











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Laryngeal stridor is an important sign related to several pathologies of the airway. When it occurs in neonates and is associated with respiratory distress, it must be treated urgently. One of its causes, although rare, is congenital laryngeal saccular cyst 1; however, differential diagnoses include more frequent pathologies such as laryngomalacia, tracheomalacia, subglottic stenosis, vocal cord paralysis, laryngocele, laryngeal membrane, among others 2.
Saccular cyst is a benign supraglottic lesion that is usually unilateral, does not have an opening to the laryngeal ventricle and is greater than 1cm 3. This lesion corresponds to 25% of all laryngeal cysts 4 and to 2-5% of all benign laryngeal lesions 5,6. Since this is a very rare pathology and there is no exact data on its incidence, although some authors state that it is 1.82 per 100 000 live births 7, while others state that it is less than 1 per 300 000 live births 8.
CASE PRESENTATION
Full-term newborn patient with adequate weight for gestational age, delivered via cesarean section and with polyhydramnios and APGAR 10/10. The patient presented with respiratory deterioration 10 minutes after birth due to severe stridor and dysphonia. Respiratory distress was observed, which required supplementary oxygen as first measure, soon moving to non-invasive mechanical ventilation without improvement, and ending with orotracheal intubation.
Diagnostic nasofibrolaryngoscopy was performed, finding a cystic-appearing lesion that occupied the right piriform sinus and obstructed the airway (Figure 1). Contrast computed tomography (CT) of the larynx with 3D reconstruction under sedation was requested to assess the extension of the lesion. A right cystic-appearing lesion (1.3x1.2x2.1cm) was observed, which compromised the hypopharynx, pyriform sinus, glottis and right supraglottic space, and caused loss of definition of laryngeal ventricle and right vocal structures with wall enhancement (Figure 2). Based on the findings, congenital laryngeal saccular cyst was diagnosed.

Source: Own elaboration based on the data obtained in the study.
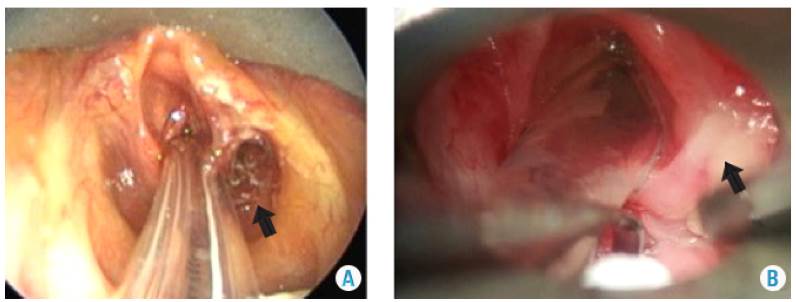
Figure 1 Nasofibrolaryngoscopy with cystic image on the right aryepiglottic fold, extended towards the ipsilateral piriform sinus and laryngeal ventricle.

Source: Own elaboration based on the data obtained in the study.
Figure 2 Contrast coronal CT scan of the neck showing a cystic lesion extending from the piriform sinus to the trachea with a significant decrease in the caliber of the airway.
Surgical approach was performed by means of microlaryngoscopy and endoscopic resection of the laryngeal lesion with radiofrequency (laryngeal electrode tip MC/AC/BC 403, 100-300V, 100-500 kHz). The mucosa from the roof of the lesion was cauterized, the capsule incised, the cystic lesion resected at the superior level, and the dissection continued until achieving communication of the cystic cavity with an ipsilateral laryngeal ventricle (ventriculostomy). Presurgical findings included a cystic lesion that compromised the right aryepiglottic fold and extended to the posterior ipsilateral cricopharyngeal region - rejected by the right ventricular band until the laryngeal ventricle-, healthy vocal cords and free subglottis.
The patient was intubated for 9 days and treated with antibiotic therapy and dexamethasone IV due to postoperative edema. On day 10, adequate extubation tolerance was achieved. Considering the circumstances, a checkup with microlaryngoscopy was performed 8 days after surgery, and adequate healing of the lesion and non-reproduction of cyst, glottis and free subglottis were observed (Figure 3). A postoperative control was performed after a year using nasofibrolaryngoscopy without new surgical interventions, no recurrence of the cyst, and adequate epithelization and laryngeal development.
DISCUSSION
The saccular cyst consists of a dilation of the laryngeal ventricle filled with mucus that does not communicate with the laryngeal lumen 9. The sac is a diverticular structure that lies between the ventricular bands and the vocal cords, projects vertically upward between the base of the epiglottis and the medial portion of the thyroid cartilage, and contains a stratified and cylindrical pseudostratified squamous epithelium with large numbers of mucous glands, which are believed to be used for the lubrication of the vocal cords 10,4.
The main symptom of this pathology is stridor at birth that can conceal laryngomalacia or congenital vocal cord paralysis, which appear with stridor in the first weeks of life 11. Other symptoms depend on the size of the lesion and its location; for example, dysphagia may occur if the cyst occupies the hypopharynx 12 or if there is progressive respiratory distress until total airway obstruction, cyanosis, apnea, hoarse cry and low-pitched cry, especially with changes of position or agitation. If the cyst is on the right side, the symptoms are accentuated in the contralateral ulnar position 4.
Two types of saccular cysts are described in the literature: anterior and lateral. Anterior cysts are characterized by a submucosal mass dependent on the false vocal cord that protrudes through the anterior portion of the ventricle, while lateral cysts, usually the most common, occupy the entire ventricular band and exit the pharynx through the mucosa of the aryepiglottic fold 13.
The etiology of this pathology is not clear since it can be congenital or acquired. The first is caused by obstruction or atresia of the sac, which, depending on its location, will make the cyst more extensive or not. This obstruction can be caused by the abnormal migration of the tissue from the fourth branchial arch generating the cystic formation 14 or by the isolation of the cells of the sac due to the abnormal migration of mesenchymal cells through persistent fetal vessels in the larynx. The second may be a consequence of sac obstruction secondary to neoplasia, trauma or inflammation with subsequent fibrosis 15.
Most of the literature found on congenital saccular cyst is based on case reports; in the most extensive study, data on 20 cases were collected in a period of 15 years 16, which makes the low incidence of this pathology evident. This study found that the incidence in the Hospital Infantil Universitario de San José in the last 5 years has been 1 for every 22 318 live births. Most of the cysts are lateral with an average size of <3cm, as the one described in this article 3,7.
Diagnosis can be made through imaging studies such as lateral radiography of soft tissues of the neck, where a sac full of mucus is visualized in the supraglottic region; using CT or nuclear magnetic resonance is also possible. Several authors state that diagnostic confirmation is achieved through direct visualization of the lesion, either by direct or optical fiber laryngoscopy 17,15, as described here.
The treatment of this pathology is mainly surgical and includes the aspiration of the cystic content with needle and marsupialization, and even cyst excision via endoscopy or external approach 17,18. The first two are considered insufficient treatments because, in the first case, the mucosa glands of the cyst continue to secrete mucus, thus generating reappearance, and in the second, multiple procedures are required due to cyst recurrence that can easily generate laryngeal stenosis with subsequent tracheotomy 8,19. The excision of the cyst by microlaryngoscopy and external approach are the treatments with the highest success rates according to the literature. However, some authors, such as Ward et al.12, recommend resection by means of an external approach as the only definitive and safe treatment for the non-formation of laryngeal stenosis, given the poor manipulation of the laryngeal mucosa.
There are case reports such as Khodaei et al.17 and Danish et al.5 which establish microlaryngoscopy with CO2 laser as the first line of management and the most used treatment. Lateral cervicotomy through the thyroid membrane is used for complex, recurrent or> 3cm cysts, since they can increase anesthesia time and pose a higher risk of superior laryngeal nerve injury 8,19,20. Another endoscopic approach that has shown lower morbidity is CO2 laser vestibulectomy, since it reduces surgical time, avoids vascular or superior laryngeal nerve damage and accelerates tissue recovery. 20.
The definitive management, as stated in the literature, is microlaryngoscopy, since most reports and case series use CO2 laser for endoscopic resection 3,19,20. In Colombia, this laser is not available in all hospitals, so the procedure, in this case, was performed using radiofrequency. Of all the articles reviewed, only the series by Kumar et al.16 used this resection method and demonstrated that it is safe and effective because it improves surgical precision and the healing time of the mucosa, minimizes bleeding in the surgical site, preserves the surrounding tissues, and only 1 of 6 cases require a second surgery 16. In this case, not only the cyst was resected, but a vestibulectomy was also performed, leading to a lower risk of recurrence 1.
Despite the low frequency of this pathology, it is important to know and be able to diagnose and treat it safely and effectively with the resources available in most hospitals in Colombia. This is useful to avoid significant compromise of the patient's airway.

