). This region is aging "prematurely" as the speed of aging is estimated to be at least twice as high as it was in other parts of the world (Pelaez et al. 2005). This aging process will take place "in the midst of weak economic performance, tense intergenerational relations, fragile institutional contexts, and restricted access to health care services" (Palloni et al., 2007, p. 255). Family support and involvement in the care of their elders will take on even more relevance here, putting high and improper pressure on families to care for their dependents.
Since the early 1970s the literature has paid an increasing attention to the contribution of relatives and significant others to the well-being of older people (Twigg, 1992; Twigg & Atkin, 1994; Nolan et al., 2001). Much has been advanced in terms of policy and research on carers and caregiving since then. Countries, like those in the United Kingdom, have national carers'strategies and include caregivers in their health care system and research (e.g. Department of Health [DH], 1999, 2008; Nolan et al., 2007; Roe et al., 2011/2012). Caregivers provide an important source of community support for dependent people and their presence in hospitals are also of key importance (Quero Rufián, 2007). Their numbers and contribution to the well-being of dependent people are steadily increasing worldwide.
This article presents findings from a critical narrative review of older peoples'falls in the community, that has included quantitative and qualitative studies, meta-synthesis and policy documents. The review detected a gap in the literature relating to the social context of falls, which is the focus of this paper. It highlights the need to include family and caregivers' experiences of falls in older people and alert health and social care professionals to their needs and inform development of services and interventions. Falls do not happen in a social vacuum, they also have consequences not only for the older person that falls but also their families, caregivers and social networks.
Aim
To inform research in the area of falls in older people living in the community.
Objectives and MethodA literature critical narrative review was undertaken to identify evidence on falls and falls prevention, inform discussion and future research in the area of falls in older people living in their homes. Literature was searched in two phases from November 2011 to January 2013. First key words and electronic data bases were used to retrieve relevant articles in the area of falls of older people living in the community. Key words included "falls", "accidental falls", and "accidents at home" and age filters were used. Articles were retrieved from Medline and Scopus data bases. Language was.restricted to English, Spanish and Portuguese. Searches were not limited by year of publication. Secondly, citation searching of relevant articles cited in the papers retrieved from the first phase was complemented by hand searching of relevant journals using the same search terms. Citation searching and hand searching expanded the search to include falls prevention interventions and programmes not considered in the key words of the first phase of the search. This strategy enabled key research reports and documents to be located. In addition, a system alerts mechanism was established in Scopus for a period of one year from January 2012 to January 2013 with the term "accidental falls in the community" to identify past and future studies or literature that could also be considered. Studies to meet the aim of the review were also included.
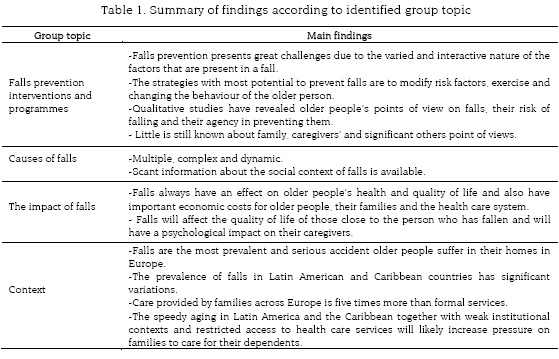
ResultsA total of 99 documents were retrieved, 14 were excluded as they did not address falls in older people in the community. In total 87 documents were included and reviewed. Included documents were reviewed and their fit for the purpose and aim of the review assessed. They were classified into four groups according to topic: a) cause of falls, b) impact of falls, c) fall prevention interventions and programme, and d) context. Documents in the four topic groups were critically read and coded according to its content by the first author. Draft narratives were developed as analytical memos (Strauss 1987) to synthesize findings on each group and to inform discussion. Drafts were reviewed by authors and consensus was reached. The review was a continuous process, and as it evolved a gap in the literature was noted highlighted by a general absence of reference to social networks in falls' events. Final analytical discussion memos were produced and the retrieved documents checked to validate this finding. The discussion memos were critically reviewed and synthesised to inform the narrative findings presented. See table 1 for a summary of main findings according to identified group topic.
Review findings
The focus of most documents was on falls prevention, epidemiological and clinical approaches to falls, with qualitative studies addressing subjective experiences in these events. However, reference to social networks in falls in the community was notably absent. Policy, research and theoretical papers focussed on practice; the main thrust of documents was on preventing falls occurring with little involvement from family and caregivers. The narrative findings are presented according to the four main identified themes: causes of falls, impact of falls and falls prevention and social context, with specific reference to qualitative research.
Causes of fallsThe causes of falls in older people have been extensively reported with an epidemiological risk approach. Causes are acknowledged to be very complex and dynamic (Todd & Skelton, 2004). Falls tend to recur within a year and the increase in the number of factors increases the risk of falling (Todd & Skelton, 2004; WHO, 2007). However, when describing the causes of falls, the terminology of infectious diseases is borrowed, using terms such as "exposure to risk" and they are generally studied as isolated events with no connection between them, although their cumulative effect on older persons' health is recognised (Vellas et al., 1997). This epidemiological approach leaves little room to consider the social and interactional aspects that are present in falls; when considering causes, falls tend to be presented in the literature similar to a disease.
The number of intrinsic factors presented in a fall identified in research studies is striking. These factors are related to the individual person (Todd & Skelton, 2004; WHO, 2007). Since early studies to the more recent ones the relevance of the environment has been acknowledged (Hornbrook et al., 1991; WHO 2007); however, the emphasis is on the physical. In the classifications of risk factors the social environment has been overlooked and its role unacknowledged and there is evidence of its importance. For instance, a study illustrated that in order to maintain a positive image in front of others as well as to keep their expectations high, older people can go beyond their abilities so they will be regarded as active and engaged; not doing it could mean being labelled as not "trying enough" with the negative consequences that this would imply (Minichiello et al., 2000). Relatives and significant others influence older people's decision making concerning the perception of the control over the risks that they have and this influence can be a facilitator as well as a barrier to prevention and risk management (Clemson et al., 1999).
In some local contexts, many falls happen in the presence of relatives, significant others and caregivers (Choi et al., 2011) and they might be a contributing cause of a fall as participants in a study pointed out (Dollar et al., 2012). A relationship between caregiver burden and dependent older persons'falls has been identified (Kuzuya et al., 2006; Maggio et al., 2010). But relatives and caregivers who live with the person who had a fall, are also reliable witness, and will have views on the causes and processes of falls. In order to better inform our understanding of falls, more research is needed into the social aspects of falls (Roe et al., 2008), this includes those close to the person who has fallen.
Scant information about the social context of falls is available. As currently reported they appear not to be socially produced, as symbolic interactionists might argue, but seem more a malady that happens due to. certain factors. The literature in this area does not acknowledge that people are always located in contexts where issues of structure, power agency and control will influence and change environments and patterns (Savin-Baden & Major, 2013). It is generally not recognized that people are suspended in a 'web of relations'as Clifford Geertz (1994) superbly stated. Consequently the epidemiological approach could blame the victim and they become the sole focus of the intervention.
Impact of fallsFalls are considered a public health issue (Ruchinskas, 2003; WHO, 2007; Bleijlevens et al., 2008) not only because of their prevalence but more importantly, because of the wider social and economic impacts they have. Studies show that among those who had a fall, 20% to 30% suffer injuries that will limit their mobility and consequently their independence (Todd & Skelton, 2004). Falls cause 40% of the deaths produced by injuries and this percentage increases with age being the highest among the oldest (WHO, 2007). In addition to the physical injuries, falls can produce a syndrome that includes dependence, confusion, immobility and depression that, in turn, lead to a restriction of the older people's activities of everyday life (WHO, 2007). Fear of falling is a common result of a fall and a threat to an older person's quality of life; it can result in isolation and dependence (Grossman & Stewart, 2003; Horton, 2008; Roe et al., 2008). Having a fall conveys the stigma of being perceived as incompetent and unable to live independently (Weeks & Roberto, 2002). Falls always have an effect on older people's health and also have important economic costs for older people, their families and the health care system (WHO, 2007; Todd & Skelton, 2004). It is expected that these costs will not be reduced but continue to increase, incurring higher costs in the health care services around Europe (Todd & Skelton, 2004).
Although it is acknowledged that falls can be a cause of anxiety for the family (Liddle & Gilleard, 1995), little is said about the impact that falls have on those who are close to affected elderly. We do not know whether the fear of a fall will extend to relatives and caregivers with negative consequences for the wellbeing of the dependent person.
Falls will affect the quality of life of those people close to the person who has fallen and will have a psychological impact on their caregivers. In some Latin countries it is said "Se me cayó"‡, implying a responsibility on the caregiver. Some evidence indicates that family and /or caregivers experience great anxiety caused by the fall of those they care for (Liddle & Gilleard, 1995) and associated with caregivers'emotional tension and their quality of life (Roth et al., 2009). However, not much more is known about the impact that falls have on caregivers'health and lives. From everyday experiences, we know about the devastating effects that a fall of an older parent can have on the lives of those who are close to them, as well as and the lasting effects of the fall. When reviewing the research evidence little is available on the consequence of relatives'falls from the perspectives of other family members or caregivers. This presents practitioners with little means to assess caregivers'needs and to support them..
Falls prevention: programmes and strategiesDeterring falls in old age is one of the health priorities in Europe. To meet this purpose policy documents have been issued (COM, 2012; EIP, 2012), models proposed (WHO, 2007), and much research is being conducted (Cameron et al., 2012; Gillespie et al., 2012). There is no question, preventing falls contributes to older peoples'quality of life, reduces much suffering and economic costs to the older person, the family and the health care system. The WHO Falls Prevention Model for reducing falls and fall-related injuries among older persons has a great significance for its comprehensiveness. This comprehensive framework was designed to identify policies, practices and procedures that will raise awareness of the importance of falls prevention, improve the assessment of risk factors of falls and promote the implementation of culturally-appropriated evidence based interventions (WHO 2007). The wider community where the older person lives is considered for the success of interventions and the importance of family and peers support in the uptake and adherence to preventive measures is acknowledged in this model (WHO, 2007). The older person's family is also included in awareness raising and information campaigns. Here falls are not considered homogenous, isolated and out of context events. Preventive strategies are to be tailored to the older person and contextualized, social groups and health care professionals are involved in this model and the process character of falls is acknowledged.
Although the rate of falls can be reduced with specific interventions (Registered Nurses'Association of Ontario [RANO], 2005; Cameron et al., 2012; Gillespie et al., 2012), falls prevention presents multiples challenges due to the varied factors that intervene and interact. Effective interventions see falls as the result of a series of risk factors and not as the result of random accidents (Lampiasi & Jacobs, 2010). For this reason, it is advised that interventions must be multiple, multi factorial (Todd & Skelton, 2004; Cameron et al., 2012; Gillespie et al., 2012) and delivered by a multi professional team (WHO, 2007). It also is suggested that older people, their significant others and health professionals engage in a collaborative process to assess the risks of falling (RANO, 2005; Lampiasi & Jacobs, 2010). However, caregivers'contribution in this matter is not documented in the reviewed literature. Thus health professionals are left to their own devices to figure out this collaboration and to find out caregivers'strengths, resources or needs. The strategies with the most potential to prevent falls identified in research studies are to modify risk factors and changing the behaviour of the older person living in the community. (Todd & Skelton, 2004). Group and home-based exercise programmes reduce falls effectively and exercise programmes appear also to reduce fractures (Gillespie et al., 2012). Attention to environmental factors are considered to be a priority since the early days, as they are associated with falls that produce injuries, fractures and dependence (Hornbrook et al., 1991). Additionally, research has pointed to the need to develop strategies to make older people's homes safer places (Lan et al., 2009). Interventions to improve home safety seem to be effective (Gillespie et al., 2012).
Research in falls prevention: The context and contribution of qualitative studies
Research studies on falls prevention programmes and activities have produced different levels of evidence synthesized in systematic reviews and assembled in best practice guidelines (Todd & Skelton, 2004; RANO, 2005; Gillespie et al., 2012). Nevertheless, older people's acceptance of preventive measures and participation in preventive programmes is low (McInnes et al., 2011) and may well reflect that local contexts, equity of access to services has not been considered. The lack of recruitment of older people in general to randomised controlled trials has been reported and is the focus of a European study (Prognostic Evaluation of Diagnostic [PREDICT]) (Crome et al., 2011). A recent study with older people living in the community in the Netherlands, found that the majority of participants showed no interest in participating in programmes for managing concerns about falls (Dorresteijn et al., 2012). It seems that that while falls might be an issue of concern for older people, established programmes fail to attract their attention.
Qualitative studies have explored their opinion about these programmes, uncovering the meaning they attach to the risk of falling, the difficulties they have in implementing the suggested actions and their motivation to participate in these programmes. It has been found that in accepting preventive measures, there are implicit issues related to older people's identity, biography and sense of independence (Yardley et al., 2006; Bunn et al., 2008; McInnes et al., 2011).
A qualitative study undertaken in six European countries found that the motivation to participate in falls prevention programmes included obtaining a wide range of benefits and not just the reduction of the risk of falling (Yardley et al., 2006). The support from their family and friends and the personal invitation of health professionals also helped their participation in these programmes (Yardley et al., 2006). Based on findings from different qualitative studies it is recommended that health professionals design flexible programmes to accommodate to the older people's different interests and needs, consult with the old person the feasibility of the changes proposed and promote the social interest of falls prevention programmes (McInnes & Askie, 2004). There is no mention of how those close to the older person might contribute to these programmes.
While qualitative studies have revealed older people's points of view on falls, their risk of falling and their agency in preventing them (Weeks & Roberto, 2002; Bunn et al., 2008; Roe et al., 2008; 2009; McInnes et al., 2011), little is known about family, caregivers'and significant others'points of view. Specifically, it is unknown the meaning they attach to the risk of falling, the strategies they use to prevent falls and how they manage these risks. The consequences of falls from the spouse, partner's or children's perspectives have received scant attention. In addition, the potential role that family and friends have in supporting preventive programmes has been overlooked.
In general terms, most of the literature on falls prevention is focussed on the individual older person. Much effort goes to develop and test intervention strategies (Cameron et al., 2012; Gillespie et al., 2012), to develop risk assessment tools (Aranda-Gallardo et al., 2013) and to engage patients in falls prevention programmes (for example, Yardley et al., 2006; Dorresteijn et al., 2012) but little is said about older people's relatives, caregivers or people close to them or the local context, availability and equity of falls services. Currently it is clearly acknowledged that interventions to prevent falls are very complex and implies more than accomplishing a set of activities or following a set of instructions. Our knowledge in this area is becoming sophisticated, the epidemiological approach is now enriched by additional approaches, namely qualitative, that are adding context to the effectiveness of interventions. The guiding principle of these approaches is to maintain and optimise older people's quality of life and preventive plans must also consider, support and respect older people taking risks, their autonomy and self-determination (RANO, 2005; Roe et al., 2008, 2009). Hence, it is very conspicuous the absence of those close to the older person, such as caregivers with whom a majority of older people in Southern Europe, Spain in particular, live with and their potential role in falls prevention initiatives and programmes.
The relationship between older people living with relatives and safer homes (Lan et al., 2009) highlights the importance of family support in preventing falls. The support from family, friends and health professionals has an influence in older people taking up fall preventive activities (Yardley et al., 2006). Informal support networks such as family, friends and neighbours are as important as formal care for those at risk of falling and for those who have fallen (Roe et al., 2009). In spite of this evidence, it is noticeable the marginal role that the family and caregivers have in the falls prevention research. Their scant presence in intervention programmes is conspicuous. In a recent systematic review on falls prevention interventions, the participation of the family and caregivers were not considered in any intervention (Cameron et al., 2012; Gillespie et al., 2012). This overlooks the fact that the family and caregivers make changes to the environment, give support to older people who have fallen and promote their confidence (Horton & Arber, 2004; Roe et al., 2009). The need to move beyond individualistic views of autonomy to a focus on interdependency (Breitholtz et al., 2013) is thus highlighted.
Current models for falls prevention include the family and caregivers in the stages of raising awareness of the importance of its prevention and treatment and in the stage of intervention (WHO, 2007; Choi et al., 2011). Guidelines state in their principles that significant others along with the health care team engage in assessment and interventions for falls'prevention (RANO, 2005). Nonetheless caregivers tend to be regarded in a passive role, as they are mostly considered for their needs for education in prevention and in risk reduction (WHO 2007) and not their actual contribution. Little has been documented about how they contribute on an everyday basis to preventing falls nor is it being taking into account the vital information they have for risk assessment and the adjustment of intervention programmes to their relatives'context and situations. As is customary, family caregivers'knowledge and skills tend to pass unnoticed in much of the literature. The WHO prevention model for falls reduction (2007) denotes a turn to the prevalent approach in the literature. This approach indeed opens up new avenues for research and intervention studies. Also, the European Action Group on falls prevention is currently including them in their initiatives (EIP, 2012). This shows a way forward. Evidence in this area will strengthen these models and practice guidelines.
Much research evidence has been produced in "a process that systematically excludes” evidence from practices and contexts (Leeman & Sandelowski, 2012; p. 171). Global evidence as gathered in systematic reviews is required for policy making, but has to also be interpreted in context with local evidence (Lewin et al., 2009). Local evidence is not only bound to countries and regions but also refers to social contexts, views and experiences of stakeholders such as relatives and caregivers. The ways in which local evidence can be useful are many; it can serve to contextualize interventions from global reviews, to inform judgements about values and preferences, to assess the availability of resources and to identify barriers (Lewin et al., 2009). Thus in discussing their importance in falls prevention attention is drawn to their importance for falls prevention services and policy making in general.
Strengths and LimitationsThis critical narrative review has included quantitative and qualitative evidence as well a range of different publications; policy, theoretical and research papers. Sustaining a search strategy over a year ensured locating up to date literature. Our review is based on the search strategy; this might have limited the scope; however, we identified a gap in the literature that has identified the need to address the perspectives of those family and caregivers who witness falls or who manage and support relatives after a fall event.
ConclusionEpidemiological and clinical studies have taken an increasing interest in falls, in older people, in particular and have provided valuable information about their causes and potential prevention. Qualitative studies are adding valuable information about meanings, perceptions, processes and experiences of those who fall that are contributing to a better understanding of this phenomenon and to the implementation of preventive measures. However, evidence from relatives, caregivers and significant others is conspicuously absent. The literature is conveying an image of older people falling alone and isolated, the fall happening in a sort of social vacuum. However, there are witnesses to these falls and there are caregivers who strive to prevent them. This might well be a reflection of the over reliance on the "organismic ageing processes" in epidemiology and policy domains that excludes social contexts (Kelley-Moore, 2010 p.107).
Relatives and significant others who assist older people in their homes and who have had a fall, have unique information about the circumstances in which they occur and know very well the effects that they have on their lives too. Their opinion about the causes of the fall, experience of managing them and the emotional consequences of falls on the older person and themselves who may have witnessed them must not pass unnoticed in the literature. Those who support and assist older people are key actors in making adjustments in the home environment and in promoting old people's safe behaviours. Preventive programmes must acknowledge and promote their engagement in such programmes. This is especially relevant if we consider that the environmental factors are also strongly associated, with falls in older people (Hornbook et al. 1991). The epidemiological approach to falls prevention with its reductionism and individualist focus is leaving blinded areas of interest for community health practitioners.
Falls and falls prevention happen in social and family contexts that must be empirically studied and reported. It is hoped that this review has highlighted the gaps, has raised awareness and ultimately, motivated to the development of studies that will further our understanding of older people who live in the community experiencing falls and the perspectives of their families and caregivers.).
Implications for practiceCaregivers incorporate risk management strategies into daily life (Kita & Ito, 2013) and contribute to the well-being of frail and dependent persons. Their contributions and views on the area of falls prevention need to be documented and their needs be considered. This knowledge will enable health care professionals to support caregivers in their efforts of risk.management and enhance their abilities in falls prevention and care. Improving family's coping strategies is a powerful type of intervention (Nolan et al., 2003) that community or primary health care practitioners are in a privileged position to use.
An epidemiological approach focused on the individual has tended to dominate research, falls seems to be in the realm of biomedicine, this is well illustrated in a research study that advises a referral to a "falls clinic" and to "specialist falls services" following a fall (Close et al., 2012, p. 746). Research from the social sciences and community health care perspectives is much needed in this area, to not only contribute to current falls prevention programmes; but provide health care professionals with evidence that is contextualized and close to older people's experiences, identify barriers to the implementation of guidelines and programmes and highlight gender differences. It must not be overlooked that falls affects the lives of those close to the person who has fallen; studies need to capture these broader impacts and consequences so interventions could be developed to assist them. This is an area that health and social care practitioners could contribute.
Qualitative research is helpful in bringing the voices of people to the fore and may consequently have greater impact in the development of policies (Scharf, 2010). In the area of ageing, research about the experiences of particular groups will contribute to the development of social policies (Scharf, 2010) as well as health care policies and practices. In particular, research studies that include relatives, caregivers and significant others will contribute to the development of effective interventions and the development of falls assessment instruments. It will also shed light onto the situations and events that follow a fall, that is, on the impact that it has on the older person's life and how they are coping with its consequences. These are issues that health and social care professionals need to consider in order to develop effective interventions (Weeks & Roberto, 2002).
Referencias
Alzheimer's Society. (2013). Building dementia-friendly communities: A priority for everyone. UK: Alzheimer's Society. [ Links ]
Aranda-Gallardo, M., Morales Asencio, J. M., Canca-Sanchez, J. C., Mora-Banderas, A. M. & Moya Suarez, A. B. (2013). Instruments for assessing the risk of falls in acute hospitalized patients: a systematic review protocol. Journal of Advanced Nursing, 69(1), 185-193. [ Links ]
Breitholtz, A., Snellman, I. & Fagerberg, I. (2013). Older people's dependence on caregivers'help in their own homes and their lived experience of their opportunity to make independent decisions. International Journal of Older People Nursing. 8, 139-148. doi: 10.1111/j.1748-3743.2012.00338.x [ Links ]
Bleijlevens, M. H. C., Hendriks, M. R. C., van Haastregt, J. C. M., van Rossum, E., Kempen, G. I. J. M., Diederiks, J. P. M., Crebolder, H. F. J. M. & van Eijk, T. H. M. (2008). Process factors explaining the ineffectiveness of a multidisciplinary fall prevention programme: A process evaluation. BMC Public Health, 8, 332. Available in: http//www.biomedcentral.com/1471-2458/8/332. [ Links ]
Bunn, F., Dikinson, A., Barnett-Page, E., McInnes, E. & Horton, K. (2008). A systematic review of older people's perceptions of facilitators and barriers to participation in falls-prevention intervention. Ageing and Society, 28(4), 449-472. [ Links ]
Cameron, I. D., Gillespie, L. D., Robertson, M. C., Murray, G. R., Hill, K. D., Cumming, R. G.,& Kerse, N. (2012). Interventions for preventing falls in older people in care facilities and hospitals. Updated. Cochrane summaries. Published on line: December 12, 2012. Available in: http://summaries.cochrane.org/CD005465 [ Links ]
Carrascosa, L. L. & Sancho Castiello, M. T. (2012). Formas de convivencia, relaciones personales y la experiencia de envejecer. [Ways of living together, personal relationships and the experience of ageing] In: IMSERSO (Ed), Informe en 2010, las personas mayores España. [2010 Report; elders in Spain] (pp. 233-264). Madrid: IMSERSO. [ Links ]
Choi, Y. S., Lawlwe, E., Boenecke, B., Ponatoski, E. R. & Zimring, C. (2011). Developing a multi-system fall prevention model, incorporating the physical environment, the care process and technology: a sustematic review. Journal of Advanced Nursing, 67(12), 2501-2524. [ Links ]
Clemson, L., Cusick, A. & Fozzard, C. (1999). Managing risk and exerting control: dermining follow through with falls prevention. Disability and rehabilitation, 21(12), 531-541. [ Links ]
Close, J. C., Lord, S. R., Antonova, E., Martin, M., Lensberg, B., Taylor, M., Hallen, J. & Nelly, A. (2012). Older people presenting to the emergency department alter a fall: a population with substantial recurrent health care use. Emergency Medicine Journal, 29(9) 742-747. [ Links ]
COM, Comisión Europea. (2012). Comunicación de la Comisión al Parlamento Europeo y al Consejo- Plan Estratégico de Aplicación de la Cooperación de Innovación Europea sobre el Envejecimiento Activo y Saludable.[European Strategic Plan for the Aplication of Innovation and Cooperation in Active and Healthy Ageing] Available in: http://www.envejecimientoactivo2012.es/InterPresent1/groups/imserso/documents/binario/7293es12.pdf [ Links ]
Crome, P., Lally, F., Cherubini, A., Oristrell, .J, Beswick, A. D., Clarfield, A. M,, Hertogh, C., Lesaukaite, V., Prada, G. I., Szczerbinska, K., Topinkova, E., Sinclair-Cohen, J., Edbrooke, D. & Mills, G . (2011). Exclusion of people from clinical trials: Professional views from nine European countries participating in the PREDICT study. Drugs Aging, 28(8), 667-677. [ Links ]
Department of Health [DH]. (1999). Caring about cares: a national strategy for carers. London, Department of Health. [ Links ]
Department of Health [DH]. (2008). Carers at the heartof 21st centrury families and communities. London, Department of Health Available in: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/136492/carers_at_the_heart_of_21_century_families.pdf [ Links ]
Dollard, J., Barton, C., Newbury, J., & Turnbull, D. (2012). Falls in old age: a threat to identity. Journal of Clinical Nursing, 21(17-18), 2617-2625. [ Links ]
Dorresteijn, T. A. C., Rixt Zijlstra, G. A., van Eijs, Y. J. J., Vlaeyen, J. W. S. & Kempen G., I. J. M. (2012). Older people's preferences regarding programme formats for managing concerns about falls. Age and Ageing, 41(4), 474-481. [ Links ].
European Innovation Partnership on Active and Healthy Ageing (EIP). (2012). Action Plan 2 on Specific Action on innovation in support of Personalized health management, starting with a falls prevention initiative. Available in: http://ec.europa.eu/research/innovation-union/pdf/active-healthy-ageing/a2_action_plan.pdf#view=fit&pagemode=none [ Links ]
Geertz, C. (1994). Conocimiento Local. Ensayos sobre la interpretación de la culturas [Local Knowledge Furthrer essays in interpretative anthropology]. Basic Books, Haper Collins, USA. 1983]. Barcelona: Paidós. [ Links ]
Glendinning, C. (2010). Continuous and Long-term Care: European Perspectives. In: D. Dannfer & Philipson, C. (Eds.), The SAGE Handbook of Social Gerontology. (pp. 551-572.) Los Angeles:SAGE. [ Links ]
Gillespie, L. D., Robertson, M. C., Gillespie, W. J., Sherrington, C., Gates, S., Clemson, L. M. & Lamb, S. E. (2012). Interventions for preventing falls in older people living in the community. Cochrane summaries. Published on line: November 14, 2012. Available in: http://summaries.cochrane.org/CD007146. [ Links ]
Grossman, M. D., & Stewart, A. L. (2003). "You aren't going to get better by just sitting around: physical activity perceptions, motivations and barriers in adults 75 years of age or older. The American Journal of Geriatric Cardiology, 12(1), 33-37. [ Links ]
Hornbrook, M. C., Wingfield, D. J., Stevens, V. J., Hollis, J. F. & Greenlick, M. R. (1991). Falls among older persons: Antecedents and consequences. In: Weindruch, R., Hadley, E. C., Ory, M. G. & Badinelli, J. (Ed.) Reducing frailty and falls in older persons (pp. 106-125). Sprinfield, Illinois, USA: Charles C. Thomas Publisher. [ Links ]
Horton, K. (2008). Falls in older people: The place of telemonitoring in rehabilitation. Journal of Rehabilitation Research & Development, 45(8), 1183-1194. [ Links ]
Horton, K. & Arber, S. (2004). Gender and the negotiation between older people and their careers in the prevention of falls. Ageing and Society, 24(1), 75-94. [ Links ]
Instituto de Mayores y Servicios Sociales (IMSERSO). (2011). Envejecimiento Activo-Libro Blanco [Active ageing-White paper]. Madrid: Ministerio de Sanidad, Política Social e Igualdad. [ Links ]
Kelley-Moore, J. (2010). Disability and Ageing: The social construction of causalty. In: D. Dannfer & Philipson, C. (Eds.), The SAGE Handbook of Social Gerontology. (pp. 96-124) Los Angeles: SAGE. [ Links ]
Kita, M. & Ito, K. (2013). The caregiving process of the family unit caring for a frail older family member at home: a grounded theory study. International Journal of Older people Nursing 8, 149-158. doi: 10.1111/j.1748-3743.2012.00337.x. [ Links ]
Kuzuya, M., Masuda, Y., Hirakawa, Y., Iwata, M., Enoki, H., Hasegawa, J., Izawa, S. & Iguchi, A. (2006). Falls of the elderly are associated with burden of caregivers in the community Int J Geriatr Psychiatry, 21(8), 740-745. [ Links ]
Lan, T. Y., Wu, S. C., Chang, W. C. & Chen, C. Y. (2009). Home environmental problems and physical function in Taiwanese older adults. Archives of Gerontology and Geriatrics, 49 (3), 335-338. [ Links ].
Landy, D. C., Mintzer, M. J., Dearwater, S. R., Graygo, J. A. & Schulman, C. I. (2012). Fatal falls in an ethnically diverse urban community: The link between demographic factors and the circumstances surrounding fatal falls Southern Medical Journal, 105 (8), 405-410. [ Links ]
Lampiasi, N. & Jacobs, M. (2010). The role of the Physical and Occupational Therapies in Fall prevention and Management in the Home Settings. Care Management Journals, 11 (2), 122-127. [ Links ]
Leeman, J. & Sandelowski, M. (2012). Practice-Based Evidence and Qualitative Inquiry. Journal of Nursing Scholarship, 44 (2), 171-179. [ Links ]
Lewin, S., Oxman, A. D., Lavis, J. N., Fretheim, A., Garcia-Marti, S. & Munabi-Babigumira, S. (2009). SUPPORT Tools for evidence-informed Policymaking in health 11: Finding and using evidence about local conditions. Health Research Policy and Systems, 7 (Suppl 1) SII doi: 10.1186/1478-4505-7-SI-SII. [ Links ]
Liddle, J. & Gilleard, C. (1995). The emotional consequences of falls for older people and their families. Clin Rehabil, 9(2), 110-114. [ Links ]
Maggio, D., Ercolani, S., Andreani, S., Ruggiero, C., Mariani, E., Mafialasche, F., Palmari, N., & Mecocci, P. (2010) Emotional and Psychological distress of persons involved in the care of patients with Alzheimer disease predicts falls and fractures in their care recipients. Dementia and Geriatric Disorders, 30 (1), 33-38. [ Links ]
McInnes, E., Seers, K. & Tutton, L. (2011). Older people's views in relation to risk of falling and need for intervention: a meta-ethnography. Journal of Advanced Nursing, 67 (12), 2525-2536. [ Links ]
McInnes, E, & Askie, L. (2004). Evidence Review on Older People's Views and Experiences of Falls Prevention Strategies. Worldviews on Evidence-Based Nursing. 1 (1), 20-37. [ Links ]
Minichiello, V., Browne, J. & Kendig, H. (2000). Perceptions and consequences of ageism: views of older people. Ageing and Society, 20 (3), 253-278. [ Links ]
Nolan, M., Davies, S. & Grant, G. (2001). Working with older people and their families/ Key issues in policy and practice. Buckingham: Open University Press. [ Links ]
Nolan, M. R., Lundh, U., Grant, G. & Keady, J. (2003). Partnerships in Family Care: Understanding the Caregving Career. Maidenhead: Open University Press. [ Links ]
Nolan, M., Hanson, E. M., Grant, G. & Keady, J. (2007). User participation in health and social care research. Voices, values and evaluation. Maidenhead,:Open University Press. [ Links ]
Oudijk, D. Woittiez, I., & de Boer, A. (2011). More family responsability, more informal care? The effect of motivation on the giving of informal care by people aged over 50 in the Nehterlands compared to other European countries. Health Policy, 101(3), 228-235. [ Links ]
Palloni, A., McEniry, M., Wong, R. & Pelaez, M. (2007). Ageing in latin america and the caribbean:implications of past mortality. In: Department of Economic and Social Affairs-Population Division (Ed.) United nations expert group meeting on social and economic implications of changing population age structures (pp. 253-284)). United Nations, New York: Department of Economic and Social Affairs-Population Division. [ Links ]
Pelaez, M., Palloni, A., Albala, C., Alfonso, J. M., Ham-Chande, R., Hennis, A., Lebrao, M. L., Lesn-Diaz, E., Pantelides, E & Prats, O. (2005). SABE - Survey on Health, Well-Being, and Aging in Latin America and the Caribbean, 2000. Ann Arbor, MI: Inter-university Consortium for Political and Social Research. Available in: http://doi.org/10.3886/ICPSR03546.v1 [ Links ]
Quero-Rufián, A. (2007). Los cuidadores familiares en el hospital de Ruíz de Alda de Granada [Family caregivers in Ruiz de Alda Hospital Granada]. Unpublished Doctoral Thesis, Departamento de Antropología Social, Universidad de Granada. [ Links ]
Registered Nurses'Association of Ontario [RANO]. (2005). Prevention of fall and fall injuries in the older adult (Revised). Toronto, Canada: Registered Nurses'Association of Ontario. [ Links ]
S Reyes-Ortiz, C. A., Al Snih, S. & Markides, K. S. (2005). Falls among elderly persons in Latin America and the Caribbean and among elderly Mexican-Americans. Pan Am J Public Health, 17, 362-369. [ Links ]
Roe, B., Howell, F., Riniotis, K., Beech, R., Crome, P. & Ong, B. N. (2008). Older people's experience of falls: understanding, interpretation and autonomy. Journal of Advanced Nursing, 63 (3), 586-596. [ Links ]
Roe, B., Howell, F., Riniotis, K., Beech, R., Crome, P. & Ong, B. N. (2009). Older people and falls: health status, quality of life, lifestyle, care networks, prevention and views on service use following a recent fall. Journal of Clinical Nursing, 8, (16) 2261-2272. [ Links ]
Roe, B., Corbett, K., Byrne, M., McCourt, H., Chadwick, J., Jinks, A. (2011/12). Developments in mental health service provision: Views of service users and carers. Research, Policy & Planning. The Journal of the Social Services Research Group, 29(1), 3-19. [ Links ]
Roth, D. L., Perkins, M., Wadley, V., Temple, E, M. & Haley, W. (2009). Family caregiving and emotional strain: associations with quality of life in a large national sample of middle-aged and older adults. Quality of Life Research, 18 (6), 679-688. [ Links ]
Ruchinskas, R. (2003). Clinical prediction of falls in the elderly. Journal of Physical Medicine and Rehabilitation, 82 (4), 273-278. [ Links ]
Salud, Bienestar y Envejecimiento [SABE]. (2005). Survey on Health, Well-Being, and Aging in Latin America and the Caribbean, 2000. Ann Arbor, MI: Inter-university Consortium for Political and Social Research. Available in: http://doi.org/10.3886/ICPSR03546.v1. [ Links ]
Salkeld, G., Cameron, I. D., Cummings, R. G., Easter, S., Seymour, J., Kurrle, S. E., & Quine, S. (2000). Quality of life related to fear of falling and hip fracture in older women: a time trade off study. Bristih Medical Journal, 320 (7231), 341-346. [ Links ]
Savin-Baden, M. & Major, C. H. (2013) Qualitative Research. The essential guide to theory and practice. Abingdon, UK: Routledge. [ Links ]
Scharf, T. (2010). Social policies for ageing societies: Perspectives from Europe. In: D. Dannfer & Philipson, C. (Eds.), The SAGE Handbook of Social Gerontology (pp. 497-512). Los Angeles:SAGE. [ Links ]
Sole-Auro, A. & Crimmins, E.M. (2014). Who cares? A comparison of informal and formal care provision in Spain, England and the USA. Ageing & Society, 34, 495-517. [ Links ]
Todd, C. & Skelton, D. (2004). What are the main risk factors for falls among older people and what are the most effective interventions to prevent these falls? Copenhagen, WHO Regional Office for Europe (Health Evidence Network report) Available in: http://www.euro.who.int/document/E82552.pdf. [ Links ]
Twigg, J. (1992). Carers. Research & practice. London, HMSO. [ Links ]
Twigg, J. & Atkin, K. (1994). Carers perceived: Policy and practice in informal care. Buckingham: Open University Press. [ Links ]
Weeks, L. E. & Roberto, K. A. (2002). Empowering older women to address falls prevention. Quality in Ageing, 4 (3), 5-13. [ Links ]
World Health Organization. (WHO). (2007).Who Global report on falls prevention in older age .Geneva, Switzerland: WHO. [ Links ]
Vellas, B. J., Wayne, S. J., Romero, L. J., Baumgartner, R. N. & Garry, P. J. (1997) Fear of falling and restrictions of mobility in elderly fallers. Age and Ageing, 26 (3), 189-193. [ Links ]
Yardley, L., Bishop, F. L., Beyer, N., Hauer, K., Kempen, G. I. J. M., Piot-Ziegler, C., Todd, C., Cuttelod, T., Horna, M., Lanta, K. & Holt, R. (2006). Older people's views of falls-prevention interventions in six European countries. The Gerontologist, 46 (5), 650-660. [ Links ]
