











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Dengue fever is a tropical disease characterized by high fever and bleeding caused by the dengue arbovirus. It is transmitted by the bite of Aedes aegypti, of the flavivirus genus, a species largely found in territories below 1800 masl. According to the World Health Organization (WHO), dengue fever is the biggest public health issue in tropical and subtropical countries, accounting for more than 500 000 hospitalizations per year, with a mortality rate of 1% 1.
In 2012, 54 726 cases of dengue fever were reported in Colombia, of which 1 641 corresponded to severe dengue, and 25 174 to patients under 15 years of age, with a mortality rate of 3.9%. Such figures labeled the country as an endemic territory for dengue fever in the past years 2. Data on its incidence in obstetric population are not clear; however, a susceptibility condition related to the development of infections has been reported, as well as an increase in their severity. In addition, growing evidence on predisposition to the development of activation pictures and severe immune response has been found, especially in cases of Plasmodium falciparum and Listeria monocytogenes infections, and viral infections such as influenza A(H1N1) 3.
Recently, guided transfusion therapy techniques, such as thromboelastography, have been implemented in patients with critical illnesses to evaluate the different phases of coagulation and clot lysis. The reduction of morbimortality and the cost associated with health care, as a result of the decrease in the number of transfusions, have been described as the main advantages of their use 4. Although reports evidencing the usefulness of thromboelastography in sepsis 5 can be found, its clinical applicability in patients with dengue fever infection and hemorrhagic complications requiring administration of blood products is unknown to date.
Considering the facts exposed above, this article presents the case of a pregnant patient infected with dengue hemorrhagic fever, treated in a university hospital of Colombia. This patient underwent a transfusion therapy through thromboelastography with the purpose of controlling obstetric bleeding and avoiding pregnancy loss.
CASE PRESENTATION
Clinical findings
33-year-old woman, with no previous medical-surgical history, and eight weeks into her second pregnancy by the time she attends the emergency department. She reported a clinical picture of five days of repeated intermittent fever of 38.3°C, associated with chills, generalized myalgias, musculoskeletal, recto-ocular and headache pain, as well as nausea, asthenia, adynamia and abdominal pain.
She denies any history of trauma and vaginal or urinary tract infections. Likewise, she reported that, by the time of consultation, she was getting prenatal care and that no abnormality had been found. She also reported that seven days before the consultation she had been in an endemic region for multiple tropical diseases, a place located at 300 masl; further investigation revealed that she received multiple insect bites during the trip.
Calendar and diagnostic evaluation
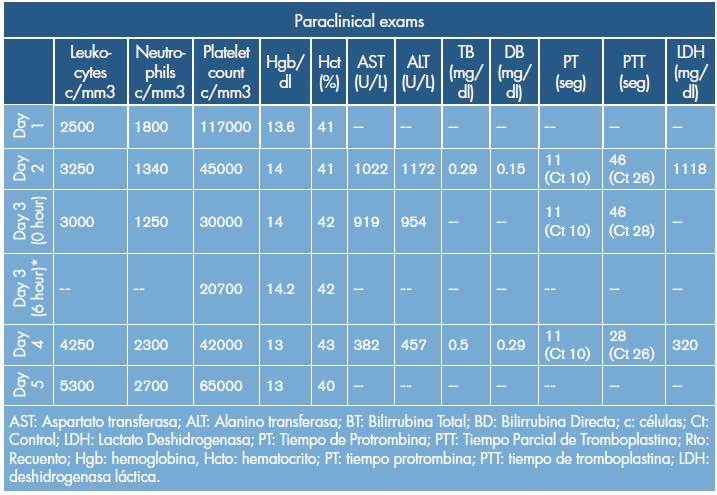
Based on clinical findings, a possible dengue virus infection was suspected and paraclinical tests were requested for admission (Table 1). Physical examination on admission did not show any lesion associated with hemorrhagic phenomena such as ecchymosis, petechia or hematoma. The only abnormal finding developed during her stay in the emergency room after presenting with an episode of acute, sparse and bright genital bleeding. Pelvic examination was omitted, and an obstetric ultrasound was performed, confirming fetal viability and the presence of a retroplacental hematoma of approximately 50%, which could be a sign of threatened abortion. Due to the risk of hemorrhagic complication, the patient was transferred to the ICU, where the dengue infection diagnosis was confirmed after obtaining positive IgG and IgM tests for dengue fever.
THERAPEUTIC MANAGEMENT
On the third day of hospitalization and facing an abrupt reduction of platelet count, a platelet transfusion was indicated and a thromboelastogram (TbEg) was performed to determine the coagulation status. TbEg reported R: 12.5, K: 13.0, alpha: 20.4, MA: 27.2 (Figure 1A). Furthermore, a control complete blood count taken six hours after the platelet transfusion yielded the following results: Hg: 14.4 g/dL, Hct: 42.3%, Polys: 50%, Lymphs: 40.1%, platelet count: 20 700 c/mm3. Taking into account the risk of miscarriage due to persistent vaginal bleeding, a transfusion of blood products was administered again, this time with platelets and fresh frozen plasma (FFP); phytonadione 10mg was initiated intravenously (IV). The control thromboelastograms requested within the next 24 hours are shown below (Figure 1A, B, C and D).
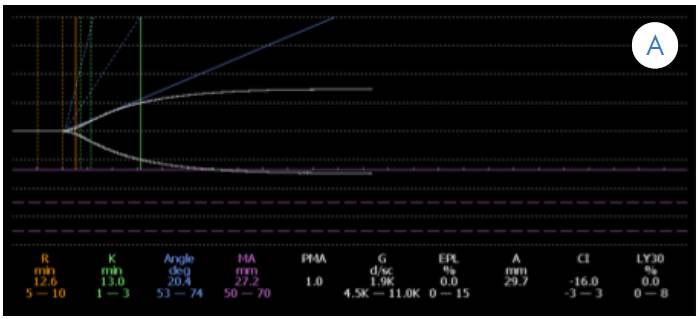
Figure 1 A. Initial thromboelastogram showing an anticoagulation pattern and deficiency of coagulation factors (prolonged k time, decreased alpha angle, and decreased maximum amplitude).
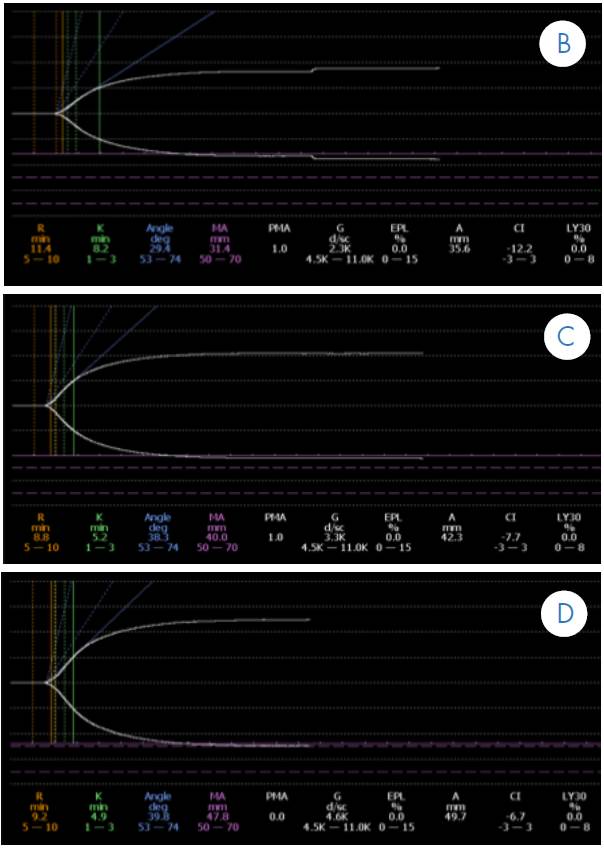
Figure 1 B. Control thromboelastogram (TbEg) # 1 done after the transfusion of platelets and of 10U FFP (gradual correction in K time values, alpha angle, and maximum amplitude). Figure 1 C. Control TbEg # 2 done after the second transfusion of platelet concentrate. Figure 1 D. Control TbEg # 3 done after the FFP transfusion (correction of K time, alpha angle, and maximum amplitude close to reference values).
Monitoring and evolution
During ICU stay, a positive IgM and IgG serum antigen for dengue fever was reported. In addition, the evolution of the patient was satisfactory, and no new episodes of bleeding occurred. On the sixth day of evolution of the disease and with TbEg in the correction phase, the patient was discharged from the ICU without complications. Multidisciplinary follow-up by obstetrics, infectology and psychology was indicated. Seven days after the discharge, an obstetric ultrasound was performed, which showed that retroplacental hematoma persisted with a 50% decrease of the original size and fetal viability.
DISCUSSION
The clinical presentation of dengue is broad and depends on the phases of the disease, which range between asymptomatic or febrile cases during the febrile phase (0-3 days), severe cases of bleeding, shock or organ dysfunction during the critical phase (3-6 days), and the resolution of symptoms in the convalescent phase (>6 days). Recently, a classification of this disease was made according to its clinical presentation to timely identify severe cases and establish proper treatment. Such classification is based on the presence or absence of warning signs and severe dengue states characterized by shock, bleeding or organ involvement such as myocarditis, hepatitis, encephalitis, and renal failure 6.
The risk of hemorrhagic dengue fever during pregnancy is determined according to the trimester in which it is contracted, and includes vaginal bleeding, threatened abortion, and abruptio placentae. In this regard, Carles et al. 7 determined an increased preterm delivery rate of 55% in French Guyana, which is similar to the findings reported by Poli et al. 8. Restrepo et al. 9 reported an increase in the incidence of threatened abortion and preterm delivery in patients with dengue hemorrhagic fever in Colombia.
A more recent study reports that 10% of cases show hemorrhagic events associated with maternal dengue infection, stressing that an association with retroplacental hematoma is observed during the first trimester 10. Evidence suggesting that there is no relationship between dengue and congenital malformations during the first trimester of pregnancy has been compiled. However, in India, Sharma & Gulati 11 have reported some cases of neural tube defects following a regional dengue epidemic, without finding associated chromosomal defects 11.
Most individuals who are infected and develop the disease, evolve to classic dengue fever, a self-limited febrile disease that usually does not represent any complication. Nevertheless, a variable amount of patients develop spontaneous bleeding, decreased platelet count and signs of plasma extravasation; all these manifestations define the dengue hemorrhagic fever.
Hemorrhagic manifestations have been reported in 35-50% of cases, the most common being epistaxis, gingivorrhagia, and gastrointestinal bleeding 12-13. Despite this trend, some authors, such as Chaudhary et al. 14, consider that there is no association between hemorrhagic manifestations and platelet count, although, this claim has not been confirmed yet due to the heterogeneity of patient selection. Deep thrombocytopenia may be strongly related to the severity of dengue in special populations such as children and pregnant women, for whom it is estimated in terms of major and minor bleedings and signs of plasma extravasation.
Discussions around transfusions, particularly about platelets, have been held regarding pregnant women. To date, no information has been published that could certainly associate abortion with dengue infection during the first trimester, whereas an association between the presence of a placental hematoma and the risk of miscarriage has been reported in 5 to 17% of losses in patients with hematomas, with an OR of 2.18 (1.20-3.67) 15-17.
Although multiple etiologic causes of retro-placental hematomas have been found, including fetal malformations, corpus luteum insufficiency, trauma and perinatal infections such as parvovirus and toxoplasmosis, they have also been reported in infections contracted at the uterine and systemic level 18. When considering the case presented here, it is possible to affirm that the placental hematoma was associated with a systemic viral infection, which worsens due to the presence of hematological dysfunction with severe thrombocytopenia.
In this context, there is no protocol to determine whether the correction of coagulopathy improves obstetric prognosis and reduces the risk of abortion. In a series of 53 patients, Basurko et al. 10 reported two cases of early abortion due to utero-vaginal bleeding and five hemorrhagic complications at the time of delivery. Another study by Chotigeat et al. 19 made a comparison between patients who were transfused platelets before delivery and patients who were not transfused, finding a reduction of associated bleeding events in the first group.
Thromboelastography assesses hemostasis from a functional point of view, and is represented by the interpretation of the cellular coagulation model. Its application in different clinical scenarios, especially in cardiovascular surgery patients and trauma patients, is a proper option to correct acute hematological alterations and to decrease the unnecessary use of blood products. 20. It is worth noting that conventional coagulation tests do not allow managing the underlying coagulation disorder, which often results in unnecessary replacement of blood components. Thus, thromboelastography allows physicians to recognize a coagulopathy and, more importantly, to understand the underlying coagulation disorder 20.
In this case, the alteration was determined at its full extent by using thromboelastography, which allowed transfusing platelets to correct this variable and to ensure adequate platelet function, therefore, resolving the vaginal bleeding. Although determining if this behavior was beneficial to the patient or if the resolution of vaginal bleeding and subsequent reabsorption of the hematoma could have been achieved only through resting and medical management of the viral infection symptoms can be further discussed, this report raises the possibility of including this treatment in the medical practice.
The literature does not provide records regarding the assessment of the performance and the usefulness of thromboelastography as a dynamic test to define the correctness of coagulopathy and, specifically, thrombocytopenia in patients with dengue hemorrhagic fever, as well as in pregnant patients with dengue fever. Its use has been reported in relation to other obstetric conditions, such as acute fatty liver of pregnancy 21, which is another reason to consider this report as relevant.
However, this reports also lacks information on other causes of placental hematoma, such as fetal malformations, which were not determined since the described clinical management was selected due to the gestational age of the patient and the acute course of the disease.
CONCLUSION
Patients with retroplacental hematoma and dengue fever infection associated with severe thrombocytopenia are at increased risk of miscarriage and fetal loss. In consequence, coagulopathy correction may improve pregnancy prognosis. Conventional coagulation tests may underestimate the risk of coagulopathy and increased bleeding secondary to hematoma. Thromboelastography may be a useful tool for identifying patients at high risk of bleeding due to severe thrombocytopenia in cases of dengue fever during pregnancy, so its use in institutions where this technology is available should be considered.

