











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Ultrasound is routinely used in the initial evaluation of trauma patients in the emergency department (ED), since early detection of life-threatening injuries is the most important factor in reducing mortality 1 Rozicky et al. 2 first described the use of ultrasound in the evaluation of trauma patients as extended focused assessment with sonography for trauma (E-FAST). In the context of trauma, the E-FAST protocol is used to identify free fluid and determine which patients should immediately undergo surgery. This is a non-invasive, operator-dependent, cost-effective and affordable procedure 3, which can be used by residents and specialists for the primary or secondary survey of trauma, in the absence of the availability of conventional imaging tools.
Point-of-care ultrasound (POCUS) and surgeon-performed ultrasound both build on the portability of the new ultrasound instruments to perform scans without involving patient transfers, delays in emergency department care or where necessary. Recently, revolutionary technologies such as portable POCUS probes 4, for example, the Butterfly IQ+ (Butterfly Network Technologies, Guilford, CT, USA), have generated great expectation. Main features consist of its portability, user-friendly interface and ease of configuration on everyday devices such as a cell phone or tablet, in addition to its relatively low cost compared to other devices with similar characteristics, without sacrificing fundamental properties such as image quality and maneuverability, making it an essential tool 5. Evidence in traumatology has shown that non-radiologist emergency physicians can perform E-FAST, with great precision, through specialized training 6. In regions with limited resources and barriers in the availability of specialized services 24 hours a day, such as the Colombian Caribbean region 7, alternatives should be sought to preserve efficiency in emergency care 8.
Currently, in this region, the performance of the use of E-FAST in the approach to trauma by general surgery residents in the emergency department, who during their training period attend the highest volume of trauma cases with risk or need for surgical care, has never been evaluated. Based on the above, the objective of this study was to determine the performance of the use of E-FAST in the assessment of trauma by second-year general surgery residents in a trauma referral center in the Colombian Caribbean region.
Methods
Retrospective observational study, which evaluated the diagnostic performance of E-FAST with Butterfly IQ+, in patients with thoracoabdominal trauma, who attended a reference center in the Colombian Caribbean, in the city of Barranquilla, between November 2021 and July 2022. This is a referral trauma center in the northern region of Colombia, which concentrates many injured patients. As inclusion criteria, it was defined that all patients over 18 years of age who were admitted to the emergency department presenting abdominal or thoracic injuries due to penetrating or blunt trauma, and who eventually underwent E-FAST with the Butterfly IQ+ ultrasound device, performed by 2 second-year general surgery residents with basic training in POCUS in the emergency department, were included. Pregnant women and patients with incomplete data in their clinical history were excluded.
Data were extracted from electronic medical records (EMR) and ultrasound (US) images stored in the individual Butterfly Network Cloud database. Sociodemographic data (age and sex), mechanism of trauma, E-FAST results, conventional imaging outcome, intraoperative findings, and final patient status were collected.
For portable ultrasound, a Butterfly IQ+ single probe whole body ultrasound system connected to an Apple iPhone 13 Pro Max (2021) or Apple iPad Mini (2021) via Lightning or USB-C cable, respectively, was used with the “Butterfly IQ” app. Patient data were recorded in the app and the preset “FAST protocol” was used in which each window to be evaluated was sequentially selected: subxiphoid pericardium, Morrison’s pouch, splenorenal recess, suprapubic window, and pulmonary window. The general surgery resident in charge performed the standard FAST evaluation between 1 and 5 minutes for each patient.
A true negative E-FAST was defined as an ultrasound with absence of free fluid and clinical surveillance or normal imaging performed by a radiologist using a console ultrasound machine. In contrast, a true positive E-FAST was defined as the sonographic identification of free fluid associated with positive findings on surgical examination, regardless of the location or volume of free fluid. A false negative E-FAST test was defined as the absence of free fluid on E-FAST, but with positive clinical or radiological findings suggestive of hemoperitoneum, hemopericardium, hemothorax or pneumothorax. A false positive E-FAST was defined as images suggestive of free fluid in the pleural, peritoneal or pericardial space in the absence of intraoperative findings.
Initially, the data were recorded in an Excel spreadsheet and then exported to SPSS software version 28.0, where the statistical analysis was performed. The normality of the quantitative variables was evaluated using the Shapiro-Wilk test. Data were presented as mean ± standard deviation (SD) for continuous variables. Qualitative variables were summarized as frequencies and percentages. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive test likelihood ratio (PLR), and negative test likelihood ratio (NLR) were calculated using the OpenEpi version 3.01 tool 9.
This study was approved by the institutional Ethics Committee and was conducted in accordance with the principles established in the Declaration of Helsinki.
Results
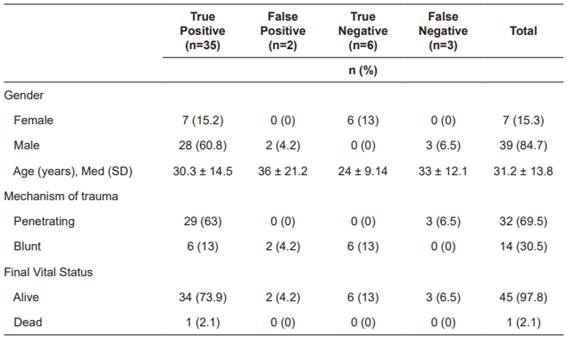
A total of 46 patients were included, with a mean age of 31.2 ± 13.8 years, 87.4% (n=39) were male. The main mechanism of trauma was penetrating (n=32; 69.5%), 93.4% (n=43) were taken to the operating room, mainly performing emergency laparotomy (n=24; 52.1%); 37 (80.4%) patients had positive E-FAST (Figure 1), 97% (n=35) were found to be true positive, based on intraoperative findings (only two were false positive). Of the nine (19.5%) patients with negative E-FAST, five underwent surgery, with three having positive findings of free cavity fluid (false negative) (Table 1). In comparison to the imaging and intraoperative findings, the sensitivity, specificity, PPV, NPV were found to be 92.1%, 75%, 94.6% and 66.6%, respectively. The PVR was 3.68, while the NPV was 0.10. The accuracy was found to be 89%.
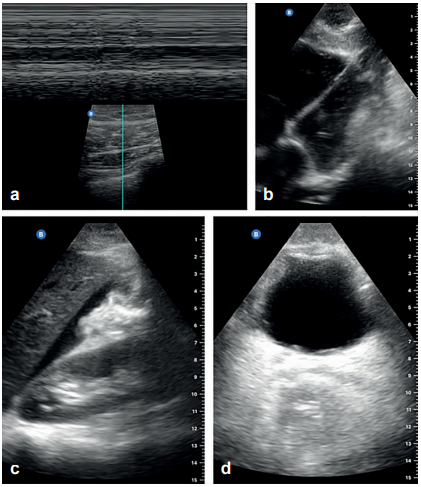
Figure 1. Findings with the use of E-FAST protocol using the portable ultrasound machine (Butterfly iQ+, Butterfly Network Technologies, USA). a. M-mode barcode sign, linear lung scan; b. Subxiphoid ultrasound showing four-chamber cardiac window; c. Morrison’s pouch ultrasound with positive identification of free fluid; d. Transverse suprapubic ultrasound showing four-chamber cardiac window. Subxiphoid ultrasound showing the four-chamber cardiac window.
Discussion
In scenarios with limited resources, the use of innovative diagnostic tools such as POCUS by the health team in training is somewhat controversial, due to the diagnostic performance and cost-utility and cost-effectiveness indicators, especially in the emergency setting 10-12. However, in the reality of some low- and middle-income countries, where it is precisely this team in training that is responsible for the immediate care and response of these services. Solutions should be evaluated and proposed to improve the performance of medical care with the least possible use of resources.
Trauma patients are a challenge for emergency physicians, especially those presenting with blunt trauma. Late diagnosis reduces good outcomes, survival rates and increases complications and mortality 13. The E-FAST protocol is a useful tool to diagnose and detect early thoracic and abdominal injuries during the primary examination 14. In high-income countries in the last two decades, general surgery residents and junior surgeons have been increasingly involved in the specialized training of this type of techniques, being mandatory to cover certain services, such as the emergency department. This has made it possible to increase performance and diagnostic accuracy, as well as patient flow in care centers 15.
E-FAST performed by a radiologist in all trauma patients is not feasible in our region due to lack of resources, especially because many of the hospitals in the Caribbean region of Colombia do not have a permanent staff radiologist. Therefore, trying to use and replicate portable techniques is an urgent necessity to promote decision-making in clinical practice 16. High quality evidence has reported significant performance with use by emergency physicians, obtaining sensitivity values of 74% (95% CI: 65 - 81) and specificity of 96% (95% CI: 94 - 98) 17. Sheng-Der Hsu et al. 18 carried out a study in 438 patients with thoracoabdominal trauma, who were evaluated by means of POCUS by general surgery residents, obtaining a sensitivity, specificity, NPV, PPV, and accuracy of 87%, 99%, 98%, 91%, and 97%, respectively. The PVR and NPV were 87% and 0.12, respectively 18. Therefore, the authors concluded that general surgery residents could be trained to perform E-FAST in the evaluation of trauma in the emergency department. It should be noted that systematic reviews to date have found significant heterogeneity in their results 17,19, since this performance varies substantially depending on the context, population, pathology and team operator. This could explain why in countries where the context of trauma and the population differs in terms of physical characteristics, it has a lower yield, probably due to greater difficulty in finding signs suggestive of liquid in the free cavity, due to mild traumas 20. Our results suggest an adequate performance, considering the common context of trauma in the Caribbean region and more exposed population, with only two false positive and three false negative, and only one dead patient, which was true positive.
Despite what has been previously described, the ease and usefulness of access to the tool cannot be omitted, since it is a complementary aid in the acute evaluation of trauma, especially in severe cases, where a probable diagnosis must be made to define surgical conduct. Considering that this is an operator-dependent tool, a possible solution would be a specialized and massive training that would allow residents to improve the accuracy of the use of portable tools in the management of trauma in the emergency department from their first years.
As limitations, it should be mentioned that this is a short report on the first experience reported in the literature on the use of E-FAST by general surgery residents in the Colombian Caribbean, being a single-center retrospective study without a control group, with a considerable risk of selection bias. However, it constitutes the first evidence for the design of future studies, which could evaluate specific problem questions in greater depth.

